
Article Figures & Data
Figures
- Fig 1.
Typical supratentorial right frontal cPML in an HIV-positive patient. A, On DWI, the lesion shows typical restricted diffusion along the advancing edge posteriorly (arrows) and facilitated diffusion centrally. B, On the ADC map, ADC value is low at the posterior advancing edge (arrow) and high at the center of the lesion. C, The lesion typically involves the subcortical U-fiber and is hypointense (relative to gray matter) on the T1-weighted sequence. Note the absence of mass effect from this moderate-sized lesion. D, There is no enhancement of the lesion on the postcontrast T1-weighted sequence. E, On the FLAIR sequence, there is hyperintensity in most parts of the lesion. Note the inversion of the FLAIR high signal anteriorly (arrow) due to intralesional cystic change. F, On the T2-weighted sequence, the entire lesion is hyperintense. Note the adjacent anterior cortex is relatively spared (arrow). G, On perfusion imaging, cerebral blood volume of the lesion is lower (arrow) than that of the contralateral white matter.
- Fig 2.
Typical infratentorial cPML in another HIV-positive patient classically involving the middle cerebellar peduncle (left). A and B, This lesion also has diffusion restriction at the anterolateral advancing edge (high DWI signal intensity and low ADC value, arrows) and diffusion facilitation at the center as evidenced by the DWI (A) and the ADC map (B). C and D, The lesion shows typical hypointensity on the T1-weighted sequence (C) and hyperintensity on FLAIR (D). Note, there are no mass effect. There is no enhancement in the postcontrast T1-weighted sequence (E).
- Fig 3.
There is an incomplete rim of T1 hyperintensity (arrows) at the advancing edges of the supratentorial (A) and infratentorial (B) cPML lesions.
- Fig 4.
Progression of cPML. A and B, These FLAIR images, 4 months apart, from an HIV-positive patient with cPML demonstrate typical progression of the supratentorial white matter FLAIR hyperintensity.
- Fig 5.
A, Intralesional microcyst on T2-weighted sequence on the left parietal cPML lesion in an HIV-positive patient, zoomed up in the inset. The arrow points to a microcyst. B, There are 2 intralesional microcysts (arrows) in this right fronto-parietal cPML lesion in another HIV-positive patient.
- Fig 6.
Typical disease course of cPML in an HIV-positive patient receiving HAART. Top panel, a set of images at presentation with focal diffusion restriction (A and B) and very subtle but typical hypointensity on T1 (C) and hyperintensity on FLAIR (D). This initial study was confused with acute subcortical infarction. Middle panel, a set of images 1 month after the initial presentation. No HAART was administered before this scanning. Now the lesion has enlarged in size with typical diffusion restriction (arrows) at the medial and posterior advancing edges (E and F). Now the T1 hypointensity is more obvious (G). The adjacent cortex is not involved (arrows). Typically the lesion is hyperintense on FLAIR (H). Bottom panel, a set of images 19 months after initial presentation. The patient received HAART for 18 months. Now there is no diffusion restriction (I). On the T1-weighted sequence (J), there is profound T1 hypointensity associated with new/progressive atrophy. There is FLAIR hyperintensity in the adjacent areas. However, the main lesion is not hyperintense on FLAIR (K). On T2 (L), the lesion itself is very hyperintense compared with the adjacent white matter, suggesting cystic encephalomalacia. Note that the adjacent cortical architecture is preserved.
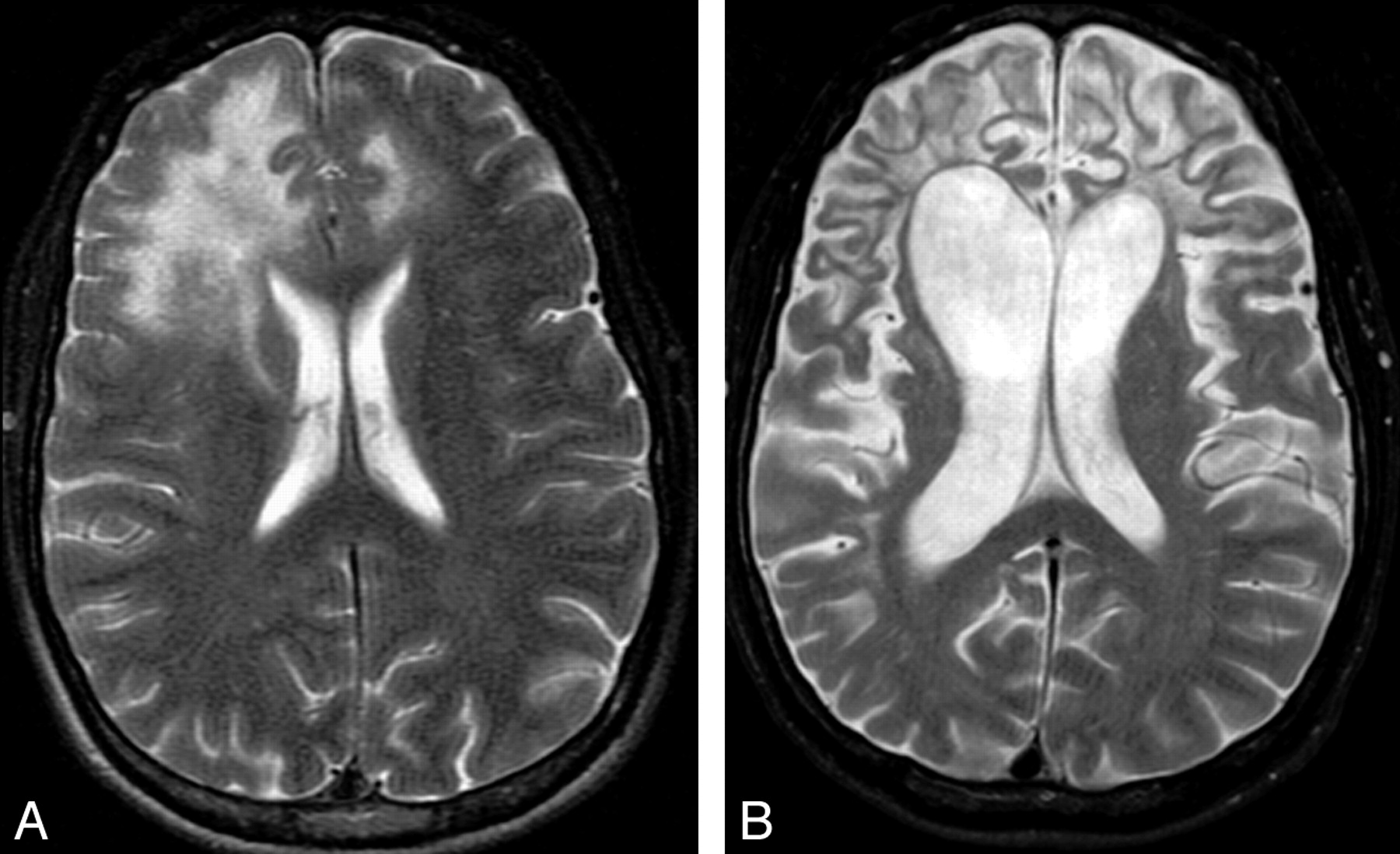
- Fig 7.
Sequel of cPML. A and B, The 2 T2-weighted sequences, 16 months apart, from an HIV-positive patient demonstrate prominent brain atrophy with dilation of the ventricles and prominence of the sulci. Even at this advanced stage, there is minimal cortical involvement.







Tables
Types of PML Clinical Presentation Imaging Appearance Histopathology cPML Focal neurologic signs depending on the location of lesions T1 hypointense (to white matter) and T2 hyperintense (to gray matter) lesions in the subcortical U-fiber rather than in periventricular white matter; diffusion restriction at the margin; no enhancement Severe demyelination; swollen oligodendrocytes with enlarged densely basophilic nuclei filled with eosinophilic inclusion bodies; bizarre astrocytes; absent/minimal inflammation iPML iPML in IRIS presents with aggravated cPML symptoms; iPML in the non-IRIS setting has similar or aggravated cPML symptoms Peripheral or rim enhancement with or without mass effect and vasogenic edema Similar to cPML plus marked inflammatory reaction characterized by diffuse or focal perivascular mononuclear cell (mainly CD3) infiltration JCVGCN Cerebellar symptoms including ataxia and dysarthria MR findings are negative in early stage; isolated cerebellar atrophy with T2 hyperintensity in later stage of the disease Isolated infection of the cerebellar granule cell neurons sparing oligodendrocytes JCM Similar to viral meningitis No specific imaging finding CSF positive for JCV DNA JCE Abnormal higher CNS function without focal neurologic deficit Predominant cortical T2 hyperintensity with involvement of white matter in later stage of the disease Extensive infection of the pyramidal cell neurons with meager infection of oligodendrocytes Diagnosis Typical Clinical Feature Typical Imaging Feature CSF JCV DNA Typical Histopathology with Demonstration of JCV DNA/Protein Definite PML + + + − Definite PML + + − + Presumptive PML + + − − -
Note:—+ indicates present; –, absent.
-
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- Abbreviations
- Epidemiology: Population at Risk
- Pathogenesis
- Clinicopathologic Syndromes of CNS JCV infection
- IRIS and NIRIS
- Diagnosis
- Imaging
- Diffusion Imaging
- Magnetization Transfer Imaging
- Spectroscopy
- Perfusion Imaging
- Angiography
- Nuclear Imaging
- Signs of Disease Progression
- Can Imaging Monitor Treatment?
- Can Imaging Predict Prognosis?
- iPML
- JCVGCN
- JCM
- JCE
- Treatment
- Conclusions
- References
- Figures & Data
- Info & Metrics
- Responses
- References
Related Articles
Cited By...
- Rhombencephalite chez une femme de 86 ans atteinte de leucemie lymphoide chronique
- Rhombencephalitis in an 86-year-old woman with chronic lymphocytic leukemia
- Clinical Reasoning: A 71-Year-Old Man With Horizontal Gaze Palsy, Anarthria, and Quadriparesis
- Clinical Reasoning: A 52-year-old woman with 3 weeks of progressive gait ataxia and dysarthria
- Neuroimmune Axes of the Blood-Brain Barriers and Blood-Brain Interfaces: Bases for Physiological Regulation, Disease States, and Pharmacological Interventions
- Punctate pattern: A promising imaging marker for the diagnosis of natalizumab-associated PML
- Brain Magnetic Susceptibility Changes in Patients with Natalizumab-Associated Progressive Multifocal Leukoencephalopathy
- Unusual Case of Progressive Multifocal Leukoencephalopathy After Allogeneic Hematopoietic Stem-Cell Transplantation
- CNS-Immune Reconstitution Inflammatory Syndrome in the Setting of HIV Infection, Part 1: Overview and Discussion of Progressive Multifocal Leukoencephalopathy-Immune Reconstitution Inflammatory Syndrome and Cryptococcal-Immune Reconstitution Inflammatory Syndrome
- Cranial nerve involvement in infratentorial progressive multifocal leukoencephalopathy
- Progressive multifocal leukoencephalopathy in a patient with transitory lymphopenia