
Article Figures & Data
Figures
- Fig 1.
A, Coronal drawing demonstrates the basic anatomy of the BPL. B–D, Oblique sagittal drawings (B–D from medial to lateral) demonstrate 3 parts of the BPL. The supraclavicular plexus is composed of roots and trunks. Roots are seen at the interscalene triangle between the anterior and middle scalene muscles. The subclavian artery forms the floor of the interscalene triangle (B). Roots then form the trunks at the lateral border of the middle scalene muscles. The retroclavicular plexus is composed of divisions situated in the costoclavicular space between the first rib and clavicula, and the BPL is seen in the superior and posterior aspect of the subclavian artery (C). The infraclavicular plexus is composed of cords and terminal branches located in the retropectoralis minor space. The BPL is situated in the posterior and superior aspect of axillary artery (D). The subclavian artery and vein take the name of axillary artery and vein at the lateral border of first rib.
- Fig 2.
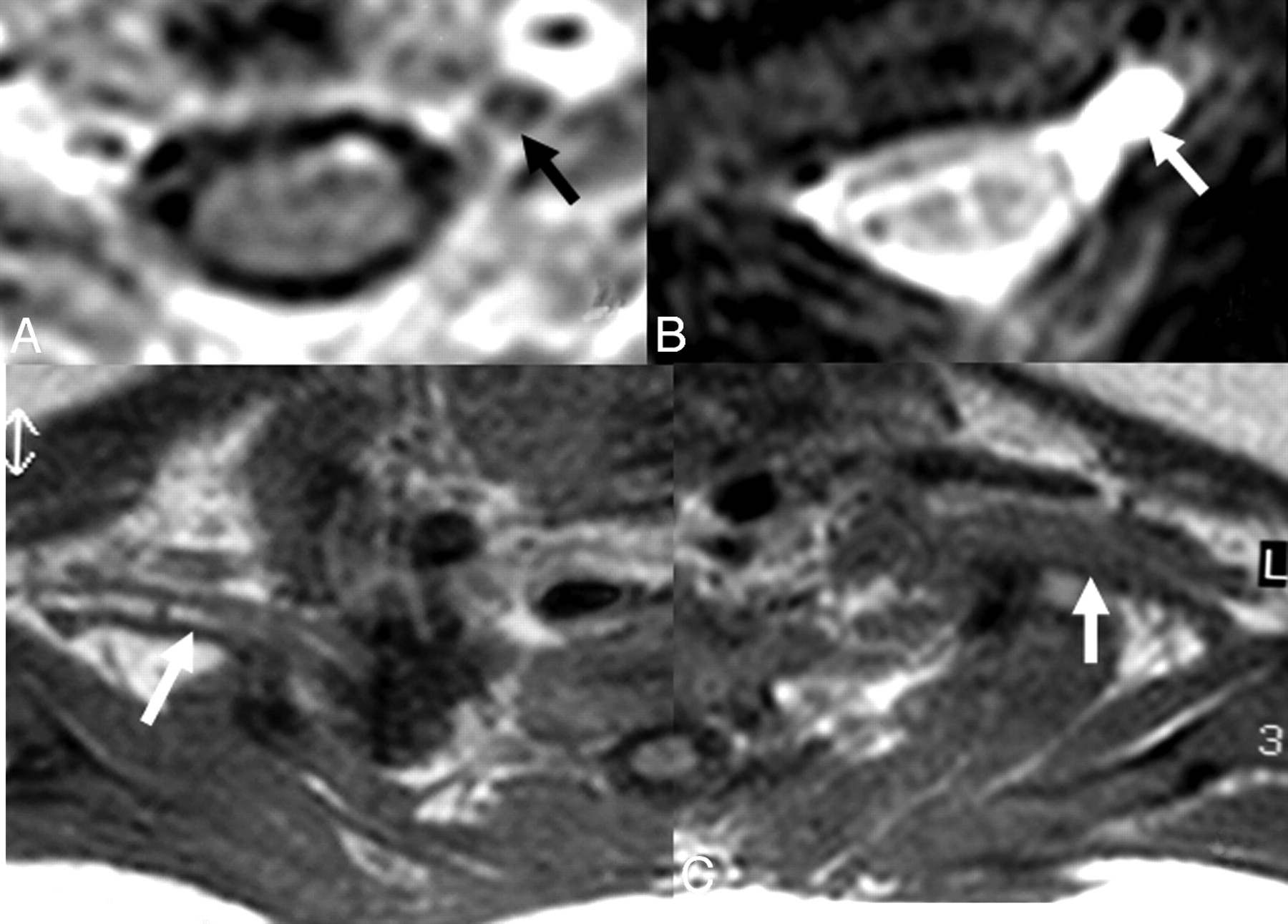
A and B, In a 1-month-old infant with a history of difficult birth, contrast-enhanced axial T1-weighted (A) and axial MR myelography (B) views show avulsion of the left C5 anterior root with contrast enhancement at its root stump (A) and a pseudomeningocele (arrows), consistent with preganglionic injury. C, Distal to the injury, the BPL on the left appears thickened and irregular on axial T1WI images compared with the BPL of the normal right side (arrows).
- Fig 3.
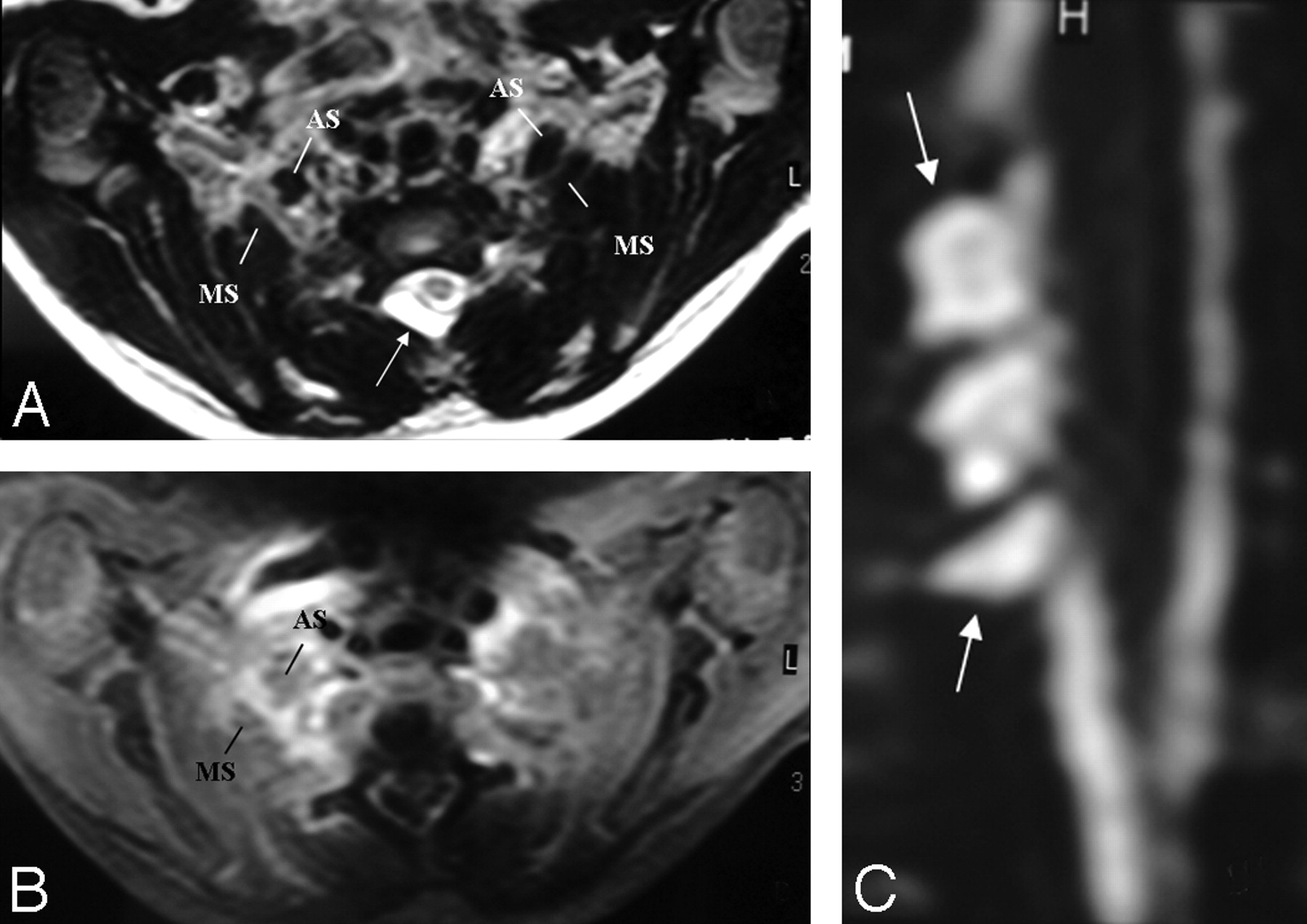
A and B, There is asymmetric thickening, T2 hyperintensity, and contrast enhancement of the right BPL compared with that of the left side, better seen between the anterior and middle scalene muscles. The pseudomeningocele is noted at the right posterolateral aspect of the central canal on axial T2-weighted TSE image (arrow, A). C, However, a coronal reformatted image from MR myelography shows the roots intact within the pseudomeningocele sac (arrows), suggesting only a traction injury. There is neither asymmetric enhancement nor T2 signal-intensity change of the BPL-innervated muscles or paraspinal muscles to support preganglionic injury.
- Fig 4.
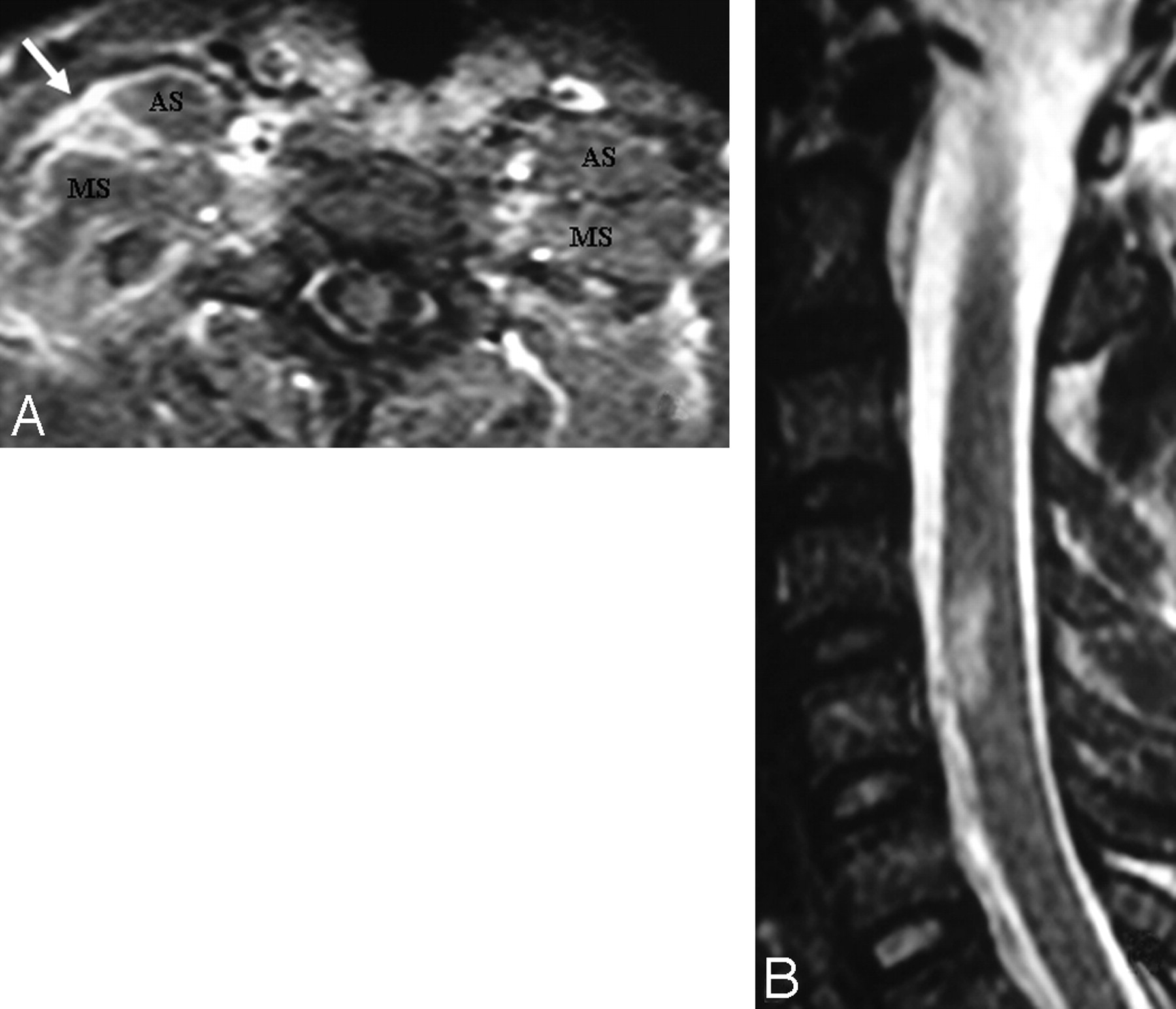
A, In a patient with a right-sided scapula fracture and monoparesis following trauma, the right BPL (arrow) is thickened and asymmetrically enhancing at the truncus level between the anterior and middle interscalene muscles. There is no associated root avulsion or pseudomeningocele, suggesting only traction injury at first glance. B, However, the presence of an expansile spinal cord lesion at the C4-C5 level could signal the possibility of preganglionic injury.
- Fig 5.
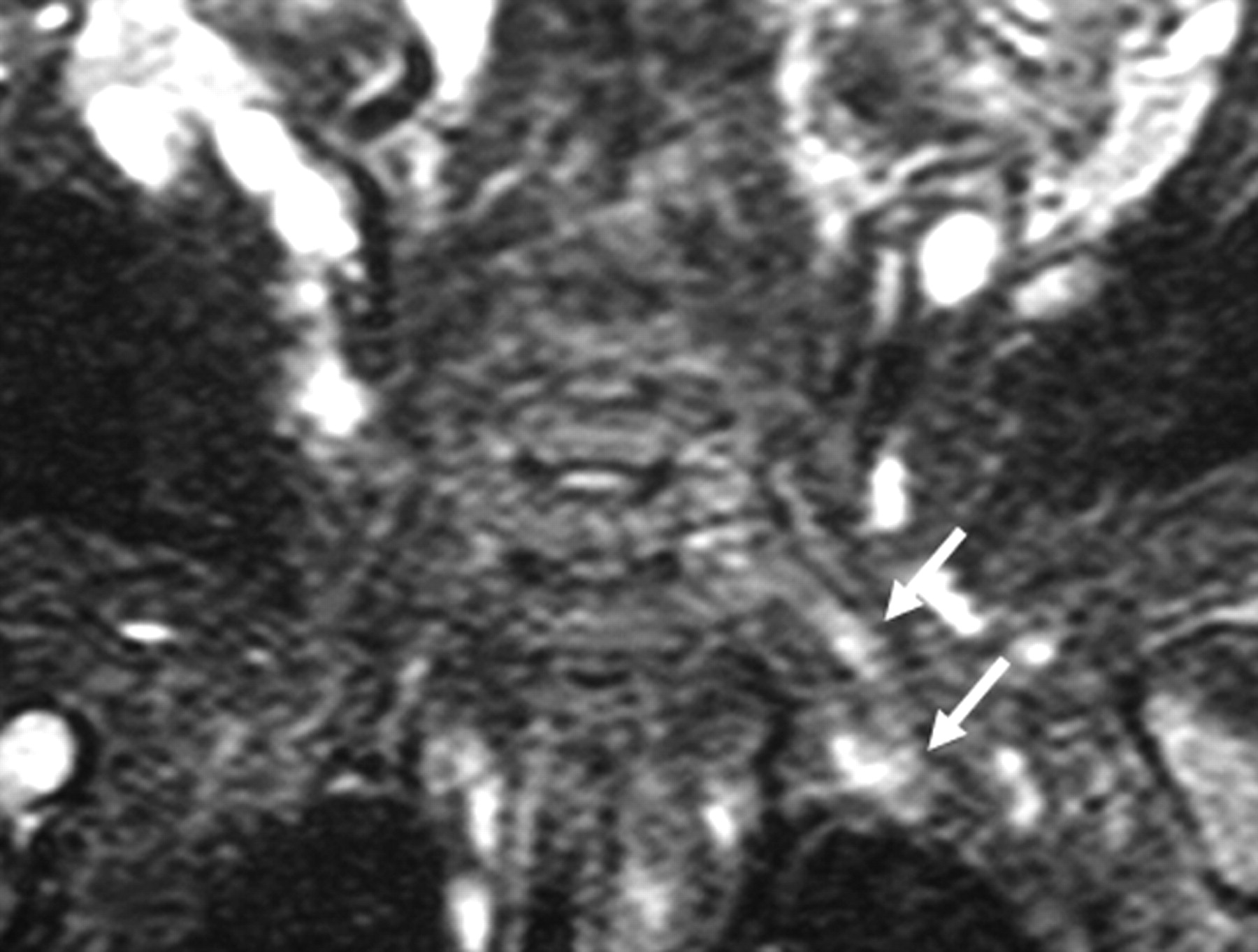
In another infant with a left-sided BPL paralysis following birth trauma, there is only hyperintensity of the left BPL on the coronal STIR T2-weighted image (arrows) without thickening on T1-weighted and T2-weighted TSE images (not shown). There is no associated root avulsion and pseudomeningocele. Findings are suggestive of traction injury.
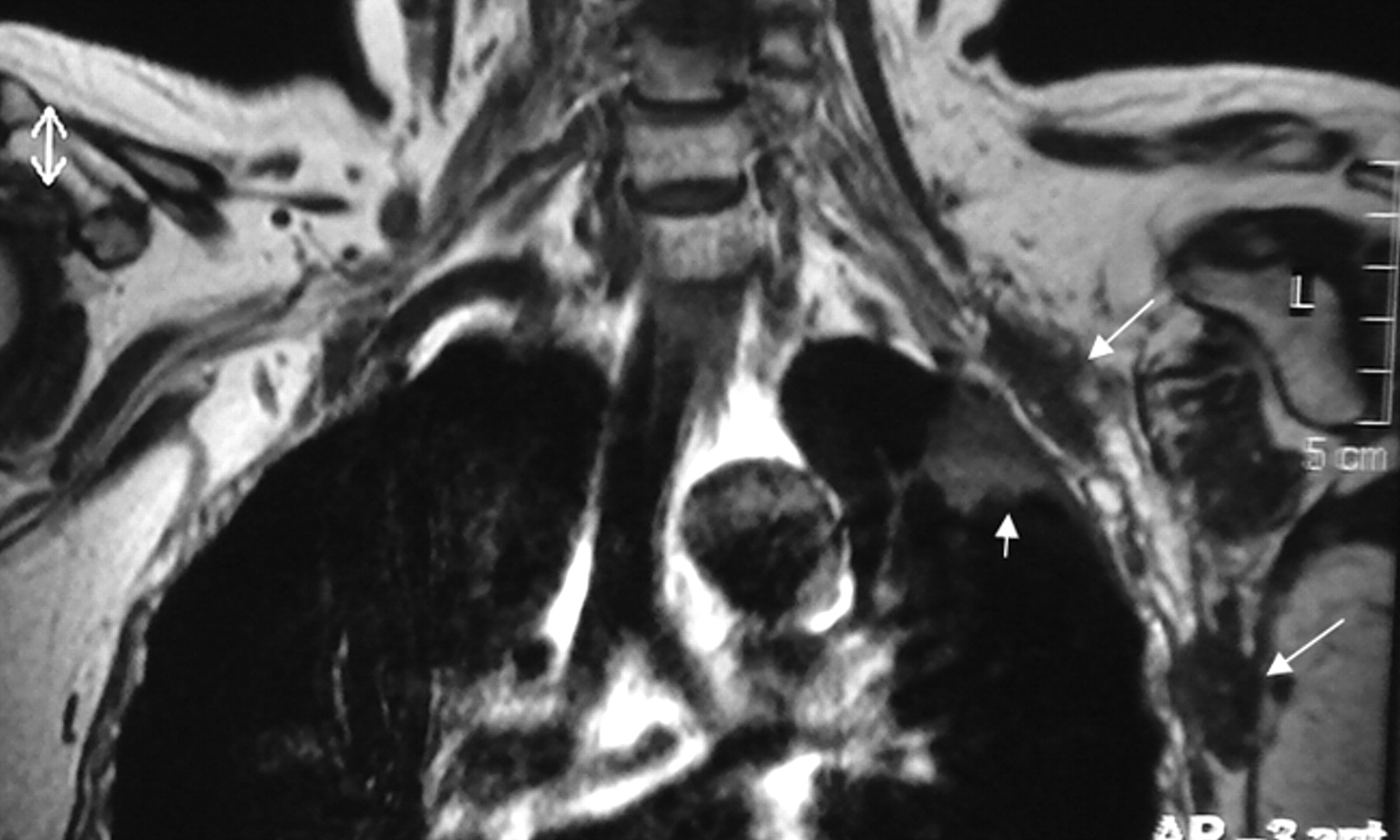
- Fig 6.
A Pancoast tumor surrounds the subclavian artery (arrow) circumferentially. The subclavian vein is not seen as separated. This finding means that it is either compressed or invaded. The BPL posterosuperior aspect of the subclavian artery is invaded as well.
- Fig 7.
Precontrast coronal T1-weighted view shows metastatic nodules (long arrows) from breast cancer in the vicinity of the left BPL and another metastatic mass in the upper lobe of the left lung (small arrow).
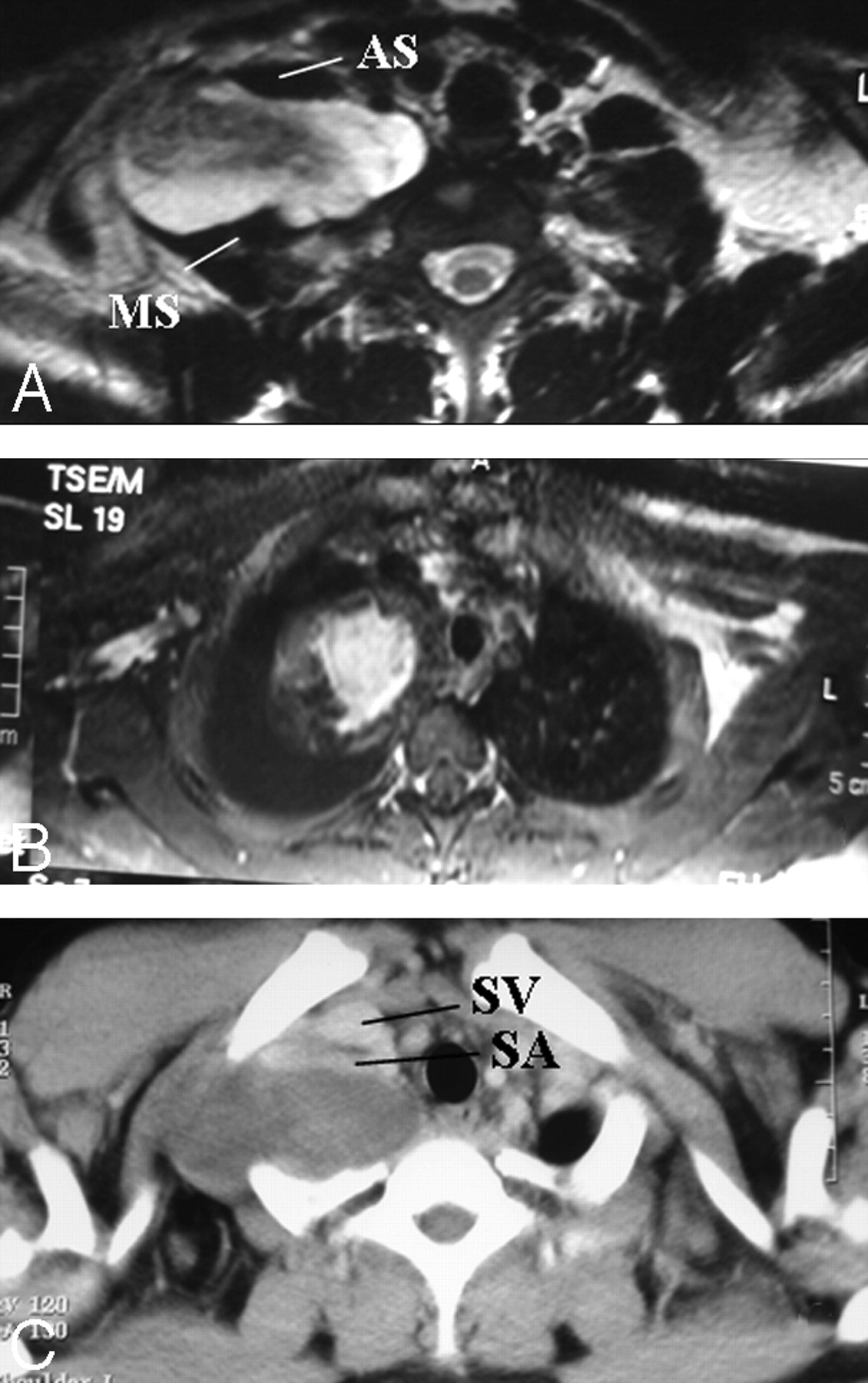
- Fig 8.
A and B, Pathologically proved neurofibroma elongating between the anterior and middle scalene muscles. The mass lesion is fusiform, longitudinally oriented along the BPL (A), with central homogeneous enhancement (B). A target sign with central hypointensity and peripheral hyperintensity on T2WI (A) and central homogeneous enhancement (B) are suggestive of neurofibroma. C, The subclavian vein and artery are extended at the anterior aspect of the mass on the axial postcontrast CT view. There is diaphragm paralysis on the right side compatible with phrenic nerve involvement as well (not shown).
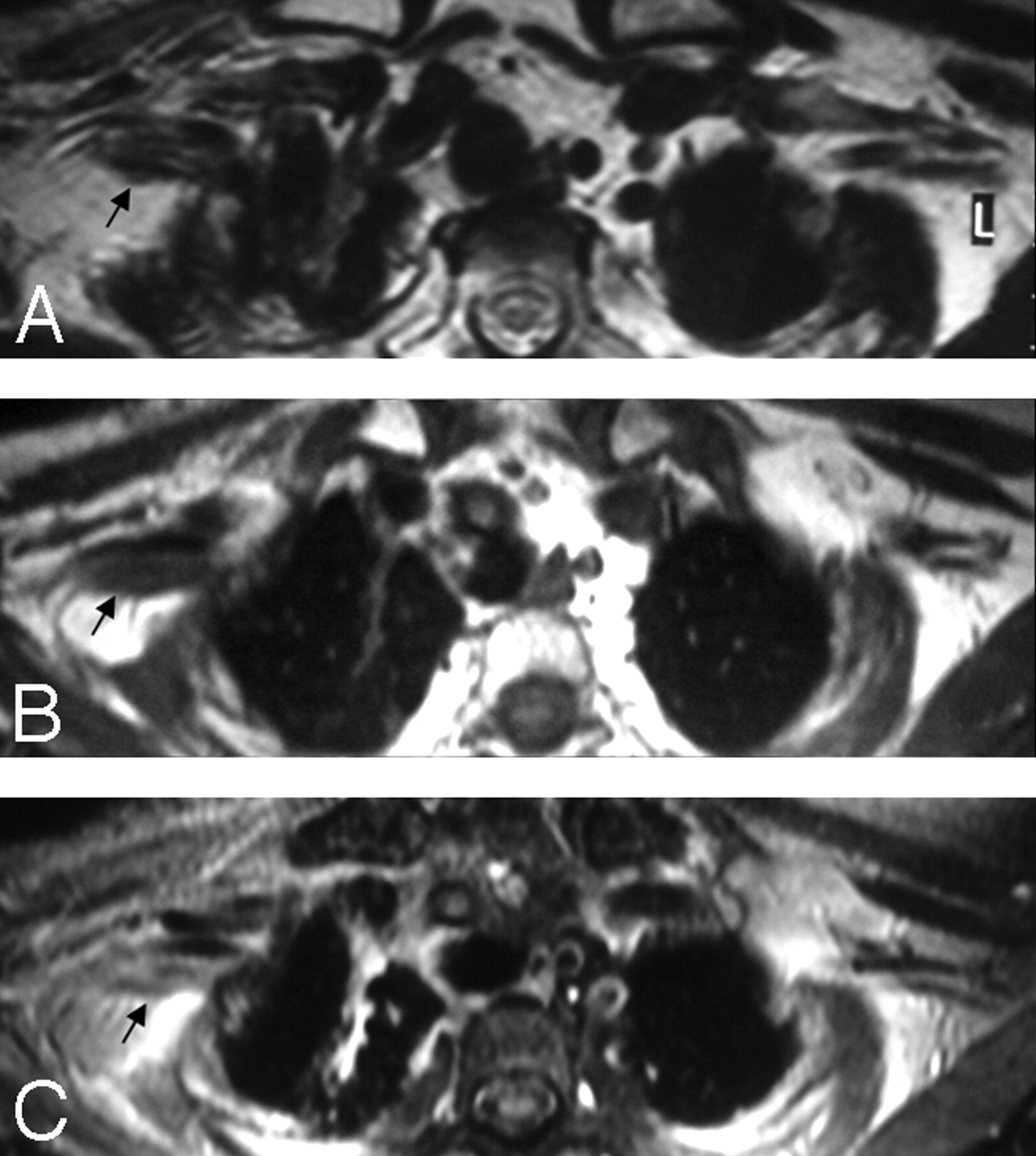
- Fig 9.
A, In a patient with a history of breast cancer surgery and radiation treatment with right-arm weakness, axial T2WI shows diffuse thickening of the right PBL with no associated hyperintensity (arrow). B and C, Pre- (B) and postcontrast (C) axial T1WIs show minimal contrast enhancement of the thickened right BPL fibers with no associated nodularity (arrows). Findings are suggestive of radiation fibrosis rather than metastasis.
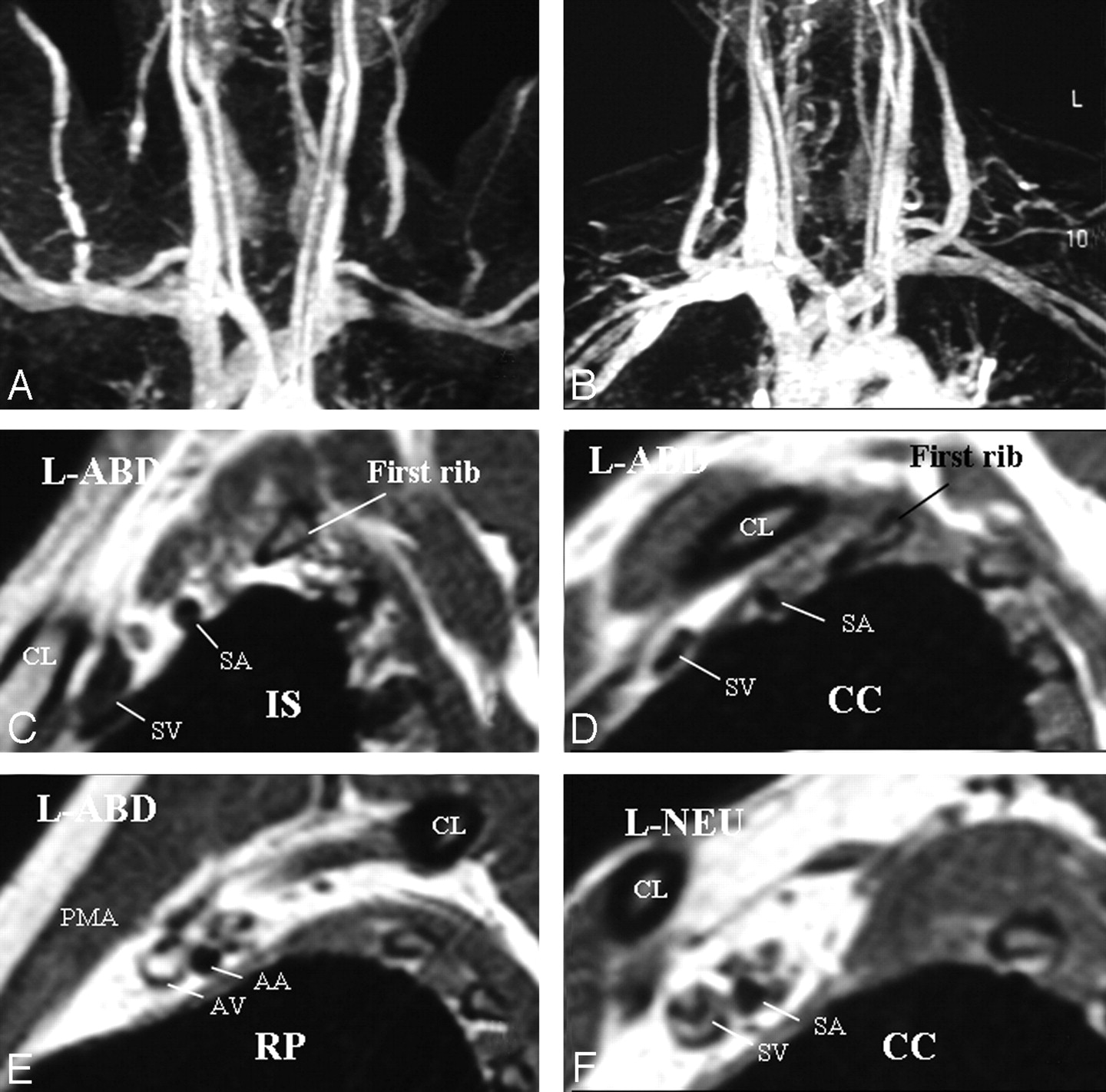
- Fig 10.
A, Left-sided neurogenic, arterial, and venous TOS with compression in the costoclavicular space in a patient with bluish discoloration of the left hand. MRA and MRV in abduction show impingement on the left subclavian artery and vein. B, In a neutral position, impingements on the vessels are all resolved. C–E, Sagittal views through the left BPL in abduction show narrowing of the subclavian artery and vein in the costoclavicular space and a normal caliber of the vessels in the interscalene triangle and retropectoralis minor spaces. In abduction, the left BPL is also squeezed in the costoclavicular space, suggesting neurogenic TOS additionally. F, In the neutral position, there is neither narrowing of the vessels nor any impingement on the BPL nerves in the costoclavicular space of the left side.
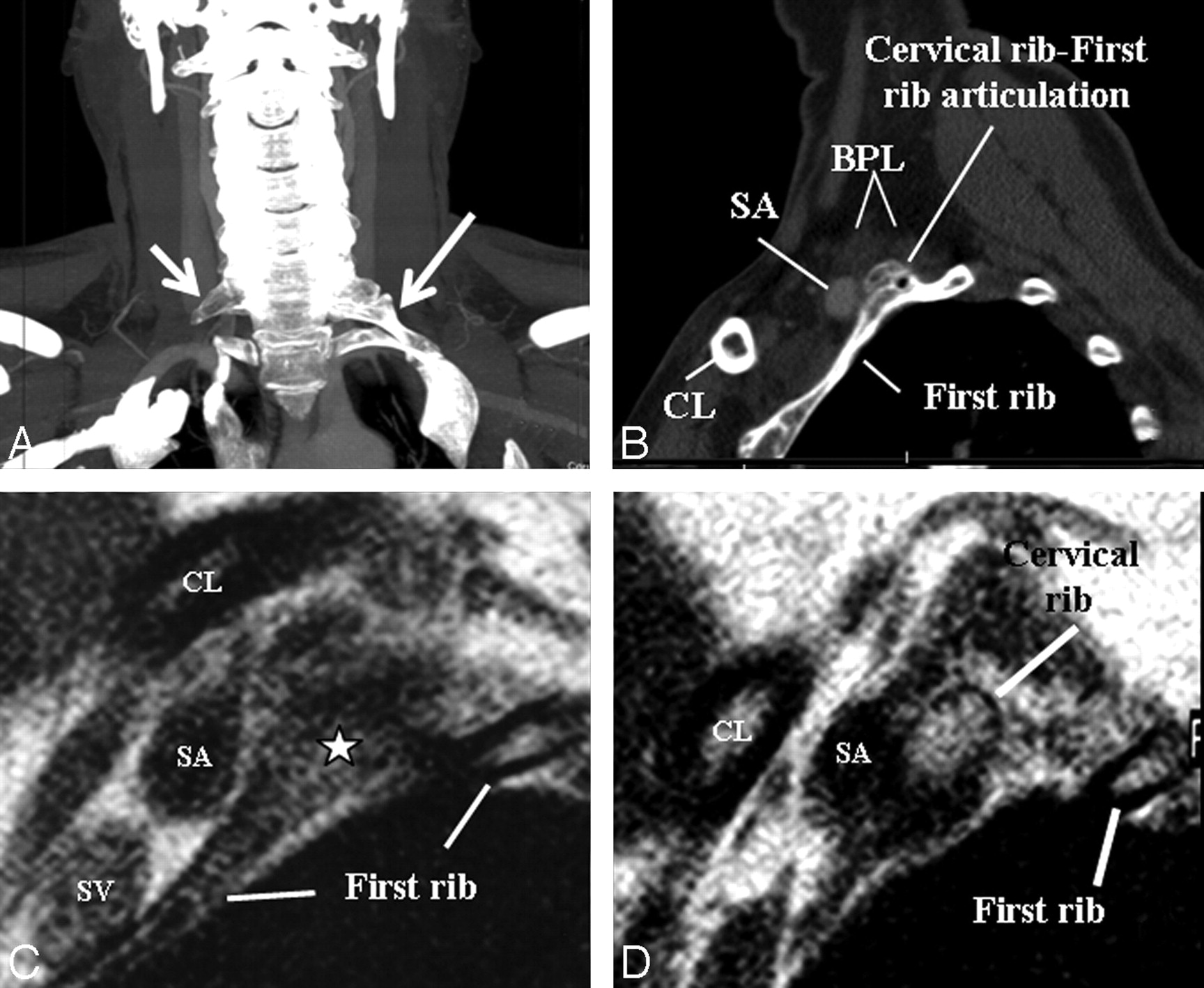
- Fig 11.
A, An elongated C7 transverse process on the right (small arrow) and a cervical rib (long arrow) articulating with first thoracic rib on the left on a maximal-intensity-projection view of a neck CT of a patient presenting with cervical pain and bluish discoloration of both hands, more so on the left. MRA and MRV of the neck vessels (not shown) in abduction did not show any stenosis excluding vascular (arterial or venous) TOS. B–D, Sagittal CT (B) and sagittal MR imaging (C and D from lateral to medial) views in a neutral position on the left side demonstrate cervical rib−first rib articulation (star) and the cervical rib contacting the BPL fibers in the costoclavicular space, responsible for neurogenic TOS. The patient's symptoms on the right are due to the elongated C7 transverse process impinging the BPL within the interscalene triangle (not shown).











Tables
MR imaging sequences obtained in brachial plexopathy with/without TOS
MR Imaging Sequences Associated Anatomic Structures or Pathologic Conditions Sagittal TSE T2WI through cervical spine Spinal cord lesion (edema, hemorrhage, avulsion, myelomalacia, syrinx, tumor, etc) Precontrast axiala T1WI BPL (thickening, nodularity) Precontrast coronalb T1WI BPL, vertebrae, long C7 transverse process, cervical rib Axiala 2D TSE T2WI BPL (thickening, nodularity, signal changes better seen between anterior and middle scalene muscles), radiculopathy, diskopathy, foraminal invasion, spinal cord lesions, large-sized pseudomeningocele, muscle denervation Coronalb STIR T2WI BPL (any signal changes not detectable on 2D TSE T2WI, especially in traction injuries and brachial plexitis), muscle denervation in traumatic injury, and brachial plexitis Axiala 3D TSE heavily T2WI (MR myelography) Root avulsions, small-sized pseudomeningocele, which can be missed on 2D TSE T2WI. Postcontrast fat-saturated axiala T1WI BPL (contrast enhancement), contrast enhancement of root stump or intradural roots or denervated muscles in preganglionic injuries Postcontrast coronalb T1WI BPL (contrast enhancement) Sagittalc,d T1WI from the symptomatic side in abduction Compression on BPL and subclavian vessels (positional, cervical rib, long C7 transverse process, accessory muscles, fibrous band) Sagittalc,d T1WI from the symptomatic side in neutral if there is compression Resolution of compression on the BPL and subclavian vessels MRAc and MRVc of subclavian artery and vein in abduction Subclavian artery and vein (patency, thrombosis, aneurysm, any impingement on the vessels) MRAc and MRVc of subclavian artery and vein next day in neutral if there is impingement Resolution of impingement on the subclavian vessels a Perpendicular to the long axis of the vertebrae in the coronal plane.
b Parallel to the long axis of the lower cervical vertebrae of C4-C7.
c Additional MR imaging sequences obtained when there is clinical suspicion of TOS.
d Perpendicular to the long axis of the BPL from the spinal cord to the medial border of the humerus.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}