
Abstract
BACKGROUND AND PURPOSE: Aneurysm geometry has been shown to predict the need for adjunctive techniques in the endovascular treatment of intracranial aneurysms. We conducted a systematic retrospective study examining which thresholds of dome-to-neck ratio, maximum neck width, and aspect ratio of intracranial aneurysms best predict the need for adjunctive techniques in endovascular management.
MATERIALS AND METHODS: One hundred seventy-five consecutive patients who were selected for attempted embolization of 185 intracranial aneurysms were included in this study. Aneurysm dome-to-neck ratio (maximum dome width/maximum neck width), maximum neck width, and aspect ratio (dome height/maximum neck width) were measured on 2D digital subtraction angiography. Statistical analysis was conducted to determine which thresholds of dome-to-neck ratio, maximum neck width, and aspect ratio were most predictive of the need for adjunctive devices in endovascular management of these aneurysms.
RESULTS: We demonstrated that 75% of aneurysms with dome-to-neck ratios >1.6 (P < .0001), 75% of aneurysms with aspect ratios >1.6 (P < .0001), and 70% of aneurysms with neck diameters <4.0 mm (P < .0001) did not need adjunctive techniques in their management. Adjunctive techniques were essential to treatment of 80% of aneurysms with dome-to-neck ratios <1.2 (P = .02) and 89% of aneurysms with aspect ratios <1.2 (P < .0001). Multivariate logistic regression analysis demonstrated that aspect ratio was the best predictor of the need for an adjunctive device (P = .0004).
CONCLUSIONS: Aneurysms with aspect and dome-to-neck ratios >1.6 usually did not require adjunctive techniques. Aneurysms with aspect and dome-to-neck ratios <1.2 almost always required adjunctive techniques. In this single-center series, aspect ratio was the independent predictor of the need for adjunctive techniques in the endovascular management of intracranial aneurysms.
Since the early era of detachable coil therapy, assessments of aneurysm geometry and its effect on treatment decisions and treatment outcomes have been in use.1–6 The most common and well-studied geometric determinants of treatment decision and outcome have been dome-to-neck ratio or the maximum aneurysm dome width-to-neck diameter, and neck width. Zubillaga et al7 originally defined a “wide neck” as an absolute neck diameter of 4.0 mm. Debrun et al1,2 defined “wide-neck” aneurysms as those with dome-to-neck ratios of <2.0. These early definitions were created on the basis of success with endovascular coil therapy when the technique was in its infancy. Cloft et al8 later noted that the technical advance of complex coil shapes allowed successful endovascular therapy of aneurysms with a dome-to-neck ratio of >1.5.
These definitions predate widespread use of major technical advances that allow successful coil therapy of wide-neck aneurysms, such as balloon remodeling and stent assistance.9,10 A more practical modern approach to the definition of “wide-neck” or “difficult” aneurysm would be a definition that predicts the need to use adjunctive measures, such as balloons or stents, to treat the aneurysm safely. Furthermore, in addition to dome-to-neck ratio and neck width, other geometric factors may play a role in treatment decisions and outcomes. Although not explored as extensively as dome-to-neck ratio and neck width, aspect ratio, defined as aneurysm height-to-neck width, may play a role as a predictor of treatment outcomes and decisions.
In the current report, we correlate dome-to-neck ratio, aspect ratio, and aneurysm neck diameter with the need for adjunctive measures to propose practical thresholds for the definition of difficult aneurysms. We also ascertain which of these 3 geometric parameters is the best determinant of the need for adjunctive measures in the coiling of intracranial aneurysms.
Materials and Methods
Patients
Following institutional review board approval, a retrospective analysis of 175 consecutive adult patients who were selected for attempted coil embolization of 185 intracranial aneurysms between January 2005 and November 2007 at our institution was conducted. The aneurysms included in this study were included in a previous study examining differences in dome-to-neck ratio in 2D digital subtraction angiography (DSA) and 3D rotational angiography images.11
Angiographic Technique
Typically, 5F or 6F catheters were placed into the internal carotid arteries or vertebral arteries. All of the DSA examinations were performed by using a biplane digital angiography suite (Integris; Philips Medical Systems, Best, the Netherlands). A volume of 16 mL of nonionic contrast medium was injected through a 5- to 6-F catheter by use of an injector with a velocity of 4 mL/s. Biplane DSA images of the entire circulation were usually obtained, followed by working projection DSA. “Working projection” images were those images that offered ideal separation between the aneurysm neck and parent artery.
Coiling Technique
Patients typically were treated under general anesthesia. Guiding catheters or guiding sheaths were placed in the target vessel. A coaxial technique was used for microcatheter, balloon, and stent catheter access. In general, balloons were placed if there was even a moderate suspicion that balloon assist would be needed. Even in cases in which balloons had been placed, at least 1 attempt at coil placement was made before balloon inflation. Balloon inflation was typically performed only if the initial or subsequent coils were not retained in the aneurysm cavity without balloon inflation. Stents were typically used in cases of failed balloon-assist coiling. Four operators were involved in the coiling of these aneurysms.
Analysis of Images
Aneurysm location, maximum dimension, and aneurysm shape were recorded. Aneurysm dome-to-neck ratio, neck width, and aspect ratio in 2D DSA were measured. Aneurysms were classified as those with simple-versus-complex shapes as previously described.4
Measurement of dome-to-neck and aspect ratios was performed on PACS.12 A single reader selected an early- or midarterial phase from the 2D DSA for measurement. The reader used clinical images in an attempt to simulate the clinical environment. An electronic caliper was used to measure the dome diameter, aneurysm height, and neck width. Measurements of the aneurysms were performed on 2 separate occasions. The reader was blinded to the first measurement when performing the second measurement. There was excellent agreement (κ = 0.99) between the 2 sets of measurements, and averages of the 2 measurements were used for analysis. The reader was also blinded as to whether an adjunctive device was used.
Outcomes and Complications
There were 4 outcomes for endovascular coiling: 1) complete occlusion, 2) near-complete occlusion, 3) incomplete occlusion, and 4) failure of occlusion. Successful treatment was defined as those aneurysms that had complete or near-complete occlusion on postoperative angiograms. The outcome of each procedure was determined by the neuroradiologist who analyzed the postoperative 2D DSA images of the treated aneurysm. Immediate postoperative outcomes are presented in this study. Immediate complications resulting from each procedure were also recorded. Complications were stratified into 4 groups; 1) thromboembolic complications, 2) parent artery occlusion, 3) local thrombus formation, and 4) aneurysm perforation. Complications were determined by the neuroradiologist who performed the endovascular coiling. When obtaining information on thromboembolic complications, we examined patient files for clinical evidence of thromboembolism originating at the site of the coiling.
Statistical Analysis
For categoric variables, a χ2 test was used to determine statistical significance. For determining the thresholds of dome-to-neck ratio, aspect ratio, and neck size that were most predictive of the need or lack of need for adjunctive techniques, χ2 testing was used. For determination of the significance of continuous variables, a Student t test was performed. For determining which geometric features of aneurysms were most predictive of treatment decisions, a multivariate logistic regression analysis was performed, and a log-likelihood test was performed to determine the goodness of fit of the logistic model.
Results
Demographic and Presentation Data
The patient population consisted of 44 men and 131 women. The average age was 59 ± 13 years. Of the 185 aneurysms, 138 were found in the anterior circulation (internal carotid, anterior cerebral, anterior communicating, ophthalmic, anterior choroidal, and posterior communicating arteries) and 47 were in the posterior circulation (posterior cerebral, superior cerebellar, basilar, vertebral, and posterior inferior cerebellar arteries). Of the 185 aneurysms, 54 (29%) presented as ruptured.
Characteristics of Aneurysms Treated with and without Adjunctive Techniques
In total, 115 aneurysms (62%) were treated without adjunctive techniques, and 70 aneurysms (38%) were treated with adjunctive techniques. Overall, the average dome-to-neck ratio for the aneurysms in this study was 1.82 ± 0.56, the average neck size was 3.4 ± 1.8 mm, and the average aspect ratio was 1.85 ± 0.71.
Aneurysms treated without adjunctive techniques had an average dome-to-neck ratio of 1.97 ± 0.59, an average aspect ratio of 2.09 ± 0.68, and an average neck size of 3.0 ± 1.5 mm. Aneurysms treated with adjunctive techniques had an average dome-to-neck ratio of 1.59 ± 0.42, an average aspect ratio of 1.48 ± 0.59, and an average neck size of 4.0 ± 2.0 mm. Thus, on average, aneurysms treated without adjunctive techniques had a larger dome-to-neck ratio (P < .0001), a larger aspect ratio (P < .0001), and smaller neck sizes (P = .0004). There was no difference in the shape (complex versus simple) (P = .74) between those aneurysms treated with and without adjunctive techniques or in the presentation (ruptured versus nonruptured) (P = .25). These data are summarized in Table 1.
Characteristics of aneurysms treated with and without adjunctive techniques
Influence of Dome-to-Neck Ratio on Treatment Decisions
When examining the effect of dome-to-neck ratio on treatment decisions, we determined that coiling without adjunctive techniques was favored over coiling with adjunctive techniques for aneurysms with a dome-to-neck ratio ≥1.6 in 78 of 104 (75%) cases (P < .0001). For aneurysms with a dome-to-neck ratio <1.2, coiling with adjunctive techniques was favored over coiling without adjunctive techniques in 12 of 15 (80%) cases (P = .02). For aneurysms with dome-to-neck ratios between 1.2 and 1.6, the frequency of use of adjunctive techniques (32 cases) was similar to the frequency of use of no adjunctive techniques (34 cases) (P = .81). Figure 1 shows the percentage of cases needing adjunctive devices at given intervals of dome-to-neck ratios.

Effect of dome-to-neck ratio on the need for adjunctive devices in endovascular management. This graph demonstrates the influence of dome-to-neck ratio on treatment decisions. For cases with dome-to-neck ratios <1.6, adjunctive techniques were used in most of them, whereas for cases with dome-to-neck ratios >1.6, aneurysms were treated without adjunctive techniques in most of them.
Influence of Neck Size on Treatment Decisions
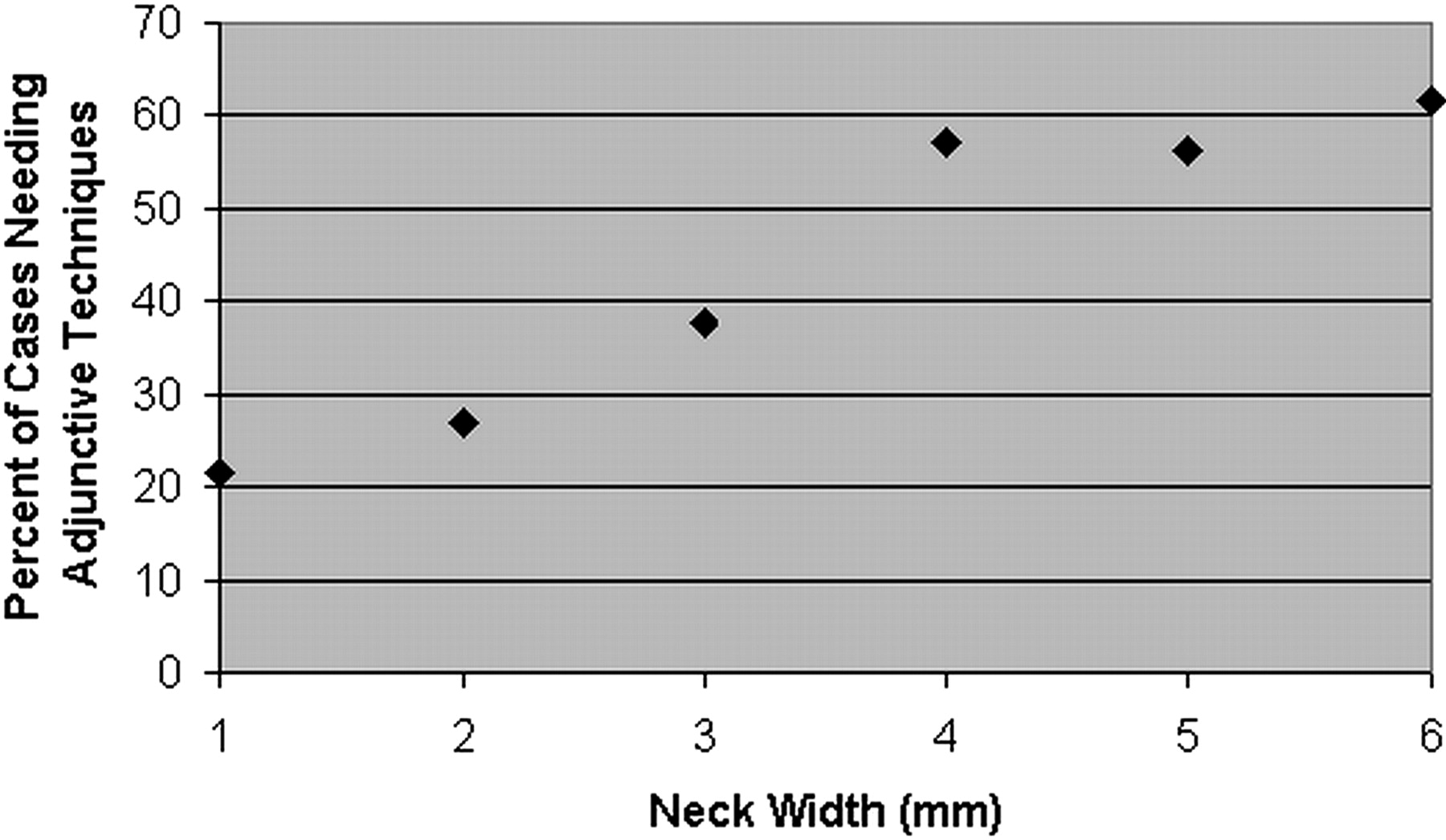
When examining the effect of neck size on treatment decisions, we determined that coiling without adjunctive techniques was favored over coiling with adjunctive techniques in 94/134 (70%) cases of aneurysms with a neck size <4.0 mm (P < .0001). However, there was no neck size in which coiling with adjunctive techniques was significantly favored over coiling without adjunctive techniques because 30/51 (59%) aneurysms with a neck size >4.0 mm were treated with adjunctive techniques (P = .21). Figure 2 shows a comparison of the percentage of cases needing adjunctive devices at given intervals of neck widths.

Effect of neck size on the need for adjunctive devices in endovascular management. This graph demonstrates the influence of neck size on treatment decisions. For a neck size <4.0 mm, coiling without adjunctive techniques was favored over coiling with adjunctive techniques. At a neck size >4.0 mm, this was no longer true.
Influence of Aspect Ratio on Treatment Decision
When examining the effect of aspect ratio on treatment decisions, we found that coiling with adjunctive techniques was favored over coiling without adjunctive techniques at an aspect ratio <1.2 in 24 of 27 (89%) cases (P < .0001). For cases with an aspect ratio >1.6, coiling without adjunctive techniques was favored over coiling with adjunctive techniques in 87 of 110 (79%) cases (P < .0001). Figure 3 shows a comparison of the percentage of cases needing adjunctive devices at given aspect ratios.

Effect of aspect ratio on the need for adjunctive devices in endovascular management. This graph demonstrates the influence of aspect ratio on the need for adjunctive techniques. Most cases with aspect ratios <1.4 necessitated adjunctive techniques in their management; however, statistical significance was attained at an aspect ratio >1.6.
Multivariate Analysis
After performing a multivariate logistic regression analysis comparing the effects of dome-to-neck ratio, aspect ratio, and aneurysm neck size on treatment decisions, we found aspect ratio to be the strongest and only statistically significant independent predictor (P = .0004) of the need for an adjunctive technique. Larger aspect ratios were associated with a lower need for adjunctive techniques, and smaller aspect ratios were associated with a higher need for adjunctive techniques. Neck size and dome-to-neck ratio were not found to be independent predictors of the need for an adjunctive technique. The goodness of fit of this multivariate logistic regression analysis was P < .0001.
We also compared the combined effect of aspect ratio and dome-to-neck ratio on treatment decisions (Table 2). For aneurysms with a dome-to-neck ratio >1.6 (ie, “favorable” geometry based on dome-to-neck), aneurysms with aspect ratios <1.6 (ie, “unfavorable” geometry based on aspect ratio) were treated with adjunctive techniques in 10/24 (42%) cases. When the aspect ratio was increased above 1.6, 16/80 (20%) cases were treated with adjunctive techniques. The effect of this increase in aspect ratio on the ability to treat aneurysms without adjunctive techniques was statistically significant (P = .03). Conversely, for aneurysms with an aspect ratio >1.6 (ie, “favorable” geometry based on aspect ratio), aneurysms with dome-to-neck ratios <1.6 (ie, “unfavorable” geometry based on dome-to-neck) were treated with adjunctive techniques in only 7/31 cases (23%). When the dome-to-neck ratio was increased above 1.6, 16/80 (20%) cases were treated without adjunctive techniques. Thus, for aneurysms with an aspect ratio >1.6, changes in dome-to-neck ratio from <1.6 to >1.6 had no effect on the ability to treat aneurysms without adjunctive techniques (P = .76). An example of an aneurysm with a low dome-to-neck ratio and a high aspect ratio that was successfully treated without adjunctive techniques can be seen in Fig 4.
Percentage of cases needing adjunctive techniques at given dome-to-neck and aspect ratios

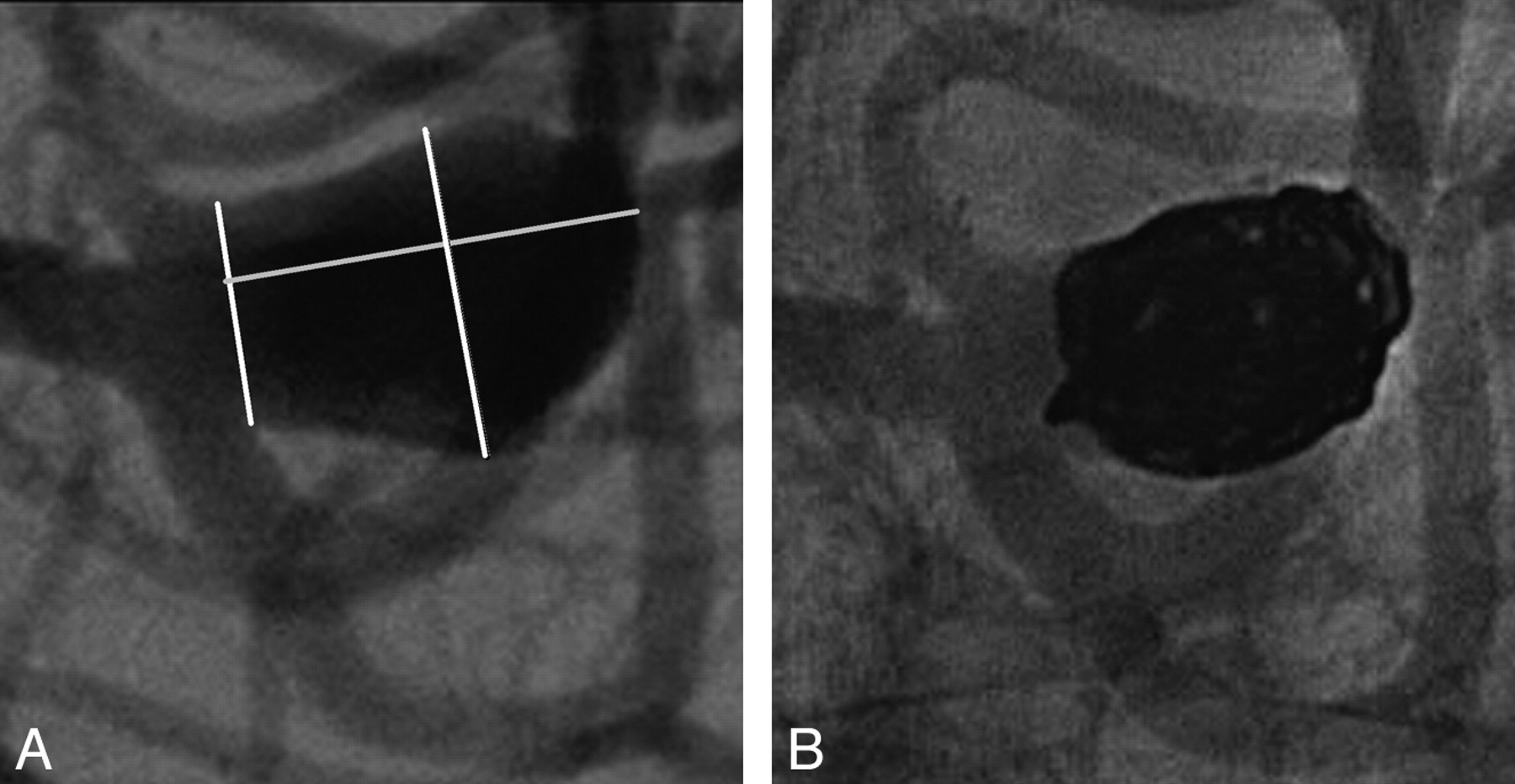
Coiling of middle cerebral artery aneurysm. Images show the successful coiling of a middle cerebral artery bifurcation aneurysm without adjunctive techniques in a 50-year-old man. A, This aneurysm has an unfavorable dome-to-neck ratio (1.3), an unfavorable neck width (5.0 mm), and a favorable aspect ratio (1.8). Given the low dome-to-neck ratio and large neck width, this aneurysm would have been considered not amenable to coiling without adjunctive techniques. B, Immediate postoperative image of the aneurysm shows near-complete coiling with a small neck remnant.
Treatment Outcomes
Overall, 111 of the 115 (96.5%) aneurysms treated without adjunctive techniques were successfully treated with complete (50 cases) or near-complete (61 cases) occlusion of the aneurysm. The 4 cases that were not successfully treated had an average aspect ratio of 1.74 ± 0.66, an average dome-to-neck ratio of 2.16 ± 0.58, and an average neck width of 3.31 ± 2.32. Sixty-five of the 70 aneurysms (92.9%) treated with adjunctive techniques were successfully treated with complete (20 cases) or near-complete (45 cases) occlusion of the aneurysm. The 5 unsuccessfully treated cases had an average aspect ratio of 1.32 ± 0.49, an average dome-to-neck ratio of 1.39 ± 0.34, and an average neck width of 3.02 ± 1.16.
When comparing the dome-to-neck ratio, aspect ratio, and neck size of completely occluded aneurysms versus incompletely (ie, near-complete and unsuccessfully treated combined) occluded aneurysms, we found that the completely occluded aneurysms had larger dome-to-neck ratios (1.91 ± 0.59 versus 1.76 ± 0.54, P = .08), larger aspect ratios (1.92 ± 0.71 versus 1.81 ± 0.70, P = .30), and smaller neck sizes (3.2 ± 1.4 mm versus 3.6 ± 2.0 mm, P = .14); however, none of these values were statistically significant. Multivariate analysis demonstrated that dome-to-neck ratio was the best independent predictor of complete occlusion; however, this was not statistically significant (P = .19)
Complications
Overall 16 of the 115 (13.9%) aneurysms treated without adjunctive techniques had a complication associated with the procedure, including 1 case of thromboembolic complication, 10 cases of local thrombus formation, and 5 cases of intraprocedural aneurysm perforation. Eleven of the 70 (15.7%) aneurysms treated with adjunctive techniques had complications associated with the procedure, including 1 case of thromboembolic complication, 8 cases of local thrombus formation, and 2 cases of intraprocedural aneurysm perforation. Overall, there were no cases of parent artery occlusion. In all cases of local thrombus formation, the thrombus was promptly dissolved by using anticoagulation. In cases of aneurysm perforation, there were no sequelae because all these aneurysms were successfully treated. In the 2 cases of thromboembolic complications, the effects were transient and resulted in no permanent dysfunction.
Discussion
In this study, we demonstrated that a low aspect ratio plays a more dominant role than either dome-to-neck ratio or neck diameter in predicting the need for adjunctive techniques in the coiling of intracranial aneurysms. Furthermore, aspect ratio is a significant independent predictor of the need for these adjunctive techniques. We also demonstrated that the coiling of intracranial aneurysms without adjunctive techniques such as stent placement and balloon remodeling is clinically favored for aneurysms with an aspect ratio ≥1.6, a dome-to-neck ratio ≥1.6, and a neck size of <4 mm. Coiling with adjunctive techniques is favored for aneurysms with dome-to-neck ratios <1.2 as well as aspect ratios <1.2. For aneurysms with dome-to-neck ratios between 1.2 and 1.6, coiling with and without adjunctive techniques was performed equally. The same was true for aneurysms with aspect ratios between 1.2 and 1.6.
Previous studies discussing wide-neck morphologies have used relatively outdated thresholds. The first studies to determine the impact of dome-to-neck ratio on treatment decisions and outcomes were performed by Debrun et al,1,2 when endovascular coiling of intracranial aneurysms was in its infancy. They demonstrated that in a 25-case series, inferior outcomes in endovascular coiling were associated with aneurysms with dome-to-neck ratios <2.0. Since the time of publication of these studies, aneurysms with dome-to-neck ratios <2.0 have been classified as wide neck. In our study population, by using the threshold of 2.0, 70% (130/185) of aneurysms would have been considered wide neck. Additionally, with a mean dome-to-neck ratio of 1.82 in our population, even an average aneurysm would be defined as having a wide neck if we used a dome-to-neck ratio of 2.0 in our definition.
Because we believe that the definition for wide-neck aneurysm should relate to exceptional aneurysms rather than typical aneurysms, our study instead focused on the practical ramifications of wide-neck morphologies—that is, whether an aneurysm is likely to require adjunctive techniques for treatment. We were able to make this assessment because our standard practice is to attempt to coil essentially every aneurysm without adjunct and to inflate a balloon only if primary coiling fails. For cases with dome-to-neck ratios <1.2, we found that coiling with adjunctive techniques was significantly favored over coiling without adjunctive techniques. Thus, we propose that the term “wide-neck” be used for aneurysms with dome-to-neck ratios <1.6 and “very wide-neck” be used for aneurysms with dome-to-neck ratios <1.2. Thresholds for wide- neck and very wide-neck regarding aspect ratio would be 1.6 and 1.2, respectively. These thresholds may allow improved communication and standardization for such terminology in the interventional community.
The current study is the first to show that aspect ratio is a significant independent determinant of the need for an adjunctive technique. Notably, the impact of aspect ratio dominates that of dome-to-neck ratio for predicting the need for adjunctive techniques. Specifically, we have shown that even in cases in which the dome-to-neck ratio is unfavorable, aneurysms with favorable aspect ratios frequently can be treated without adjunctive techniques with success equal to those treated with adjunctive techniques. Conversely, even in cases in which the dome-to-neck ratio is favorable, aneurysms with unfavorable aspect ratios usually require adjunctive measures. Notably, for cases with more extreme aspect ratios (aspect ratio <1.2, aspect ratio >2.0), aspect ratio alone determines the need for adjunctive techniques in nearly 90% of cases, irrespective of dome-to-neck ratio.
Our study has a number of limitations. First, it is limited by the inherent subjective nature of when to use an adjunctive measure. In our practice, as noted in the “Materials and Methods” section, we typically will at least try 1 type of coil before inflating a balloon. We acknowledge that other operators may try either multiple attempts with 1 coil or multiple different types of coils with various shapes or diameters before inflating a balloon. In addition, there is almost certain interobserver bias, even within our own practice, regarding the need for adjunctive measures. As such, our standard of reference for the use of adjunctive measures, that of “needing” balloon inflation in our practice, is imperfect. Second, the authors recognize that there exist other anatomic parameters that are important in determining the need for an adjunctive device that were not taken into consideration in this study, such as the relationship of the aneurysm to the parent artery and the location of an aneurysm at a bifurcation of an artery.4
Third, it might be argued that this study is from a single center and may not reflect widespread practice. Given the definition that we propose of a dome-to-neck ratio <1.6 as being wide neck, 81 of the 185 (43.7%) aneurysms in this study would be considered wide-neck and likely not amenable to coiling without adjunctive techniques. Given the alternative definition of an aspect ratio of <1.6 being wide-neck, 74 of the 185 (40%) aneurysms studied would be considered wide-neck and likely not amenable to coiling without adjunctive techniques. In actual practice, we used adjunctive techniques in 38% of the cases. Two recent multicenter studies have demonstrated that adjunctive techniques were necessary in approximately 45% of cases.13,14 Thus, our practice with adjunctive techniques does not seem to be unusual.
Ultimately, given the retrospective nature of our study and the subjectivity of a need to use adjunctive devices, our observations cannot be applied to the treatment of aneurysms in general. Thus, this study hopes to function as a potential baseline for future research of adjunctive techniques such as balloons and stents. Determining the exact anatomic and clinical parameters that make adjunctive techniques necessary in the endovascular treatment of aneurysms is critical so as to not subject patients to the unnecessary complications of these techniques. In addition, proving the utility of newer adjunctive devices will be much easier if they are applied in studies focused on aneurysms that are likely to require adjunctive techniques for successful endovascular therapy. As mentioned earlier, studies often cite the wide-neck criteria of dome-to-neck ratio <2.0 and a neck size >4.0 as signifying a need for an adjunctive device and have not investigated the role of aspect ratio. However, our study suggests that these criteria are not necessarily ideal because our criteria for defining an aneurysm as “wide-neck” is a dome-to-neck ratio <1.6 rather than 2.0, a neck width >4.0, and an aspect ratio <1.6.
Conclusions
In this retrospective study, we methodically determined criteria to define a difficult aneurysm likely to require adjunctive measures for treatment. We have demonstrated that a practical approach to defining wide-neck geometric criteria includes an aspect ratio <1.6, a dome-to-neck ratio <1.6, and a neck width >4.0 mm. In this single-center series, aspect ratio was the independent predictor of the need for adjunctive techniques in the endovascular management of intracranial aneurysms.
References
- Received January 14, 2009.
- Accepted after revision March 7, 2009.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Lateral Compression Manipulation: A Simple Approach for Sizing Taller-Than-Wide Intracranial Aneurysms with the Woven EndoBridge Device
- Deep learning-based cerebral aneurysm segmentation and morphological analysis with three-dimensional rotational angiography
- Deep learning-based cerebral aneurysm segmentation and morphological analysis with three-dimensional rotational angiography
- Development of the SAFETEA Scores for Predicting Risks of Complications of Preventive Endovascular or Microneurosurgical Intracranial Aneurysm Occlusion
- Endovascular Treatment of Small and Very Small Intracranial Aneurysms with the Woven EndoBridge Device
- Flow-Diversion Treatment for Unruptured ICA Bifurcation Aneurysms with Unfavorable Morphology for Coiling
- eCLIPs bifurcation remodeling system for treatment of wide neck bifurcation aneurysms with extremely low dome-to-neck and aspect ratios: a multicenter experience
- Early clinical experience with Cascade: a novel temporary neck bridging device for embolization of intracranial aneurysms
- Critical role of angiographic acquisition modality and reconstruction on morphometric and haemodynamic analysis of intracranial aneurysms
- Safety and effectiveness of the Low Profile Visualized Intraluminal Support (LVIS and LVIS Jr) devices in the endovascular treatment of intracranial aneurysms: results of the TRAIL multicenter observational study
- European Multicenter Study for the Evaluation of a Dual-Layer Flow-Diverting Stent for Treatment of Wide-Neck Intracranial Aneurysms: The European Flow-Redirection Intraluminal Device Study
- WEB Treatment of Ruptured Intracranial Aneurysms: A Single-Center Cohort of 100 Patients
- Coiling of wide-necked carotid artery aneurysms assisted by a temporary bridging device (Comaneci): preliminary experience
- Single-center experience in the endovascular treatment of wide-necked intracranial aneurysms with a bridging intra-/extra-aneurysm implant (pCONus)
- Diagnostic Impact of Bone-Subtraction CT Angiography for Patients with Acute Subarachnoid Hemorrhage
- Single-Layer WEBs: Intrasaccular Flow Disrupters for Aneurysm Treatment--Feasibility Results from a European Study
- HydroCoils Are Associated with Lower Angiographic Recurrence Rates Than Are Bare Platinum Coils in Treatment of "Difficult-to-Treat" Aneurysms: A Post Hoc Subgroup Analysis of the HELPS Trial
- Coil Occlusion of Wide-Neck Bifurcation Aneurysms Assisted by a Novel Intra- to Extra-Aneurysmatic Neck-Bridging Device (pCONus): Initial Experience
- Standard of practice: embolization of ruptured and unruptured intracranial aneurysms
- Intrasaccular Flow-Disruption Treatment of Intracranial Aneurysms: Preliminary Results of a Multicenter Clinical Study
- Aneurysm Ostium Angle: A Predictor of the Need for Stent as Assistance for Endovascular Aneurysm Coiling in Internal Carotid Artery Sidewall Aneurysms
- Stent-Assisted Coiling of Complex Middle Cerebral Artery Aneurysms: Initial and Midterm Results