
Abstract
BACKGROUND AND PURPOSE: Prenatal imaging data of the normal pituitary gland and in vivo information on the development of the pituitary region are lacking; however, we noticed that the pituitary stalk (PS) is visible occasionally in utero on MR images. Our main purpose was to establish the detection rate of the PS in healthy fetuses at various gestational ages (GAs) by using single-shot fast spin-echo T2-weighted images.
MATERIALS AND METHODS: We selected 73 fetal cases with normal findings on prenatal MR imaging and clinical postnatal follow-up. The GA ranged between 19 and 37 weeks. The 3 planes of MR imaging sections were 4 mm thick with 1.25 × 1.25 mm in-plane resolution. Two pediatric neuroradiologists evaluated in consensus whether the PS was present as a linear isointense structure connecting the hypothalamic region with the floor of sella turcica. In those cases in which the PS was visible on the sagittal section, the angle formed by the intersection of the PS and the sellar plane (SP) was measured (PS-SP angle).
RESULTS: The PS was detectable on at least 1 coronal or sagittal section from 19 to 25 weeks’ GA in 30/42 fetuses (71.4% sensitivity); from 26 to 37 weeks’ GA, the PS was detected in all 31 fetuses (100% sensitivity). The PS-SP angle decreased significantly with GA, being <90° in all fetuses after gestational week 25.
CONCLUSIONS: At the current spatial resolution of clinical prenatal MR imaging, PS can be reliably detected after 25 weeks’ GA, so in case of a missing visualization, a strong suspicion of pituitary region anomaly could be raised.
Prenatal imaging data about the normal pituitary gland and direct in vivo information on the development of the pituitary region are, to our knowledge, substantially lacking. During postnatal life, even starting from the neonatal age, MR imaging, by using sagittal high-spatial-resolution T1-weighted sections, can depict the anterior pituitary gland, the posterior pituitary gland, and the pituitary stalk (PS) with exquisite detail.1 On the other hand, in our experience, the direct depiction of the pituitary gland itself by means of sagittal T1-weighted images is only occasionally feasible in prenatal MR imaging, especially at earlier gestational ages (GAs); moreover, only a few examples of advanced GA fetuses displaying the pituitary gland on sagittal T1-weighted images have been reported.2 However, we noticed that other pituitary region structures, such as the PS, could be depicted in utero by using single-shot fast spin-echo (SS-FSE) T2-weighted images, which are the mainstay tool of current clinical fetal MR imaging.
Congenital hypopituitarism (CH) can be associated with some pituitary region anomalies,1,3,4 such as PS interruption or absence (frequently with ectopic neurohypophysis). CH is rare; its prevalence is estimated to be approximately between 1/5000 and 1/30,000 children, according to different studies.5,6 However, CH may result in severe and unpredictable neonatal hypoglycemic encephalopathy.7,8 The early detection of pituitary gland dysfunction (in particular of growth hormone deficiency) might help in planning for advance hormone replacement therapy.9 For these reasons, the knowledge of normative data on the fetal pituitary region could be valuable in detecting possible pituitary anomalies in fetuses undergoing MR imaging. Our main purpose was to establish the detection rate of the PS in healthy fetuses at various GAs, by using SS-FSE T2-weighted images.
Materials and Methods
From approximately 800 fetal MR imaging studies performed at our institution between 2000 and 2006, we retrospectively selected 73 fetal cases with the following characteristics: studies performed for suspected body lesions or because brain malformations had been detected in previous pregnancies, and normal brain on prenatal MR imaging. In all cases, a normal neurodevelopmental evaluation at postnatal age ranging from a minimum of 3 months to a maximum of 42 months could be gathered from different sources: clinical records from child neurologists of our or other institutions and written or oral reports from family pediatricians.
The GA ranged between 19 and 37 weeks. MR imaging studies were preformed at 1.5T, by using surface abdominal coils. No fetal or maternal sedatives were administered. The scanning technique was based on multiplanar SS-FSE T2-weighted 4-mm-thick contiguous sections (TR/TE, 3000/180 ms; FOV, 320 mm; matrix, 256 × 256; 1.25 × 1.25 mm in-plane resolution). Coronal sections were positioned orthogonal to axial ones, which had been acquired parallel to the subcallosal plane. We prescribed sagittal sections by using coronal ones as a guide, taking care to use a slab with an odd number of sections, in order to have one of the sections encompassing the midsagittal plane.
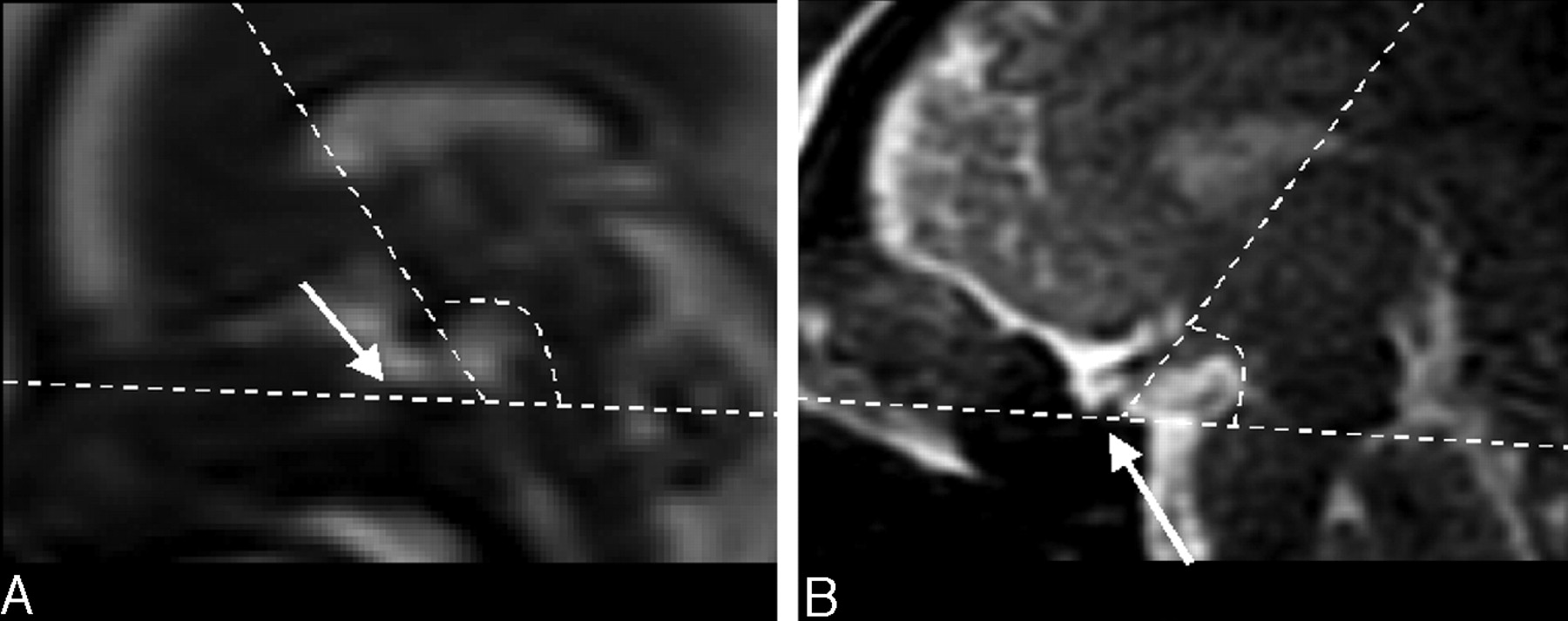
Two senior pediatric neuroradiologists (A.R., C.P.) evaluated in consensus all selected cases. The PS was considered to be present when a linear isointense structure connecting the hypothalamic region with the floor of sella turcica was visible on at least 1 coronal or sagittal section (Fig 1). In some cases, a round, ovoid, or irregular triangular hypointense structure was visible on the sellar floor; this structure, very likely representing the whole pituitary gland (anterior and posterior part), was, however, so variable in appearance in volume and shape that we decided not to consider it as sign of integrity of the anatomic region. In addition, the latter decision was also made because the anterior and posterior hypophysis had similar signal intensities, and they were not distinguishable from each other on SS-FSE T2-weighted images. In those cases in which the PS was visible on the sagittal section, the angle determined by the intersection of the PS and the sellar plane (SP) was measured (PS-SP angle) (Fig 2). This angle was taken into account because its possible variation with GA could represent an easy-to-obtain objective parameter for monitoring the normal development of the hypothalamic-pituitary region (ie, the relationship between the hypothalamus position and the sella turcica as indicated by PS-SP angle). This measurement was possible because the sellar floor was substantially flat on sagittal images, so a plane lying on it could be identified (SP). In fewer more advanced GA fetuses, in which the sellar floor already had some concave aspect, the so-called “SP” line was traced encompassing the anterior and posterior margin of the sella turcica. Finally, possible significant correlation of the variation of PS-SP angle with GA was established by simple linear regression analysis.

Sample cases of coronal and sagittal SS-FSE T2-weighted sections from 21 weeks’ GA (A and C) and 27 weeks’ GA (B and D) show the PS (arrows); curved arrows indicate the optic chiasm and optic nerve, which are more horizontally oriented than the PS.

Sagittal SS-FSE T2-weighted sections from 22 (A) and 37 (B) weeks’ GA fetuses show the PS-SP angle measurement method. Note the flat appearance of the sellar floor (arrows).
Results
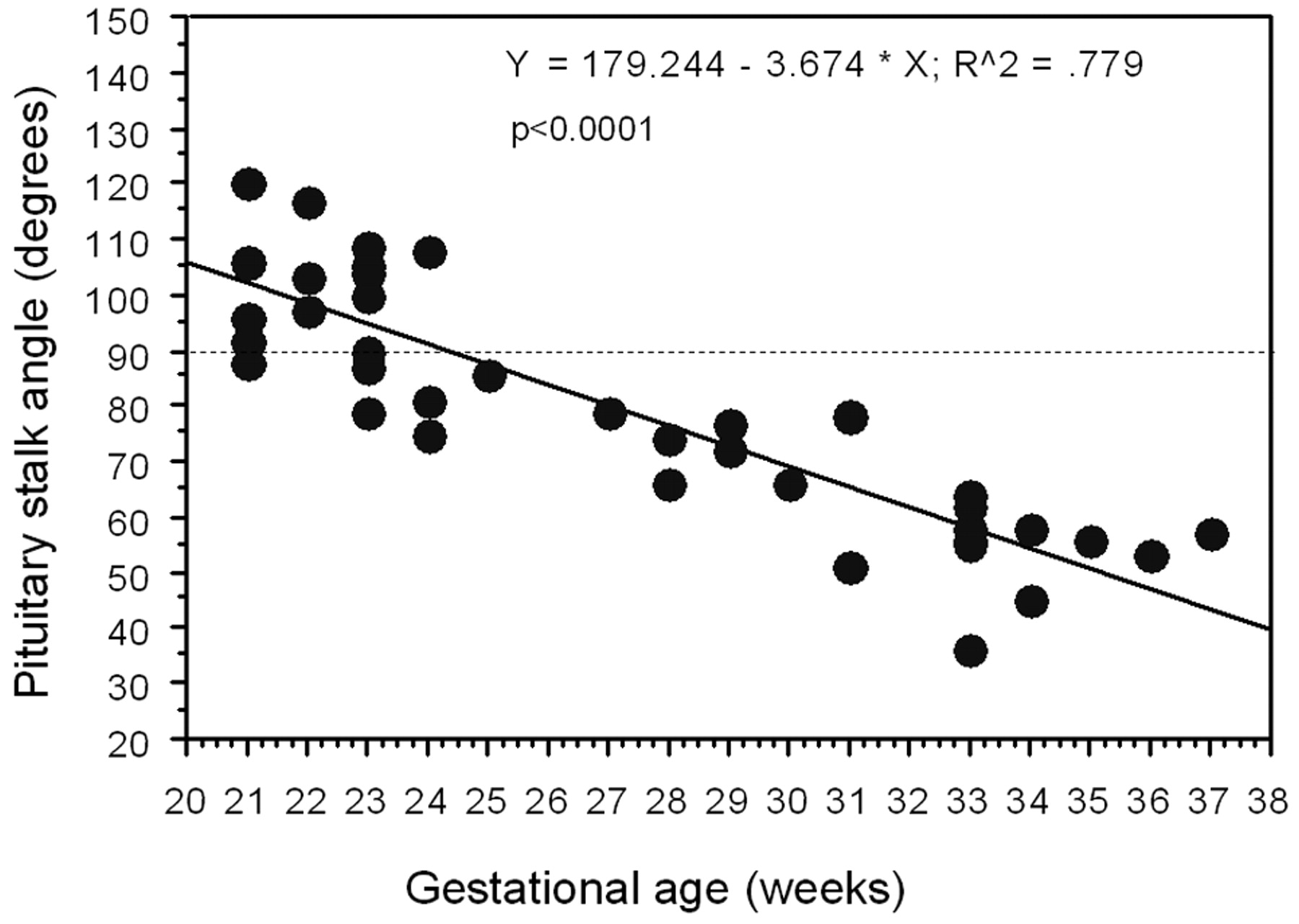
From 19 to 25 weeks’ GA, the PS was detectable in 30/42 fetuses (71.4% sensitivity); the PS was detected in all 31 fetuses from 26 to 37 weeks’ GA (100% sensitivity). In 39 fetuses (ranging from 21 to 37 weeks’ GA), the PS-SP angle could be measured; it decreased significantly with GA, being <90° in all fetuses after 25 weeks of gestation (Fig 3).

Graph showing the PS-SP angle changes with GA in those 39 fetuses (range, 21–37 weeks’ GA) where the PS was visible on the sagittal section.
Discussion
This article reports the feasibility of assessment of the PS integrity during the fetal life; it also shows that easy-to-depict features, such as the PS-SP angle, may represent a parameter that could help to assess the normal development of the pituitary region. On a single-case basis, the integrity of the PS and the normal PS-SP angle might not totally rule out some hypothalamic-hypophyseal-axis functional anomalies,10 because normal PS and gene mutation-deletion (ie, the PROP1 gene) have been considered as one of the most common causes of congenital hypopituitarism in the fetus. Conversely, the absence or interruption of the PS is very often associated with posterior pituitary gland anomalies and hormonal dysfunction.11
The clinical impact of the prenatal MR imaging capability of depicting pituitary region structures (in particular the PS) still remains to be explored because the small prevalence of CH makes the predictive value of the imaging test (missing PS visualization) low. The number of prenatal MR imaging examinations is increasing steadily in many countries, so the possibility of encountering even rarer anomalies will increase in everyday practice. As mentioned before, the prediction of the risk of neonatal hypoglycemic encephalopathy or the early detection of possible growth hormone deficit is potentially of clinical relevance. Moreover, the depiction of pituitary region anomalies (ie, the absence of the PS but also PS-SP angle aberrant values) might help in better characterizing possibly associated more complex central nervous system malformations detected in utero, such as fetuses with septum pellucidum region or forebrain abnormalities.
Prenatal MR imaging allows exploring areas of the fetal central nervous system, which have been so far substantially neglected in prenatal imaging. However, perhaps, in the near future, additional improvements in sonographic technology would allow the accurate investigation of this region to be performed by this technique too.
The PS-SP angle turned out to be an easy and practical measurement, which could be carried out in clinical practice on a single-case basis. The decrease of the PS-SP angle with GA seems to match reliably the brain and cranial maturation. We cannot provide a definite explanation for this angle value variation with cerebral maturation; however, a possible difference in the growth rates between brain hemispheres and the skull (in particular the skull base) might play a pivotal role in this process.
We cannot provide a definite explanation for why the PS was not identifiable in 100% of cases before 26 weeks’ GA. Probably the limited spatial resolution of our images did not allow a constant visualization. We did not perform a postnatal MR imaging control or postnatal endocrine tests in all those 12 fetal cases in which the PS was not detected before 26 weeks’ GA. For this reason, we cannot totally rule out the remote possibility that 1 of these fetuses might have carried a pituitary region anomaly. However, the clinical and sonographic follow-up results were normal, reducing the probability of some inclusion criteria error.
We could not perform quantitative evaluations such as the measurement of PS thickness and checking for its possible variation with GA because the spatial resolution of our scanning technique was not sufficient for this purpose.
In our series, the presence or absence of the pituitary gland itself was not taken into account. That was mainly for 2 reasons: 1) Strong limitation in the visualization of the gland was seen on both T2- and, more important, T1-weighted images, as mentioned earlier; 2) pituitary gland aplasia itself is an exceptional event,12 which is much rarer than the PS absence or interruption associated with an otherwise regular pituitary gland. Moreover, pituitary dysfunction can arise even in the presence of a well-recognizable pituitary gland, whereas the pituitary deficit is more commonly associated with PS structural anomalies. For these reasons, prenatal imaging diagnostic criteria based on the presence or absence of the pituitary gland may have less clinical impact than those based on PS integrity.
Conclusions
At the current spatial resolution of clinical prenatal MR imaging, the PS can be reliably detected after 25 weeks’ GA, so in case of a missing visualization, a strong suspicion of pituitary region anomaly could be raised. It remains to be evaluated if aberrant PS-SP angle values may help in identifying and better characterizing more general congenital brain anomalies in utero.
References
- Received October 16, 2008.
- Accepted after revision December 2, 2008.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}