
Abstract
BACKGROUND AND PURPOSE: Vertebroplasty has been commonly used for the treatment of vertebral compression fractures. Practitioners usually attempt to maximize filling of the vertebral body with polymethylmethacrylate (PMMA), either by using a bipediculate approach with separate infusions in both hemivertebrae or by using a unipediculate approach with central needle placement that allows bilateral hemivertebral filling. This study serves to investigate the clinical efficacy of a unipediculate approach in which the cement injected does not cross the midline, with resultant “hemivertebroplasty.”
MATERIALS AND METHODS: A retrospective review of 917 vertebroplasty procedures was performed. A radiologic review of each vertebroplasty in the data base was performed to extract the vertebroplasties in which there was filling of only 1 side of the hemivertebra, which we term “hemivertebroplasty.” Pre- and postoperative evaluations (1-week to 2-year postprocedure) included a Visual Analog Scale (VAS) for pain, the Roland-Morris Disability Questionnaire (RDQ) scores, and information regarding new fractures and retreatment of augmented fractures.
RESULTS: No significant difference was found between the hemivertebroplasty cases and the bilaterally filled vertebroplasty group in reducing VAS or RDQ scores. Moreover, survival analysis showed no significant difference in the risk of incident fracture between groups (hazard ratio = 0.81; 95% confidence interval, 0.33–2.65).
CONCLUSIONS: On the basis of our results, unilateral “hemivertebroplasty” is as effective in reducing pain with activity and at rest and decreasing the RDQ scores as bilateral vertebral filling. Additionally, vertebrae undergoing unilateral filling were at no greater risk of refracture or fracture of adjacent vertebrae than bilaterally filled vertebrae.
Percutaneous vertebroplasty is a common treatment for painful vertebral compression fractures. Early studies reported the use of a bipediculate approach to fill both hemivertebrae separately.1 Later reports described a unipediculate approach, in which central needle placement was used in an attempt to fill both sides of the vertebral body from a single approach, obviating a second needle placement.2 The unipediculate approach has been shown to be as efficacious as the bipediculate approach.
Unipediculate vertebroplasty is now widely accepted as a standard technique in vertebroplasty. However, in some cases, cement may fail to fill both sides of the hemivertebra from the single needle, prompting some practitioners to place a second needle to fill the unfilled hemivertebra. Prior studies focused on unipediculate vertebroplasty have not specifically addressed outcomes in “hemivertebroplasty,” which we define here as a vertebral body in which only 1 side of the vertebra contains cement.2
A previous cadaveric investigation tested the effect of cement volume and placement on the strength and integrity of fractured vertebrae undergoing vertebroplasty.3 This study found that hemivertebroplasty was just as effective as centrally placed cement in the restoration of strength, stiffness, and height in the fractured vertebrae. Additionally, these authors noted that laterally placed cement does not increase the risk of fracture of the unaugmented side.
In the current study, we report clinical outcomes among a cohort of patients who were treated with hemivertebroplasty and compare these outcomes with a larger cohort of patients who underwent vertebroplasty procedures in which both sides of the hemivertebra were filled with cement.
Materials and Methods
Patient Population
We performed a retrospective review of our data base, which included >900 vertebroplasty procedures performed between February 1999 and June 2008. This same cohort has been analyzed in multiple previous retrospective reviews but has never been analyzed regarding the effect of cement distribution on outcome.4-15 Institutional review board approval was granted for this study, and all patient information was handled according to the Health Insurance Portability and Accountability Act standards.
Procedure Details
Patients with vertebral compression fractures with intractable pain were treated with vertebroplasty when conservative treatments failed. Vertebroplasty was performed with the patient under conscious sedation or general anesthesia and as specified previously.1,6 All vertebroplasties were performed under the guidance of biplane fluoroscopy, and an 11- or 13-gauge needle was used to traverse the pedicle. In general, we used a unipediculate approach, with relatively central needle placement. Polymethylmethacrylate (PMMA), as previously described,1,5 was injected into the vertebral body until the cement reached the posterior one fourth of the vertebral body or if epidural, venous, or transendplate extravasation of cement was observed.4-6 In most cases, if both hemivertebrae were not filled with cement, a second needle was placed to infuse cement into the unfilled hemivertebra. However, at the discretion of the operator, some procedures were terminated even with filling of only 1 hemivertebra. In general, patients were kept supine for 2 hours after the procedure before being discharged.
Definition of Hemivertebroplasty
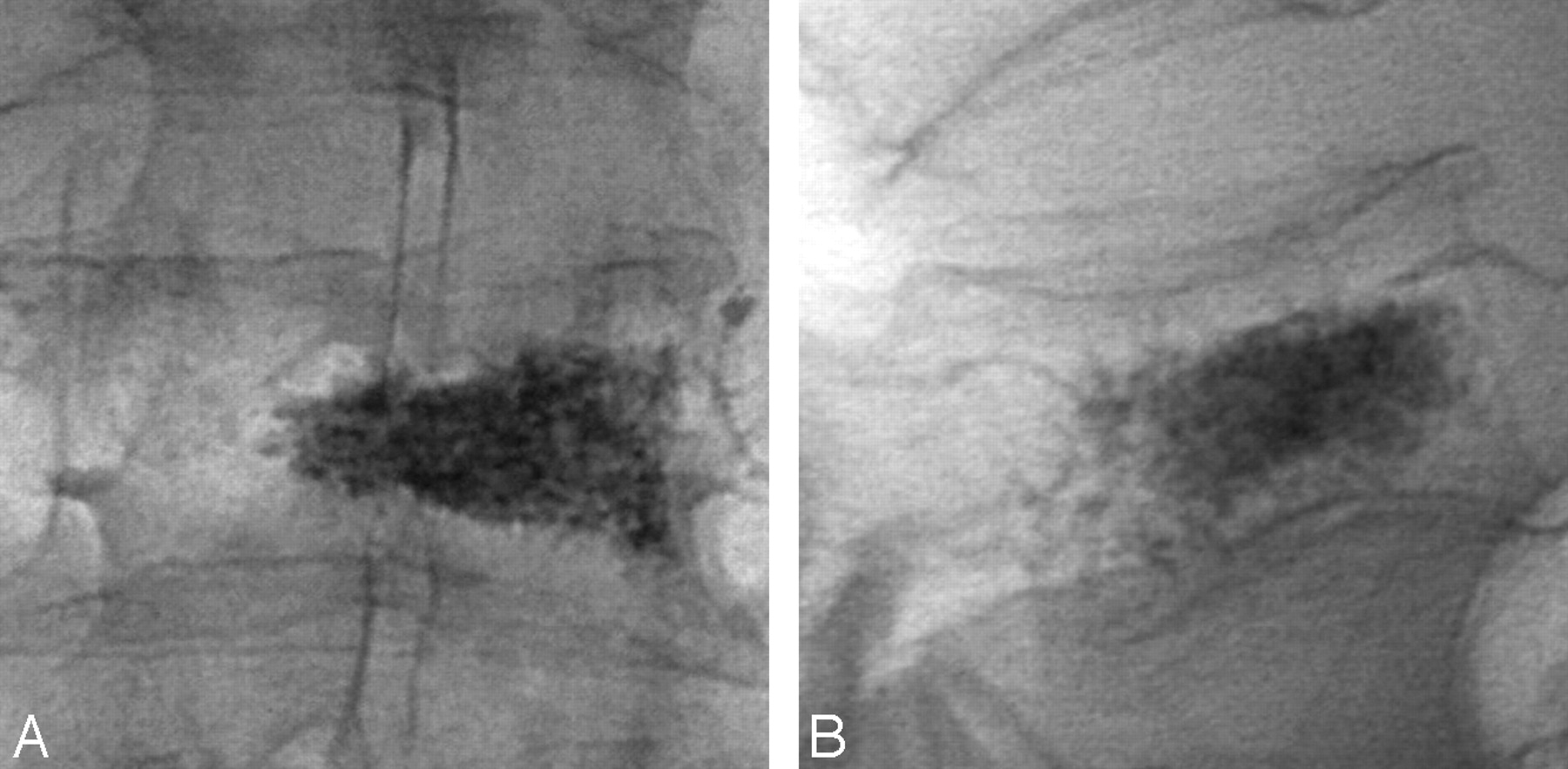
We defined “hemivertebroplasty” in patients in whom barium-opacified PMMA was present predominantly in 1 side of the vertebral body (Fig 1). If PMMA crossed the midline, we restricted the definition of “hemivertebroplasty” to patients in whom PMMA traversed only <10% of the width of the predominantly unfilled hemivertebra. Cases that exceeded >10% filling of the unaugmented side of the treated vertebra were excluded from the study (Fig 2).

A, An example of a T12 hemivertebroplasty, anteroposterior view. B, T12 vertebral body, postvertebroplasty lateral view.

A, An example of a vertebroplasty excluded from the hemivertebroplasty classification. Postvertebroplasty anteroposterior view of an L4 vertebral body with >20% filling of the unaugmented side of the vertebra. B, L4 vertebral body, postvertebroplasty lateral view.
We defined 4 groups of patients. We initially divided the data base into patients who underwent single-level vertebroplasty or multilevel vertebroplasty. We divided the single-level vertebroplasty patient group into hemivertebroplasty cases and bilateral vertebroplasty cases. We divided the multilevel vertebroplasty procedures into “hemivertebroplasty” cases, in which ≥1 treated levels were filled in only 1 hemivertebral body, and bilateral vertebroplasty cases, in which all levels were filled in both hemivertebrae. Thus, the definition of a “multilevel hemivertebroplasty” was a patient with at least 1 hemivertebroplasty level, irrespective of the laterality of other treated levels.
Film Review
A radiologic review was performed on all 917 vertebroplasty procedures to identify hemivertebroplasty cases. Two experienced reviewers evaluated immediate postvertebroplasty plain radiographs to characterize patterns of cement deposition. Disagreements were discussed, and consensus readings were achieved.
Outcomes Measurements
Patients were evaluated preoperatively and postoperatively at 2 hours, 1 week, 1 month, 6 months, and 1 year. Visual Analog Scale scores were obtained for “pain at rest” and “pain with activity,” with zero being no pain and 10 being the worst pain ever experienced. Roland-Morris Disability Questionnaire (RDQ) scores were also obtained to assess changes in patient mobility. Patients were monitored, through follow-up telephone conversations, for new fractures and to determine if the level treated needed any additional treatment throughout the follow-up period. Trained nurses in the hospital gathered the preoperative and 2-hour follow-up data, whereas follow-up data at 1 week, 1 month, 6 months, and 1 year were collected over the telephone by trained nurses.
Statistical Analysis
We initially compared all hemivertebroplasty cases, in both the single- and multivertebroplasty groups, to all bilateral vertebroplasty cases. A 1-way t test was used to evaluate the difference in pain scores between these 2 groups at each follow-up time point. We calculated the P value 6 times (preoperative and 5 postoperative follow-up time points) for each pain score (at rest, with activity, and RDQ). A Bonferroni correction was performed, so P < .008 was considered significant. JMP 7.0.1 2007 software (SAS Institute, Cary, NC) was used for all statistical analyses. A statistical power calculation was also performed for pain with activity and RDQ score at 1 month. Survival analysis by using the logrank statistic was performed to compare time to incidence of new fractures, and a hazard ratio was calculated to compare the proportion of incident fractures between groups. Similar comparisons, including clinical outcomes and incident fracture occurrence, were performed between single-level hemivertebroplasty cases and single-level bilateral vertebroplasty cases and between multilevel hemivertebroplasty cases and multilevel bilateral vertebroplasty cases.
Results
Among an initial cohort of 765 patients (917 procedures), we excluded 172 (22%) patients and 198 (21%) procedures because radiographs of their vertebroplasty procedures could not be located.
Forty-two vertebroplasty procedures containing hemivertebroplasties were selected for inclusion in our study, and 677 vertebroplasty procedures were included in the bilaterally filled vertebroplasty group on the basis of radiologic imaging from their vertebroplasty procedures. Among these 42 hemivertebroplasty cases, 11 (26%) were single level and 31 (74%) were multilevel. Among 31 multilevel hemivertebroplasty cases, an average of 2.5 (± 0.5) levels were treated per case. Twenty-eight of these 31 patients had only a single hemivertebroplasty level among their multiple treated levels, whereas 3 patients had 2 hemivertebroplasty levels among their treated vertebrae. Among the 677 bilaterally filled vertebroplasty cases, 441 (65%) were single level and 236 (35%) were multilevel (Table 1). For the entire cohort, there was a significant improvement in all outcomes measures at all time points compared with initial values, as previously reported.4
Characteristics of patients in both bilaterally filled vertebroplasty and unilateral hemivertebroplasty groups
Overall Comparisons (all hemivertebroplasty cases and all bilaterally filled vertebroplasty cases).
Significant improvements in pain and RDQ were seen in both groups at all time points, compared with preprocedure values (data not shown). No significant differences in pain at rest, pain with activity, or RDQ scores were seen between the 2 groups (all hemivertebroplasty cases versus all bilateral vertebroplasty cases) at any time point following vertebroplasty (P > .1 at all time points) (Table 2). Additionally, hemivertebroplasties were not at a greater risk of incident fracture compared with bilaterally filled vertebrae (hazard ratio = 0.81; 95% confidence interval, 0.33–2.65).
Pain (0–10) and RDQ scores in hemivertebroplasty versus bilateral vertebroplasty groups
Single-Level Treatments (single-level hemivertebroplasty versus single-level bilaterally filled vertebroplasty cases).
Significant improvement in pain and RDQ was seen in both groups at all time points, compared with preprocedure values (data not shown). There was no significant difference in time to and incidence of new fractures (logrank, 0.5; hazard ratio, 0.62; 95% confidence interval, 0.19–3.8) (Table 3).
Incident fracture rates
Multilevel Treatments (multilevel hemivertebroplasty versus multilevel bilaterally filled vertebroplasty cases).
There was no significant difference in time to and incidence of new fractures (hazard ratio = 1.02; 95% confidence interval, 0.3–6.3) (Table 3).
Refracture of Treated Vertebral Bodies.
There were no new fractures of the hemivertebroplasties, whereas 5 (0.7%) of 677 patients with bilateral vertebroplasties returned for addition of PMMA into the treated level.
Technical and Adverse Events
There were no clinically evident adverse events among the hemivertebroplasty group. Technical events, including extravertebral PMMA leakage, were seen in 169 (25%) of 677 procedures in bilaterally filled and in 9 (21%) of 42 hemivertebroplasty procedures. All extravasation of cement was asymptomatic, and the inadequate infusion of cement did not affect the outcome of the procedure because the patient had complete resolution of pain by the 2-year follow-up.
Discussion
The current study was performed to determine whether half-filled vertebral bodies, or “hemivertebroplasty” cases, achieved outcomes similar to cases with filling of both sides of the vertebral body with PMMA. Even with central needle placement, cross-filling of PMMA to the contralateral hemivertebra may not be achieved in all cases, prompting some practitioners to place a second needle to fill the unfilled portion of the vertebral body. Our study suggests that it may not be necessary to fill both sides of the vertebral body because in our small cohort of hemivertebroplasty cases, clinical outcomes were similar to those with bilateral filling. Avoiding a second needle placement would speed the procedure and, at least theoretically, might diminish risk of procedure-related complications.
We are unaware of any prior clinical study focused on hemivertebroplasty. Prior work in cadaveric systems has shown that laterally placed and centrally placed injections of cement did not result in significantly different values for the restoration of stiffness or strength. Furthermore, the lateral injections were actually superior to central injections of cement in restoring vertebral height in some cases. Additionally, the authors found that the unaugmented side of a laterally placed injection was not at an increased risk for collapse, as previously thought.3,16,17
Our study has several limitations. The study was conducted retrospectively; thus, it was subject to bias. We uncovered relatively few cases of hemivertebroplasty, likely reflecting the typical pattern in which practitioners placed a second needle in cases in which PMMA did not reach the contralateral hemivertebra. Our data relied on accurate reporting of pain and mobility by our patients. Although we did use well-accepted measuring tools for pain and mobility, our results were the subjective perspectives of our patients. We grouped patients who had both bilateral and hemivertebral filling into the “hemivertebroplasty group,” as noted in the “Materials and Methods” section, so there may be some bias from the bilaterally filled levels in these patients. Additionally, we experienced some losses to follow-up throughout the 2-year follow-up period. This potentially could have had a positive or negative effect on our results. Finally, 6 of the 42 patients underwent vertebroplasty <6 months before completion of this study. Thus, we were only able to obtain information regarding these patients’ outcomes up to their 1-month follow-up.
In the future, a larger prospective randomized trial comparing laterally placed hemifilled vertebroplasties with bilateral fully filled vertebroplasties would be ideal. This would allow us to verify the results attained in this study on a large scale and with a less-biased study methodology. Furthermore, a longer duration of follow-up would be helpful in evaluating the long-term efficacy of laterally placed hemifilled vertebroplasties. Additionally, more complete follow-up data would also increase the integrity of future studies.
Conclusions
Hemivertebroplasty, in which PMMA is instilled in only one half of the vertebral body, was shown in this small retrospective series to be as efficacious as bilateral PMMA infusion. These results may allow practitioners to avoid placement of additional needles to achieve holovertebral body filling.
References
- Received September 11, 2008.
- Accepted after revision October 21, 2008.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}