
Abstract
BACKGROUND AND PURPOSE: Hyperintense basal ganglia on MR imaging support the diagnosis of sporadic Creutzfeldt-Jakob disease (CJD). Our aim was to study the frequency of patients with sporadic CJD presenting with and without characteristic basal ganglia lesions on MR imaging and to examine the corresponding patient characteristics.
MATERIALS AND METHODS: Fluid-attenuated inversion recovery (FLAIR) and diffusion-weighted images (DWI) of 55 patients with CJD were assessed for signal-intensity increase (FLAIR) or restricted diffusion (DWI) in 7 cortex regions and the basal ganglia, thalamus, and cerebellum. Patient characteristics as well as electroencephalography, CSF, and codon 129 genotype of the prion protein gene (PRNP) were correlated with the most frequent MR imaging lesion patterns.
RESULTS: Two major lesion patterns were identified by DWI: cortex and basal ganglia involvement (two thirds) and isolated cortex involvement (one third). In the latter patient group, the cortex involvement was widespread (at least 3 regions affected in 89% on DWI) and usually included the frontal and parietal lobes (78%). The length of the disease course was significantly prolonged (median, 12 versus 5 months). No significant differences were observed concerning electroencephalography and CSF findings and codon 129 genotype distributions. Of 4 patients with normal MR imaging findings, the CSF was positive for the 14-3-3 protein in 3.
CONCLUSION: A high number of patients with CJD present without basal ganglia lesions on MR imaging. Isolated cortex involvement on DWI and FLAIR should lead to suggestion of CJD, even if the disease course is only slowly progressive. Additional 14-3-3 protein analysis in the CSF may support the CJD diagnosis.
Sporadic Creutzfeldt-Jakob disease (CJD) is a rare and fatal disease caused by the accumulation of abnormal/pathologic prion protein (PrPSc; Sc indicates scrapie) in the human brain. The classic disease type is characterized by rapidly progressive dementia, ataxia, abnormal muscle tone, and myoclonus. It leads to a state of akinetic mutism and death after a median disease duration of 6 months.1 The definite CJD diagnosis relies on the finding of PrPSc in the brain tissue, together with astrocytic gliosis, nerve cell loss, and spongiform degeneration as the typical neuropathologic changes.2,3
During one's lifetime, MR imaging hyperintensity of the basal ganglia on T2-weighted (T2WI), fluid-attenuated inversion recovery (FLAIR), and diffusion-weighted imaging (DWI) is increasingly used to support the CJD diagnosis, next to positive CSF (14-3-3 protein) and electroencephalography (EEG) findings of periodic sharp-wave complexes (PSWCs). Although the origin of the signal-intensity changes is still not fully understood, hyperintensity on T2WI and FLAIR has been thought to be caused by gliosis, whereas abnormalities on DWI are most likely derived from spongiform changes.4–6 DWI was shown to be the most sensitive sequence in the detection of brain lesions, particularly in the neocortex.7–10 Isolated cortex involvement was also found.9,11
Although abnormal MR imaging findings in CJD have been studied in detail with respect to their location, few attempts have been made to define the most frequently occurring patterns of hyperintensity in a spectrum of patients. Six disease phenotypes (MM1, MM2, MV1, MV2, VV1, and VV2) defined by the codon 129 genotype (MM, MV, VV) of the prion protein gene (PRNP) and pathologic isotype of the PrPSc type 1 or 2 have been recently described with distinctive neuropathologic features and various clinical and diagnostic findings.1–3,12 On MR imaging, predominant cortical (VV1)13 or subcortical involvement (MV2 and VV2)14,15 or no abnormalities (MM2)16,17 were found in smaller case series.
To date, to our knowledge, the overall distribution of MR imaging abnormalities has not been studied in a larger spectrum of patients with CJD, and it is unclear whether there are clinical correlates corresponding to specific MR imaging lesion patterns. The proportion of patients presenting without basal ganglia abnormalities is unknown.
We defined the most frequent MR imaging lesion patterns and corresponding clinical characteristics in a CJD patient collective by using highly sensitive MR images, and we considered a possible influence of the codon 129 genotype of the PRNP. We particularly focused on patients lacking basal ganglia abnormalities on MR imaging and suggested criteria that might support the early CJD diagnosis in these patients.
Materials and Methods
Patients
Patients with suggested CJD in Germany are reported to the National TSE (Transmissible Spongiform Encephalopathy) Reference Center in Göttingen. After notification, these patients are examined by a study physician at the hospital reporting the patient. Copies are made of the medical charts (clinical findings, laboratory tests) as well as EEG and MR imaging findings, and a neurologic examination is performed. According to the current WHO criteria,18 the diagnosis of possible CJD requires progressive dementia and 2 of 4 typical clinical symptoms (visual and/or cerebellar and pyramidal and/or extrapyramidal symptoms, myoclonus, and akinetic mutism). For probable CJD, characteristic EEG changes (PSWCs) or the presence of the 14-3-3 protein in the CSF or both are additionally required. The definite CJD diagnosis relies on postmortem examination.
The study collective was searched from the years 2000 to June 2005 (predominant use of DWIs from the year 2000 on) by using the MR imaging data base of the CJD Surveillance Unit, Göttingen, Germany. Patients with definite or probable CJD diagnosis for whom a FLAIR and DWI were available from the same examination date were included in the study. Genetic and iatrogenic (CJD) cases were excluded.
Neuropathology
Histologic examination was performed on 4-μm-thick sections of formalin-fixed and paraffin-embedded brain tissue blocks. Hematoxylin and eosin stains, as well as immunochemistry, were performed by using standard techniques. Monoclonal antibodies Gö 138 and L42 were used for immunohistochemical detection of PrPSc.
Genetic Analysis
Analysis of the PRNP was performed after isolation of genomic deoxyribonucleic acid from blood according to standard methods.19 The codon 129 genotype of the PRNP (MM, MV, and VV) was available in 48 of 55 patients.
EEG and CSF
EEG recordings were available in 48 patients and were assessed as positive or negative for PSWCs according to the established criteria (generalized periodic sharp waves with 0.5–2/s frequency, 100- to 600-ms duration, and >150–300 μV of amplitude).20 CSF samples were available in all 55 patients. The 14-3-3 protein immunoassays by means of Western blotting were performed at least twice in each sample as described previously.21
MR Imaging
The MR images were collected from various hospitals in Germany (in the framework of the epidemiologic study) and obtained from scanners of different manufacturers (mainly Siemens, Erlangen, Germany; Philips Medical Systems, Best, the Netherlands; Marconi Medical Systems, Cleveland, Ohio; Picker International, Cleveland, Ohio; and GE Medical Systems, Milwaukee, Wis) and of different magnetic field strengths of 0.5–2.9T (mainly 1.5T). The manufacturer's standard sequences were applied. The individual technique (single-shot, multishot, echo-planar imaging, stimulated echo) and the b-values (up to 4 b-values: 0.333, 666, 1000, maximal 1500 s/mm2; b = 1000 s/mm2 was most common) depended on the local facility (eg, gradient system) and individual preferences. All scans were assessed by a neuroradiologist (K.K.) who was aware of the CJD diagnosis. Because the reliability of the neuroradiologic evaluation was reported to be high, the scans were rated by 1 neuroradiologist only.8 For each patient, the FLAIR-weighted scan was assessed first, followed by DWI. Proton-attenuation–weighted scans and apparent diffusion coefficient maps were less commonly used and were not included in this study. The brain regions were evaluated as hyperintense in relation to suspected normointense brain tissue according to a standardized protocol, including 7 cerebral cortex regions (frontal, parietal, temporal, occipital regions and the cingulate gyrus, insula, and hippocampus), basal ganglia (caudate nucleus, putamen, globus pallidus), thalamus, and cerebellar cortex. The quality of the complete MR imaging examination was graded from 1 to 6 (1 = excellent, 2 = good, 3 = average, 4 = sufficient, 5 = insufficient, 6 = poor), according to individual subjective criteria (eg, due to motion or metal), technique (sequence parameters: T2WI half-Fourier acquired single-shot turbo spin-echo protocol of the brain, acquisition time, resolution, inversion recovery pulse), homogeneity, differentiability of gray and white matter, postprocessing (eg, filtering, smoothing), and, in case of hard copies, also the selected window and the absolute image size. Scans graded worse than 4 were considered as nondiagnostic and excluded from the study. If serial MR images were available, the first examination was used for the study.
Statistical Analysis
For statistical analysis, the program Statistica was used. Fisher exact and Mann-Whitney U tests were used to assess differences between qualitative and quantitative variables, respectively. For comparison of brain regions showing abnormal signal intensity on FLAIR or restricted diffusivity on DWI, the McNemar test was used.
Results
Study Collective
In the years 2000 to June 2005, 55 patients with probable (n = 24) or definite (n = 31) sporadic CJD fulfilled the inclusion criteria. The group consisted of 28 men and 27 women. The median age of all patients was 63 years (range, 29–79 years), and the median disease duration was 6 months (range, 1–41 months). Analysis of the codon 129 genotype most frequently revealed the MM genotype (63%), followed by MV (25%), and VV (13%) (Table 1).
MR imaging lesion patterns on DWI* and patient characteristics
MR Imaging
MR imaging was performed after a median of 3 months (range, 10 days to 22 months) after the onset of symptoms. The overall quality of the scans was graded as good (overall score = 2). A synopsis of the MR imaging findings as detected by FLAIR and DWI is given in Table 2. DWI was the most sensitive technique, showing basal ganglia lesions in 60% (47% on FLAIR) and cortical lesions in 91% (76% on FLAIR). Lesions were spotted as early as 10 days after the onset of symptoms (cortex and basal ganglia on DWI and FLAIR). In 5 of 55 patients, lesions were only visible on DWI (3 isolated cortical lesions, 2 cortex and basal ganglia lesions). In 4 patients, basal ganglia lesions were seen only on DWI. In 2 patients, only FLAIR showed this finding.
MR imaging sensitivity: comparison of FLAIR and DWI
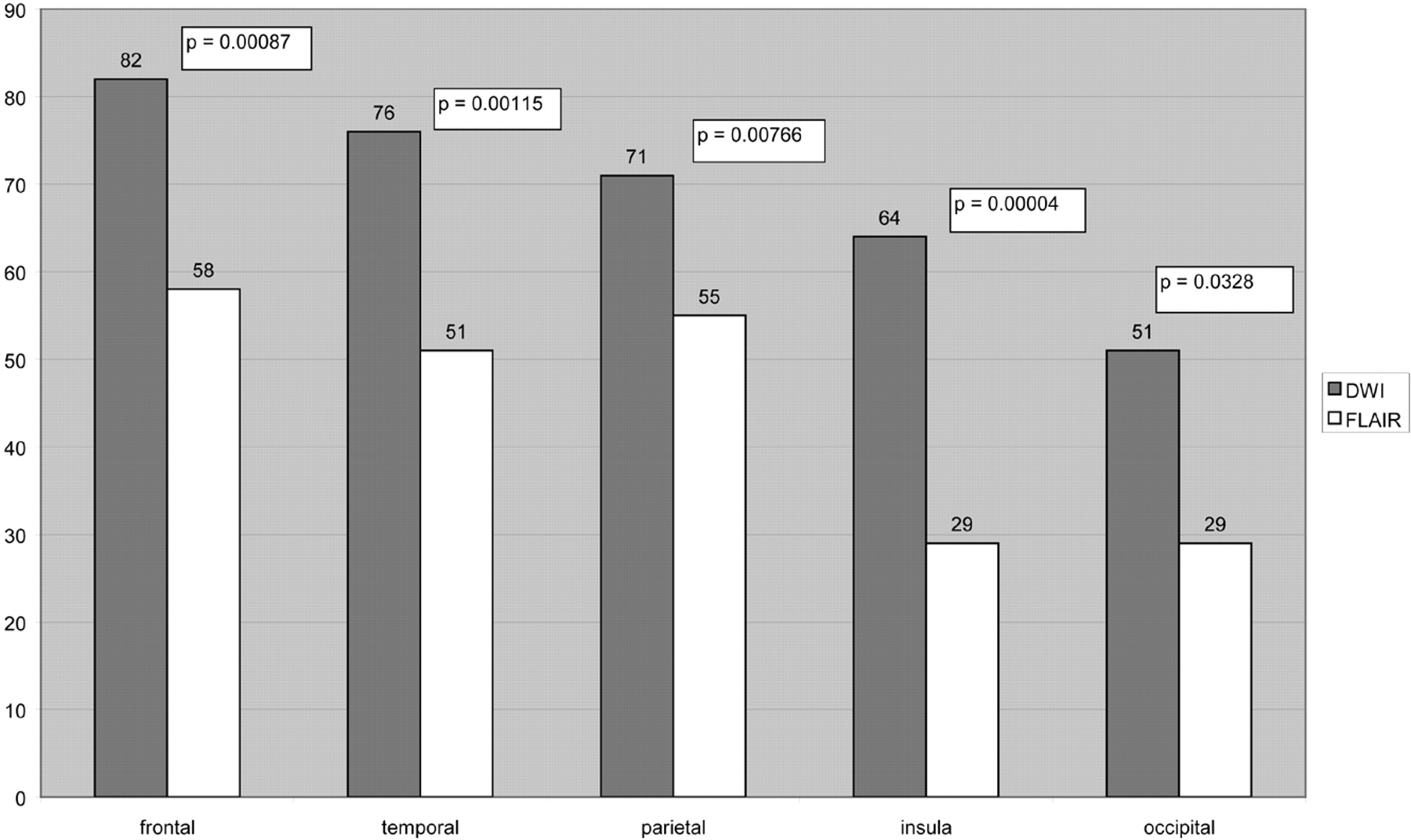
In 8 of 55 patients, cortical involvement was displayed only on DWI. In these patients, the frontal lobes were affected most frequently (7/8), followed by the cingulate gyrus (5/8) and the temporal and parietal lobes (4/8, each). In comparison with FLAIR, DWI was significantly more sensitive for the detection of cortical lesions in general (P = .01333) and with respect to the frontal, temporal, parietal, insular, and occipital cortices (Fig 1).

Detection of cortical hyperintensities by FLAIR and DWI in 55 patients with CJD. (The cingulate gyrus and hippocampus are not displayed because the findings were not significant.)
MR Imaging Lesion Patterns and MR Images
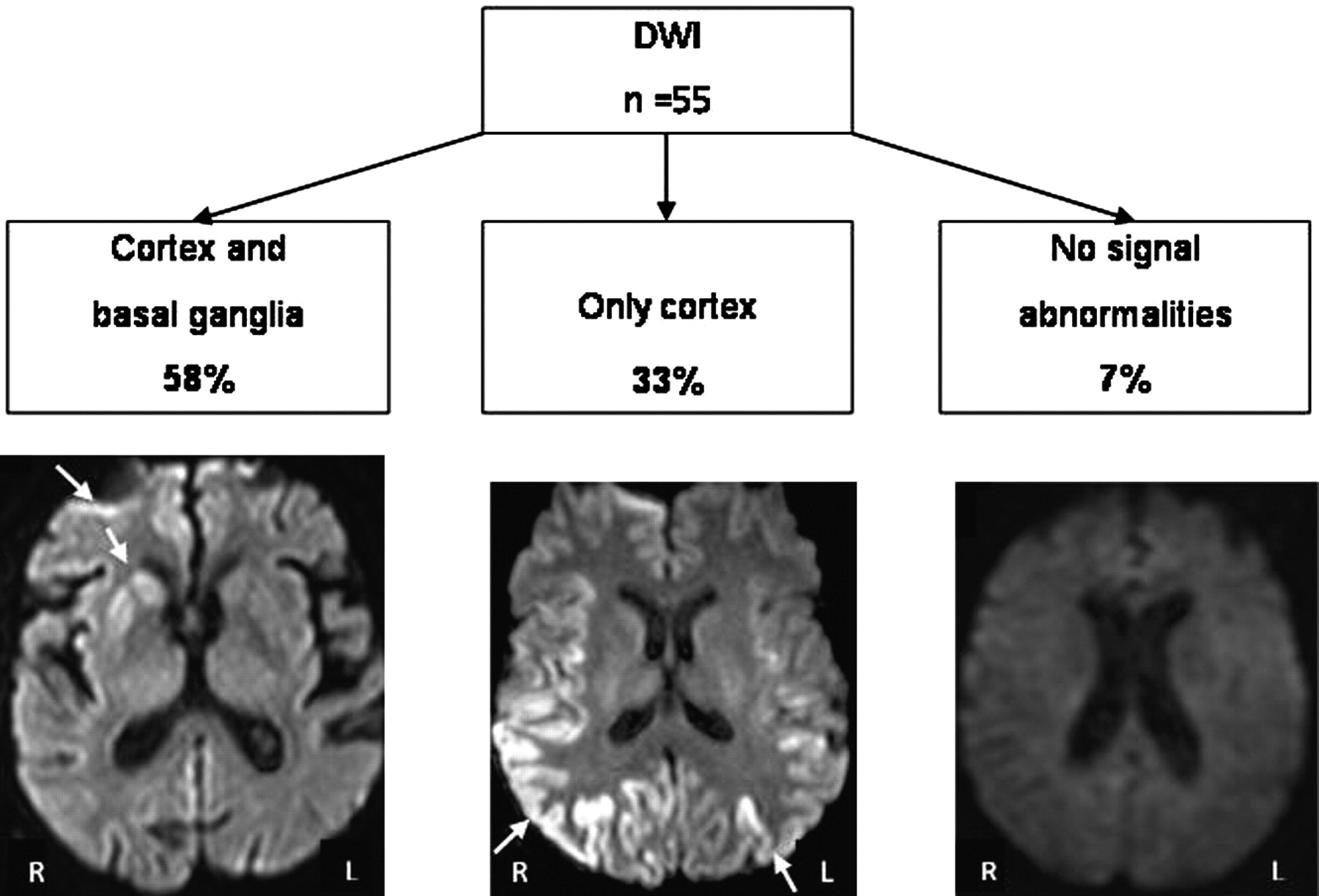
The most frequent MR imaging lesion patterns were defined by using DWI as the most sensitive technique (Fig 2). Cortex and basal ganglia hyperintensity was observed in two thirds (58%) and isolated cortical hyperintensity, in one third (33%) (Fig 3). Normal MR imaging findings were seen in 4 patients (7%).

MR imaging lesion patterns in sporadic CJD depicted by DWI.

Involvement of the frontal and parietal lobes in patients with isolated cortical hyperintensities. A, Sagittal FLAIR-weighted scan of a 58-year-old patient 3.5 months after the disease onset and 1 week before death showing signal-intensity increases of the frontal and parietal lobes. B, Axial FLAIR-weighted scan of the same patient showing frontal and parietal signal-intensity increases. C, Diffusion-weighted scan of the same patient showing frontal and parietal signal-intensity increases.
The MR imaging lesion patterns obtained for each sequence are summarized in Table 3.
Spectrum of MR imaging lesion patterns in 55 patients with sporadic CJD
Findings on FLAIR and DWI were not completely congruent: The FLAIR sensitivity for the cortex and basal ganglia was reduced (compared with patients showing that pattern on DWI), because in 3 patients, only basal ganglia hyperintensity was found, and in 2 patients, no signal-intensity changes were detected. Six patients with isolated cortex involvement on FLAIR showed basal ganglia lesions on DWI. Three patients with isolated cortical hyperintensity on DWI had normal findings on FLAIR images.
Isolated Cortical Hyperintensity on the MR Imaging
The most frequently observed patterns of cortical hyperintensity are given in Table 4. On DWI, the frontal and parietal lobes were most frequently affected (89%, each), followed by the temporal (72%) and occipital lobes (61%) (data not shown). The cortical lesions were widespread, including at least 3 regions in 89% of the patients. The frontal and parietal lobes were most frequently affected in combination (78%) (Fig 3). Hyperintensity of only 1 region (the temporal lobe) on DWI was found in a single patient.
Distribution of cortical lesions in patients with isolated cortical hyperintensity
On FLAIR, the frontal lobes (79%) were most frequently affected, followed by the parietal lobes and the cingulate gyrus (63% each) (data not shown). Combined hyperintensity in the frontal and temporal lobes was the most frequently occurring pattern (53%). A higher rate of signal-intensity increase in the hippocampus (42%) was found compared with DWI (28%).
MR Imaging Lesion Patterns and Clinical Findings
Clinical data on patients with various MR imaging lesion patterns on DWI are displayed in Table 1. In patients with cortex and basal ganglia hyperintensity on MR imaging, the disease course was rapid, whereas in patients with isolated cortical hyperintensity, the disease duration was significantly prolonged (median, 12 versus 5 months, P = .05). No significant differences were found concerning the age at disease onset, sex, codon 129 genotype, EEG, CSF, and time point of the MR imaging examination (P = .23). In 4 of 55 patients, no abnormalities apart from atrophy were found on the MR imaging. The disease duration in these patients was variable (3–38 months). One patient was very young at disease onset (female, 29 years, MM genotype) and had the longest disease duration. The CSF was positive for the 14-3-3 protein in 3 of these patients; EEG was positive for PSWC in 1.
Degree of Cortex Involvement and Disease Duration
A possible correlation between the degree of cortex involvement and the disease duration was examined for FLAIR and DWI (data not shown). Patients with >3 cortex regions affected on FLAIR had a significantly prolonged disease duration compared with patients with <3 regions affected (median, 13 versus 4 months, P = .02). On DWI, no such correlation was found (median, 8 versus 6 months, P = .68).
Discussion
We analyzed the spectrum of MR imaging and clinical findings in a collective of CJD patients with FLAIR and DWI available and were able to define 2 major lesion patterns: combined cortex and basal ganglia hyperintensity (two thirds of all patients) and isolated cortical involvement (one third). In the latter patients, the disease course was significantly prolonged compared with patients with cortex and basal ganglia lesions. The codon 129 genotype distributions and EEG and CSF findings did not differ significantly between both groups.
In previous studies, basal ganglia abnormalities on T2WI were shown to correlate with rapidly progressive dementia and short disease duration, whereas in patients lacking this finding, the onset of dementia was delayed and the disease course was prolonged.22,23 Using highly sensitive sequences, we were now able to identify isolated cortex involvement on DWI as a main lesion pattern in CJD correlating with prolonged disease duration. The findings on DWI at the time point of the diagnosis may thus indicate a rather slowly or rapidly progressive disease course. Although the presence of basal ganglia hyperintensity, on the whole, may represent a negative prognostic factor, there may be single disease variants (determined by codon 129 genotype of the PRNP and the type of PrPSc with prolonged disease duration showing basal ganglia lesions on MR imaging.14
Because patients with CJD with only cortical hyperintensities and atypical clinical presentation may be diagnosed with delay, the risk of disease transmission through invasive diagnostic procedures, such as brain biopsies, is present. CJD should, therefore, be considered as well in cases of slowly progressive dementia without characteristic basal ganglia abnormalities. Follow-up MR imaging examinations should be performed because they may show characteristic basal ganglia lesions in the later disease stage.24
Isolated cortex involvement on DWI has been reported in other conditions, such as encephalitis,25–27 hypoxia,28 and epilepsy.29–32 In these cases, further radiologic signs, such as cortical swelling, contrast enhancement on T1-weighted images, absence of hyperintensities on conventional images, predilection sites (hippocampus), and the partly observed resolution of the findings during the disease course may be useful discriminating factors from CJD.
In other cognitive disorders, used in the main differential diagnosis of CJD, isolated involvement of the neocortex was found in 17% of patients, mainly in the limbic cortex (25%) but also in the temporal (11%) and frontal lobes (9%). The parietal and occipital lobes were rarely affected (3% and 2%) (lesions not assigned to a single diagnosis).9 As a major distinctive criterion, patients with CJD in our study showed more widespread cortex involvement on DWI, which typically included the frontal and parietal lobes (78%). Similar cortical lesions, particularly on DWI, have, to our knowledge, not been described in other neurodegenerative diseases and may thus be useful in differentiating CJD from other dementias.
No MR imaging abnormalities apart from atrophy were detected in 4 of our patients with variable disease duration. Single reported cases with negative findings on DWI imply that the absence of signal-intensity alterations may be related to a very early or late examination time point33,34 or the findings may be too subtle or hard to differentiate from artifacts.9,35 Negative findings on all applied MR images have been reported in a rare variant of sporadic CJD.16,17 The CSF was positive for the 14-3-3 protein in 3 of our patients with normal MR imaging findings and may thus be a useful complementary diagnostic investigation.
In 8 patients in our study showing abnormalities only on DWI, the frontal, temporal, and parietal lobes were affected. Because DWI has already been reported to show signal-intensity alterations early in the disease course,33 this finding might reflect the onset of the disease in these brain areas and might match the early neuropsychologic deficits observed in patients with CJD.36,37
DWI, in contrast to FLAIR, depicted a significantly higher rate of high signals in the frontal, temporal, parietal, and occipital lobes as well as in the insula. This discrepancy may be explained by the neuropathologic lesions underlying the signal-intensity changes: Only predominant gliosis with a lower degree of spongiform changes gave high signals on T2WI in a hamster model.6 Because FLAIR is actually a T2WI MR imaging (without free fluids giving signal intensity), it most likely shows gliotic changes, as well. In contrast, DWI abnormalities are most probably caused by spongiform degeneration leading to decreased water diffusion due to the small size of the vacuoles.4,5 We assume that vacuoles are the predominant neuropathologic feature in the early disease stage, correlating with higher DWI sensitivity. Reactive gliotic changes may become more prominent during the disease course, causing high signals on FLAIR. Serial MR imaging studies with lesions detected first by DWI and only later by FLAIR and T2WI support this hypothesis.24,38,39
A correlation between widespread cortical hyperintensity on FLAIR and prolonged disease duration was found in the patients in our study. This finding supports the idea that widespread gliotic changes causing high signals on FLAIR are rather found in the advanced disease stages. Concerning DWI, no such correlation was found, which may be due to the small patient number with only little cortex involvement on DWI in our study.
An influence of the codon 129 genotype of the PRNP and the PrPSc isotype 1 or 2 (molecular subtype) on MR imaging findings in CJD has been postulated in small case series.13–17 Because, as in our study, the overall genotype distribution did not differ significantly between patients with and without basal ganglia signal-intensity increase on MR imaging, we assume that the PrPSc isotype may represent a major influencing factor on the neuropathologic lesion distribution and, consecutively, the signal intensity alteration patterns on the MR imaging. The role of the molecular subtype concerning MR imaging lesion patterns in CJD should be evaluated in further studies including sufficient case numbers for each type.
Conclusions
The proportion of patients with CJD presenting without basal ganglia abnormalities is high, even when DWI is applied. Isolated cortical hyperintensities, as seen in one third of the patients, should be recognized as a frequently occurring pattern on the MR imaging, which might be characteristic of atypical disease variants with a slowly progressive course. Involvement of the frontal and parietal lobes as a consistent finding on FLAIR and DWI may support the CJD diagnosis. CSF analysis for the 14-3-3 protein may represent a useful complementary test in patients without signal-intensity abnormalities or with isolated cortical hyperintensity on MR imaging.
Acknowledgments
We thank all the physicians who reported suggestive cases to the German CJD Surveillance Unit for providing pertinent clinical and especially neuroradiologic data. We also thank Dr. Walter Schulz-Schaeffer and Prof. Hans Kretzschmar for contributing neuropathologic data and Jolanthe Ehrlich, Maja Schneider-Dominco, and Christine Crozier for the valuable assistance in the data management and editing of the manuscript.
Footnotes
Authors B.M. and K.K. contributed equally to this work.
This work was supported by grants from the Federal Ministry of Education and Research (BMBF 01GI0301 and KZ: 0312720), Federal Ministry of Health (BMG Az325-4471-02/15), and Robert Koch Institute through funds of the Federal Ministry of Health (grant no. 1369-341).
References
- Received December 25, 2007.
- Accepted after revision March 12, 2008.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Towards an early clinical diagnosis of sporadic CJD VV2 (ataxic type)
- Neuroimaging of Rapidly Progressive Dementias, Part 2: Prion, Inflammatory, Neoplastic, and Other Etiologies
- Combined Diffusion Imaging and MR Spectroscopy in the Diagnosis of Human Prion Diseases
- Enhanced Detection of Diffusion Reductions in Creutzfeldt-Jakob Disease at a Higher B Factor
- MRI lesion profiles in sporadic Creutzfeldt-Jakob disease