
Abstract
BACKGROUND AND PURPOSE: Aneurysm recurrence is an innate problem after coiling, and the recurrence rate is higher in complicated aneurysms. We evaluated the feasibility and efficacy of using the Willis covered stent in treating recurrent aneurysms after coil embolization.
MATERIALS AND METHODS: Eight aneurysms in 8 patients treated with detachable coils had confirmed recurrent aneurysms: 3 giant, 1 large, 1 dissecting, and 3 small wide-necked. The recurrent aneurysms involved C3 in 1 patient, C4 in 1, C7 in 5, and V4 in 1. A total of 11 covered stents were implanted into 8 target arteries. Follow-up angiography was performed 1–16 months after the procedure. Clinical follow-up data were collected and retrospectively analyzed, grading as fully recovered, improved, unchanged, or aggravated.
RESULTS: Willis covered stent placement succeeded technically in all of the aneurysms. No technique-related adverse event occurred. Total occlusion was achieved immediately in 6 aneurysms, and a small endoleak was observed in 2 aneurysms. No mortality or morbidity occurred during or after the procedures, including during the follow-up period. Follow-up angiograms revealed that all 8 of the recurrent aneurysms were completely isolated, and 8 parent vessels kept patency, except 1 with mild stenosis. Clinical neurologic symptoms fully resolved in 5 patients, improved in 1, and were unchanged in 2 at the end of the follow-up period.
CONCLUSIONS: In this small study with a middle-term follow-up, the Willis covered stent was used safely and effectively to occlude recurred aneurysms after coiling. Longer-term follow-up and additional clinical experience are needed to fully determine the safety and efficacy of the device.
Endovascular coil embolization is an effective and popular technique in treating ruptured or unruptured aneurysms. However, aneurysm remnants or recurrence is an inherent problem with coil embolization. Follow-up angiography in previous large cohort studies revealed recurrence rates varying from 4.7% to 28.6% in coil-treated aneurysms.1–5 This rate is higher in giant, large, dissecting, and wide-necked aneurysms. Aneurysm reopenings may expose patients to the risk of hemorrhage. Most recurrent aneurysms can be treated by recoiling with or without balloon or stent assistance, but for complicated aneurysms, like giant or very large aneurysms and dissecting aneurysms, coil re-embolization techniques do not typically solve the problem.6–8 Here, we demonstrate an advanced new reconstruction technique by using the Willis covered stent (MicroPort, Shanghai, China) to completely occlude recurrent aneurysms from the normal circulation.
Materials and Methods
Human Rights Statement
All of the human studies in our pilot program were approved and supervised by the ethics committee of our hospital. All of the patients gave written informed consent before their inclusion in the study.
Patients and Recurrent Aneurysms
From April 2005 to October 2007, 8 recurrent aneurysms after coiling in 8 patients were treated by using Willis covered stents in our department, the Sixth Affiliated People's Hospital of Shanghai Jiao Tong University. Patient ages ranged from 33.0 to 51.0 years (mean, 43.6 years); there were 4 men and 4 women. These 8 recurrent aneurysms consisted of 3 giant, 1 large, 1 dissecting, and 3 small wide-necked aneurysms; 5 aneurysms were located in C7 of the internal carotid artery (ICA), 1 was located in C3 of the ICA, 1 in C4 of the ICA, and 1 in V4 of the vertebral artery (VA). Of the 8 aneurysms, 5 were degenerative saccular aneurysms, 2 were pseudoaneurysms caused by trauma, and the remaining 1 was a dissecting aneurysm. The initial result after coiling was total or near total occlusion in 3, subtotal occlusion in 3, and partial occlusion in 2 patients. The recurrence type after coiling based on follow-up angiographic images was aneurysm reopening in 3 patients and enlargement of the residual sac in 5 patients. Seven patients had neurologic symptoms after coil embolization, such as intermittent or repeated headache, diplopia, tinnitus, oculomotor (III), trochlear (IV), abducent (VI) nerve paralysis, and eyesight loss. In 5 symptomatic patients, the primary cause of symptoms was due to the mass effect of the aneurysm after coiling (Table).
Summary of treatment with Willis covered stent in 8 patients with recurrent aneurysm after coiling
Covered Stents
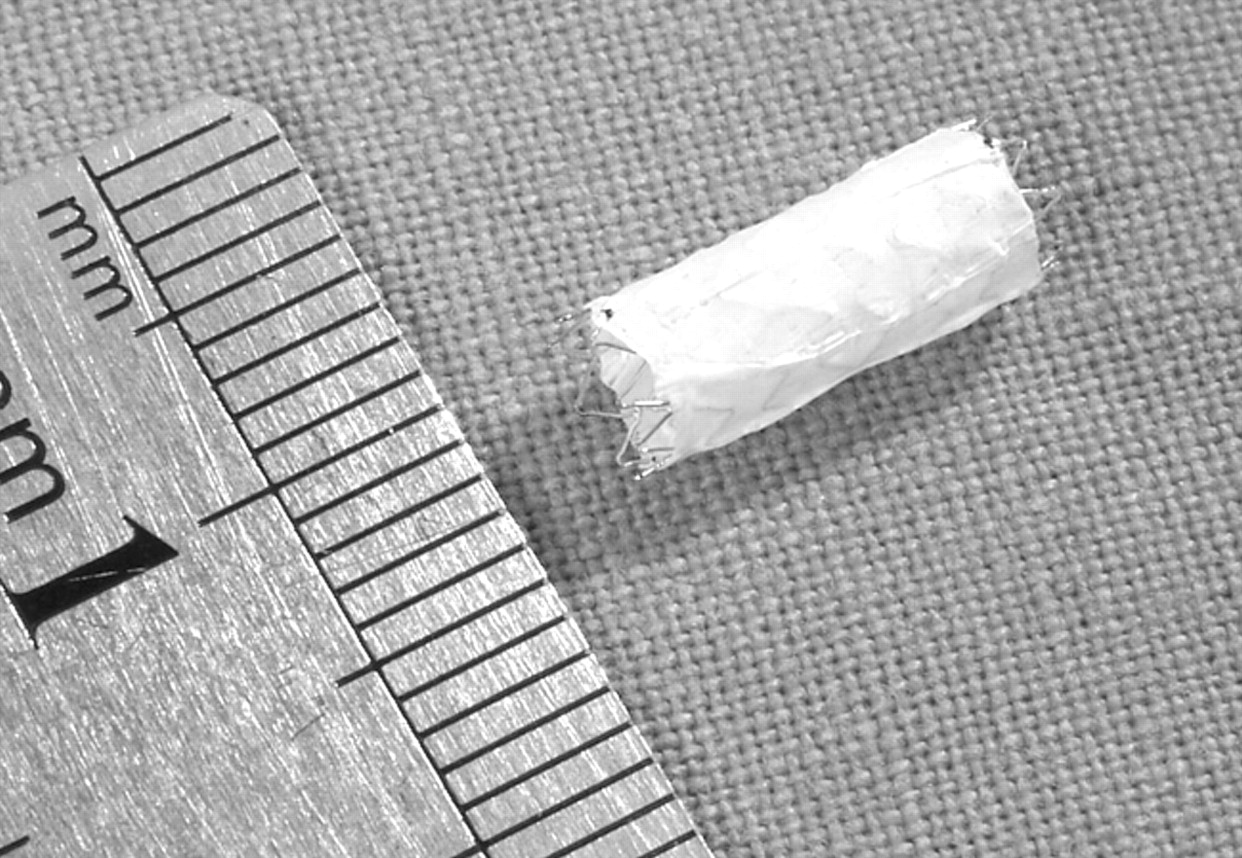
The Willis covered stent that we used in the study was specially designed for intracranial vasculature applications (Fig 1).9 It consists essentially of 3 parts: a bare stent, an expandable polytetrafluoroethylene (ePTFE) membrane, and a low-pressure flexible balloon catheter. This new stent system is uniquely suited to facilitating intracranial applications, because multiple stent bodies can be connected to the next at the 2 asymmetric points between the crest wall to enhance the flexibility of the stent, the ePTFE membrane is extremely thin and in a tubular configuration (thickness of 30–50 μm), the balloon has 5 valves instead of the commonly used 3 to prevent it from scaling the inner wall of the stent when withdrawing, the whole body of the stent is radiopaque under the fluoroscope to facilitate precise placement of the stent, and it is available in various diameters (from 3 to 5 mm) and lengths (from 7 to 19 mm).

Photograph of the Willis covered stent with complete expansion and deployment.
Stent Deployment Procedure
Considering the possibility of occasional events, including acute thrombosis and stent displacement or migration during or after the stent deployment, a balloon occlusion test (BOT) was performed before the covered stent procedure in all 8 of the patients. After getting an acceptable tolerance on the BOT, endovascular treatment was performed under general anesthesia via a right femoral approach. A 6F sheath was placed into the right femoral, and selective catheterization of the ICA or VA was performed by using a 6F guiding catheter (Envoy; Cordis, Miami Lakes, Fla). A 300-cm-long and 0.014-in-diameter microguidewire (Transcend Floppy; Boston Scientific, Natick, Mass) was navigated into the distal branch of the parent artery, with or without microcatheter, under the guidance of the roadmap. The Willis covered stent system was then advanced over the microguidewire, with the proximal and distal ends of the stent bridging the aneurysm orifice of the parent artery. Multiple control angiographies were obtained during the procedure to confirm the aneurysm orifice by the stent. Under fluoroscopic control, the stent was then deployed across the aneurysm orifice with 5–6 atm of pressure. If the aneurysm orifice was not completely covered, and a fast filling of the aneurysm cavity was observed, then another covered stent was used to cover the orifice of endoleak adjacent to the first stent. However, if immediate angiography demonstrated only slow and slight filling of the aneurysm lumen, no further treatment was needed, because significant rerouting of hemodynamics may prompt spontaneous thrombosis, eventually occluding the aneurysm sac completely.
Before the stent was introduced, a bolus of 4000–5000 U of heparin was intravenously injected, and an additional 1000 U were added every hour to maintain heparinization conditions during the procedure. Nimodipine (10 mg) diluted in 250 mL of saline was intravenously transfused during the procedure to prevent intracranial vasospasm. Nonenhanced brain CT scans were performed to occlude any intracranial hemorrhage or ischemic event, and detailed neurologic examinations were conducted preprocedure and postprocedure. All of the patients received double-antiplatelet therapy, with oral 75 mg/d of clopidogrel and 100 mg/d of aspirin, for at least 3 days before the procedure, and a dose of 5000 U of low-molecular-weight heparin was subcutaneously injected per 12 hours for 3 days postoperation, followed by an antiplatelet therapy plan for at least 6 months.
Angiographic and Clinical Evaluation
CT scans were conducted before discharge of all the patients and were performed whenever neurologic symptoms deteriorated or acute stroke was suspected in the clinic. Angiography data immediately after the procedure were reviewed by 2 experienced neuroradiologists, and cases were categorized as completely occluded, without any endoleak (excellent), subtotally occluded, with slow and slight endoleak (good), and incompletely occluded, with an obvious endoleak (poor). During 1 to 16 months after the procedure, both aneurysm recurrence and parent artery stenosis were assessed by follow-up angiograms. Clinical follow-up data were collected and retrospectively analyzed by grading into the following 4 types: full recovery from neurologic symptoms that existed before stent implantation, improved or relieved neurologic symptoms, symptoms unchanged after stent placement, and neurologic symptoms deteriorated or aggravated.
Results
Immediate Postprocedural Results
Endovascular treatment with stent grafts succeeded technically in all of the patients. In total, 11 stents were implanted into 8 target arteries to achieve the reconstruction of parent vessels. All of the stented vessels kept patency, as demonstrated by immediate angiography; 5 aneurysms were completely occluded from the normal circulation immediately after the first stent graft deployment (Fig 2), 1 aneurysm achieved total occlusion when a second stent graft was used, and the remaining 2 aneurysms, covered by 1 stent and 3 stents, still showed slow and slight contrast filling of the cavity, but no additional stent was used, because spontaneous thrombosis may prompt occlusion (Fig 3). Clinical neurologic symptoms fully recovered in 3 patients, improved in 2 patients, were unchanged in 2 patients, and were not aggravated in any patient before discharge.

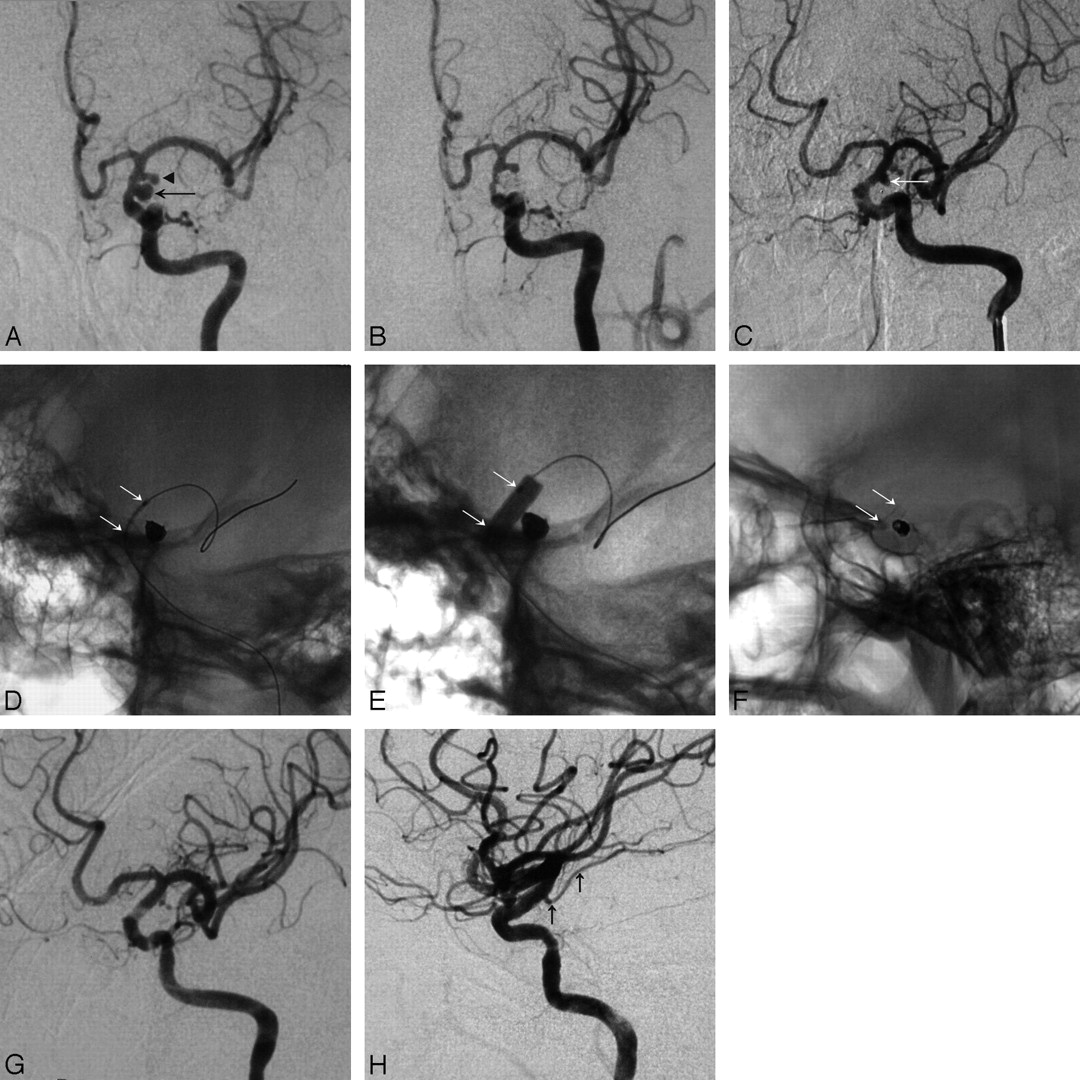
Case 8, a 33-year-old woman with acute subarachnoid hemorrhage. A, Cerebral angiogram revealed a wide-necked aneurysm (arrow) at the origin of the posterior communicating artery (PcomA) and an infundibulum at the origin of AchoA (arrowhead) on the left ICA, respectively. B, The angiogram immediately after balloon-assisted coil embolization showed a subtotal occlusion of aneurysm. C, Recurrence of aneurysm was demonstrated on follow-up angiogram 3 months after coiling (arrow). D–F, Plain film showed the covered stent in place before balloon inflation (arrows), during balloon inflation (arrows), and deployment without balloon inflation (arrows), respectively. G, (slight oblique projection) and F, (lateral projection), Complete disappearance of aneurysm and excellent patency of AchoA (arrows) was shown by immediate angiogram after covered stent placement.

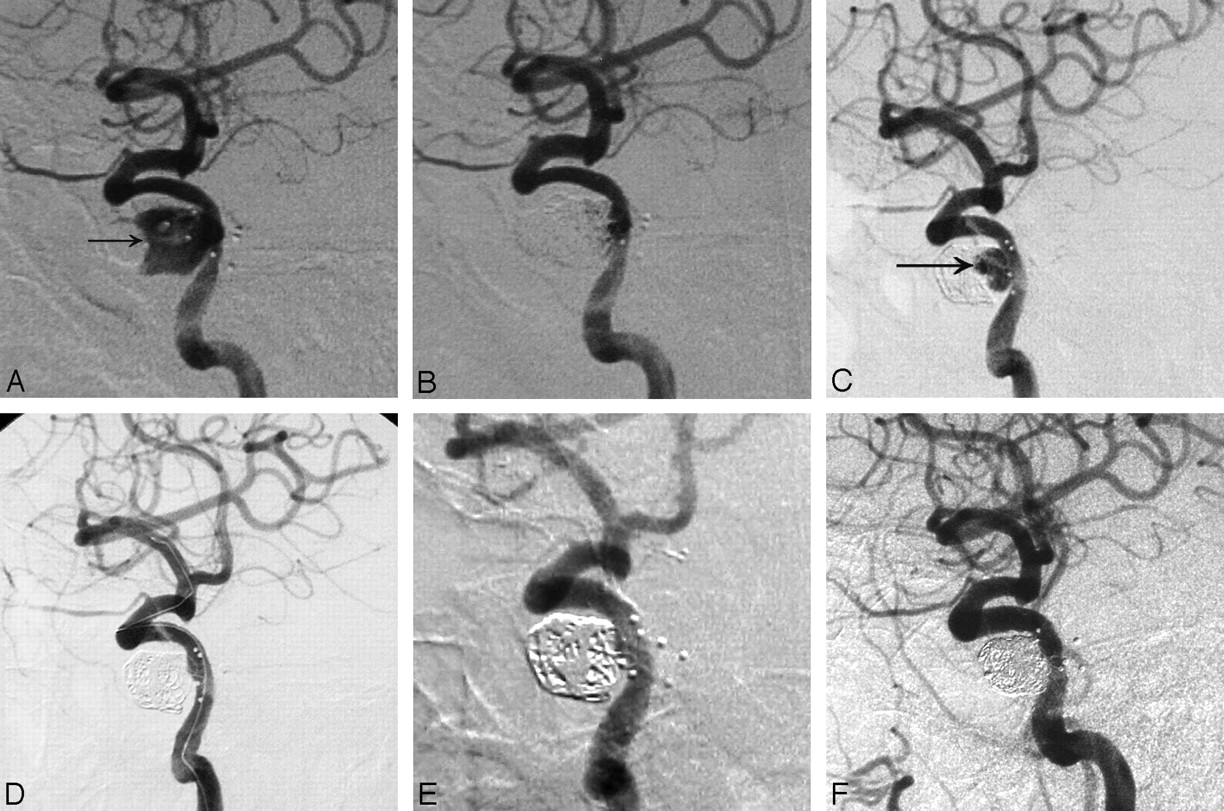
Case 2, a 48-year-old man with a pseudoaneurysm, secondary to postballoon embolization of a carotid cavernous fistula. A, Lateral cerebral angiogram reveals a large pseudoaneurysm (arrow) on the right C3 segment of the ICA at 3 months of angiographic follow-up after balloon embolization. B, The immediate angiogram after coil embolization revealed near total occlusion of the aneurysm. C, The recurrence of aneurysm (arrow) was demonstrated on the 3-month follow-up angiogram after coiling. D, The recurrent aneurysm cavity was totally occluded after the placement of a 4- × 10-mm Willis covered stent. E and F, 3- and 12-month follow-up angiograms showed complete disappearance of aneurysm and excellent patency of the parent artery.
Complications
Obvious intracranial vasospasm was observed in cases 3 and 8 during the procedure, and angiograms demonstrated that the parent arteries became rosary or bead-chain shaped. Urgently, 10 mg of papaverine hydrochloride diluted in 5 mL of saline were infused through the guiding catheter. Later angiograms demonstrated good patency of the cerebral artery and total occlusion of the aneurysm sac. Brain CT scans showed no evidence of intracranial hemorrhage or ischemic stroke immediately after the procedure or during the hospital stay. No other procedure-related complication, such as acute thrombosis, vessel dissection, vessel perforation, or stent migration, occurred. No neurologic event related to the occlusion of side branches or perforating branches, including the ophthalmic artery (OA) and anterior choroidal artery (AchoA), occurred.
Angiographic Follow-Up
Two aneurysms with residual endoleaks demonstrated complete occlusion at the 6-month angiographic follow-up; no recurrence of the aneurysm or occlusion of the parent artery was observed during the 1.0- to 16.0-month (mean, 7.9 ± 5.8 months) angiographic follow-up period. Mild dilation of the stented artery in case 6 (a dissecting aneurysm) could be seen at 3 months (Fig 4) and stenosis (<50%) of the parent artery in 1 patient (case 4) was revealed at 6 months after the procedure.

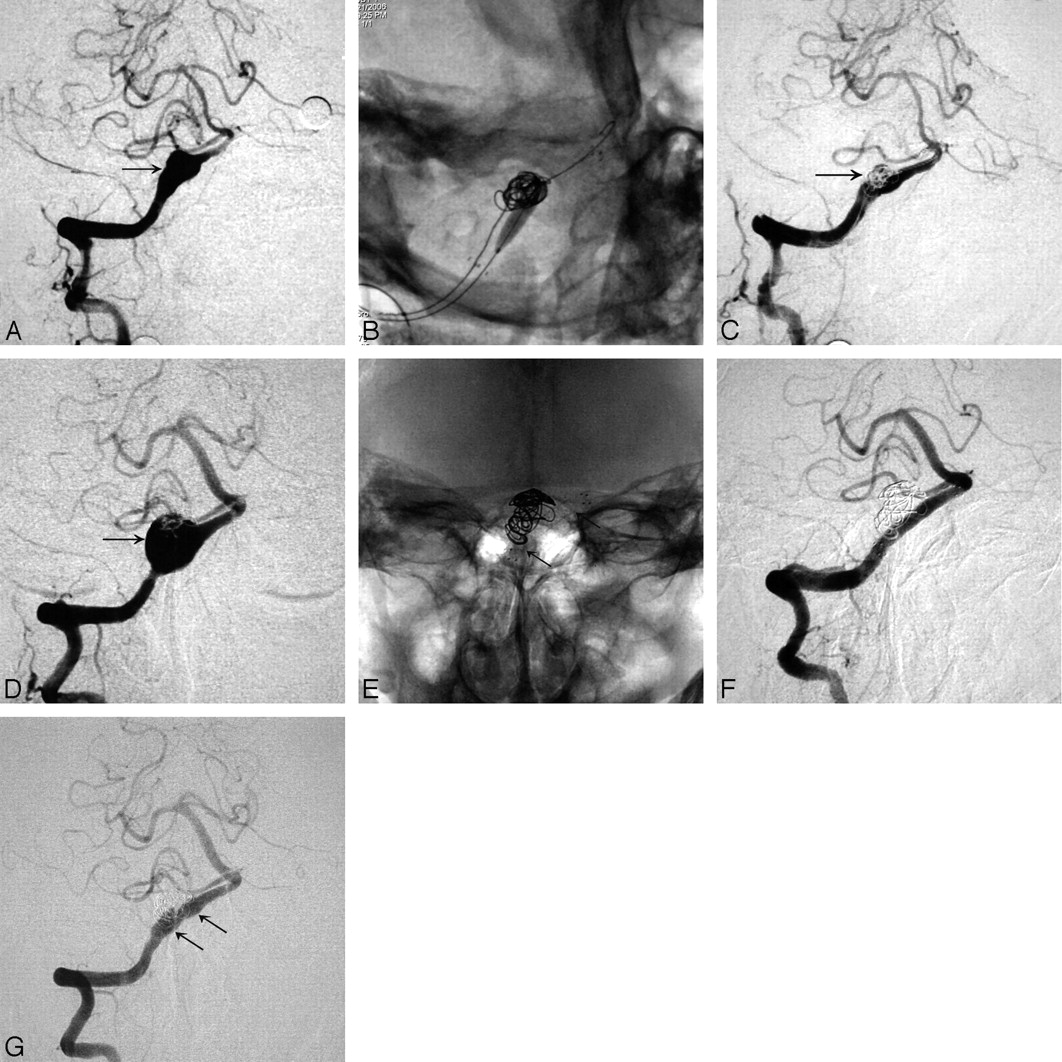
Case 6, a 51-year-old man with acute subarachnoid hemorrhage. A, Anteroposterior cerebral angiogram revealed a dissecting aneurysm (arrow) on the right V4 of the VA. B, Plain film showed balloon-in-stent technique for the coil embolization of aneurysm. C, Immediate cerebral angiogram after coiling revealed subtotal occlusion of the aneurysm (arrow). D, 3-month follow-up angiogram after coiling demonstrated enlargement of the residual aneurysm cavity (arrow). E, Plain film showed deployment of the covered stent after balloon inflation (arrows). F, Total occlusion of the aneurysm sac and excellent patency of the parent artery was shown by immediate angiogram after covered stent placement. G, 3-month follow-up angiogram revealed the disappearance of aneurysm, with mild dilation of parent artery (arrows); this patient was still under close follow-up.
Clinical Follow-Up
Clinical follow-up data were collected for all 8 of the patients; the mean follow-up period was 17.5 ± 12.8 months (range, 1.0–30.0 months), because the covered stent was placed. At the end of our follow-up period, 4 patients had fully recovered, 1 patient had conspicuous improvement in symptoms, 2 patients were essentially unchanged, and no patient had aggravated symptoms. Four patients who presented with neurologic symptoms caused by mass effect were released or disappeared at the end of follow-up time. The remaining unimproved symptoms were primarily vision degradation or eyesight loss, which could not be reversed once the damage occurred. Symptoms such as III, IV, or VI nerve paralysis; diplopia; or headache did recover significantly or completely.
Discussion
For intracranial aneurysms, endovascular coil embolization has now been proven to be a superior alternative to open microsurgery, in terms of disability-free survival at 1 year, according to the large, randomized International Subarachnoid Aneurysm Trial.10,11 Follow-up angiography in previous cohort studies revealed a recurrence rate varying from 4.7% to 28.6% in aneurysms treated with coils.1–5 The primary cause of aneurysm recurrence is incomplete and loose coil packing; other factors include coil compaction or migration, spasm relief in the aneurysm neck and/or parent vessel, thrombus organization, and fibrosis in the aneurysm cavity.1 Giant, large, dissecting, or wide-necked aneurysms treated with coils have a greater propensity to recur; indeed, the rate can reach 87% in giant wide-necked aneurysms and 50% in dissecting aneurysms.6,8
However, the treatment of recurrent complex aneurysms is challenging, with both surgical clipping and endovascular techniques. The limitations of surgical clipping include the lack of adequate residual aneurysm neck for direct clipping repair and that coils that protrude into the residual neck can cause the clip to slide onto the parent vessel, resulting in stenosis.12 Endovascular techniques applied to treat palindromic aneurysms can be divided into deconstructive and reconstructive techniques. Deconstructive strategies are a reasonable option only for the patients who tolerate BOT. However, the risk of tardus ischemia, aneurysm recurrence, or hemodynamics-related aneurysm growth at other sites still exists, even in those patients who tolerate the BOT.13 Common reconstructive techniques include coil or liquid embolization (Onyx; ev3, Irvine, Calif).6,14,15 These methods also include a risk of recurrence because of the difficulty of tight packing in giant, large, or dissecting aneurysms.
One of most promising advances is the use of covered stents to achieve reconstruction of the parent artery for the treatment of challenging aneurysms.16 In recent years, several authors reported the application of the covered stent in treatment of intracranial aneurysms.6,9,16–19 Covered stents have many potential advantages for intracranial applications. First, covered stents allow for the immediate occlusion of the aneurysm sac, while preserving the parent artery. Aneurysms treated with covered stents have greatly reduced recurrence rates, compared with coils or liquid embolics. Furthermore, this reconstructive strategy can avoid direct operations in the aneurysm cavity and reduce the risk of aneurysm rupture. Finally, in the management of very large and giant aneurysms, the mass effect after covered stent placement is less than that with coil or Onyx embolization. The currently used coronal covered stents, such as the Jostent (Abbott Vascular, Redwood City, Calif) or Symbiot (Boston Scientific) stent, have some problems and limitations, including that they are very stiff, lack longitudinal flexibility, are poorly navigated, and are difficult to adapt to the deep curves of the intracranial vasculature.6,17,18 For intracranial applications, the covered stent has to be miniaturized to fit through the more tortuous arteries and should also be highly flexible and maneuverable for smooth navigation.19,20
The Willis covered stent used in this study has been improved in terms of stent structure, membrane thickness, and the stent delivery system for intracranial applications.9,21 These improvements were intended to enhance the flexibility of the whole covered stent system and to facilitate passing it through the tortuous intracranial vasculature, especially in the siphon segment of the ICA. In our study, 100% of the Willis covered stents successfully arrived at the target area without any apparent resistance, including 5 aneurysms located in C7. Immediate angiography revealed that 2 aneurysms had small endoleaks between the stent and vessel walls. The primary cause of endoleaks may be that the covered membrane tensioned the stent, resulting in poor compliance and bad adherence. Other causes, including the inhomogeneous lumen of the blood vessel or a tear of the covering membrane, are also possible. If postdilation with a balloon is not effective, then other stent grafts may be used. Here, in 2 patients, we needed to use 2 or more covered stents, with the “end-to-end” technique. In such cases, a sufficient stents overlap (approximately 2–3 mm) must be made to prevent endoleak in the boundary area of the stents.
The closure of side branches or perforating arteries originating from the covered segment of the artery has always been a major concern in the use of covered stents for cerebral aneurysm treatment. Some reports suggest that the OA can be sacrificed if necessary, because reconstruction of the OA from the external carotid artery collaterals is possible.16 The AchoA is another important artery that primarily feeds the area of the optic tract, internal capsule, and cerebral peduncle. In our study, before stent deployment in the C7 segment, we carefully evaluated the angiogram from multiple angles to prevent covering the ostium of the AchoA. That the AchoA was patent was demonstrated by postprocedure angiography in all 5 of the patients after Willis covered stent placement in the C7 segment in this study and without neurologic event.
In the intracranial vasculature, restenosis is a hard problem for the application of covered stents. The process of intimal hyperplasia can occur as early as 2 weeks to 6 months after stent deployment.22,23 The midterm follow-up data in our series were very encouraging, and only 1 hemodynamic stenosis (<50%) was revealed by the 6-month angiographic follow-up, which may have been largely due to the irregular administration of antiplatelet drugs (case 4). Consequently, our patients usually underwent therapeutic inhibition of platelet function with 2 agents, typically, aspirin and clopidogrel, and heparinization should not be reversed at the end of the procedure.
Conclusion
In this small study with a middle-term angiographic and clinical follow-up, the Willis-covered stent was used safely and effectively to occlude aneurysms that had recurred after coiling. Longer-term follow-up and additional clinical experience are needed to fully determine the safety and efficacy of the device.
Footnotes
This study was supported by grants from the National Natural Science Foundation of China (grant 30570540), the Shanghai Important Subject Fund of Medicine (grants 05 III 023 and 074119505), and the Program for Shanghai Outstanding Medical Academic Leader (grant LJ 06016).
References
- Received December 7, 2007.
- Accepted after revision February 25, 2008.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- A single-center experience in the endovascular treatment of carotid siphon aneurysms using the Willis covered stent: a retrospective analysis
- Endovascular isolation of intracranial blood blister-like aneurysms with Willis covered stent
- Endovascular treatment of recurrent intracranial aneurysms with re-coiling or covered stents