
Abstract
BACKGROUND AND PURPOSE: The purpose of this study was to analyze the 3-month outcomes of patients with aneurysmal subarachnoid hemorrhage (SAH) treated from January 2005 to June 2006. This paper describes the outcomes after treatment of aneurysmal SAH and comparison between patients treated by clipping or coiling in a high volume center.
MATERIALS AND METHODS: A retrospective chart review was performed of records of 195 consecutive patients with SAH. The overall outcome and the pretreatment variables predicting outcomes and the difference between the clipping and coiling groups were analyzed by logistic regression analysis.
RESULTS: A total of 105 (55%) patients had microsurgical clipping and 87 (45%) had endovascular coiling. At 3 months, 69% of patients recovered with no or mild disability. The predictors of a 3-month modified Rankin Scale (mRS) were Hunt and Hess (HH) grade on admission and the presence of intracerebral hemorrhage (ICH). Patients in the coiling group had worse admission grades; they had worse 3-month mRS (2.28 vs 1.73), but this was not significant when the groups were matched (P = .38). Vasospasm rate was significantly higher in the clipping group (66% vs 52%). The immediate incomplete occlusion rate of aneurysms was higher (21.7% vs 7.6%) in the coiling group.
CONCLUSION: The overall results of treatment of aneurysmal SAH have improved. There is no significant difference in the outcomes between the patients in the clipping and coiling groups.
Subarachnoid hemorrhage (SAH) from ruptured aneurysms carries a poor prognosis; half the patients die within 1 month of the hemorrhage; of the patients who survive longer than 1 month, 40% remain dependent.1 Approximately 15% of patients with aneurysmal SAH die before reaching the hospital.2
Two prospective randomized studies of patients with ruptured aneurysms reported the differences in outcome between coiling and clipping. In the International Subarachnoid Aneurysm Trial (ISAT)3,4 (n = 2143), better outcome was noted with coiling. A second smaller study5 of 109 patients reported that the clinical outcome at 3 months was comparable between the surgical and endovascular groups. Three case series (1 retrospective6 and 2 prospective7,8 (1 with cognitive outcomes) found no difference in the overall clinical outcome between clipping and coiling. One retrospective case series9 noted better outcome in patients who underwent clipping compared with coiling.
The initial and definitive management of ruptured cerebral aneurysm is evolving, with clipping and coiling being alternative treatments. The outcomes of these treatment modalities are changing rapidly because of the improved quality of microsurgery and the development of new endovascular technologies as well as aggressive detection and management of vasospasm and other complications related to SAH itself.
Patients and Techniques
A retrospective chart review was performed of the records of 195 patients with ruptured intracranial aneurysms managed by the cerebrovascular service from January 2005 to June 2006.
Treatment Decisions and Protocols
The 3 principals (1 with extensive microsurgery experience, who was undergoing endovascular training; the second neurointerventional radiologist with extensive endovascular experience; and the third, a dually trained endovascular neurosurgeon) took turns to admit patients to the cerebrovascular service. The decision regarding clipping or coiling of the aneurysms was made independently by the physician whom the patient was admitted by on the basis of admission Hunt and Hess (HH) score, dome/neck ratio, aneurysmal location, and morphology. The other principals were consulted if necessary. The remainder of the patients’ preoperative and postoperative management was standardized.
All microsurgical and endovascular procedures were carried out by or under the direct supervision of the 3 principals. In patients who were treated with endovascular technique, coil embolization with 360 Guglielmi detachable bare platinum coils, with or without balloon assistance, was performed. Most patients treated by microsurgical aneurysmal clipping underwent skull base approaches in addition to hyperventilation, diuretics, and CSF drainage to minimize brain retraction, and the procedures were performed as soon as possible. Intraoperative and postoperative angiograms were performed to look for aneurysmal obliteration in all patients who underwent clipping or coiling.
All patients were admitted and were treated in the neurosurgical intensive care unit under the joint supervision of a neurosurgeon and a neurointensivist until there was resolution of neurologic (vasospasm, hydrocephalus, hyponatremia) and general medical (infections, deep venous thrombosis, airway, ventilation) issues. Prophylactic volume expansion therapy and nimodipine were given to all patients who could tolerate it without pulmonary edema.
Vasospasm was identified by daily clinical examination, daily transcranial Doppler (TCD) studies (Table 1), and single-photon emission CT (SPECT) scans every 2 to 3 days. Asymptomatic mild to moderate vasospasm by TCD was treated with hypertensive therapy. Endovascular angioplasty or nicardipine/papaverine injection was performed if the patient had any 2 of the following criteria: symptomatic vasospasm, severe vasospasm on TCD, or vasospasm by SPECT scan. The decision to discharge the patient from the general ward was made by the neurosurgeon in consultation with rehabilitation specialists and the nurses. Outpatient follow-up was done at 1 month, 3 months, and once yearly after discharge. A CT angiogram was done on all patients within 3 months after discharge.
Transcranial Doppler criteria for vasospasms after SAH
Follow-up intra-arterial digital subtraction angiograms were planned at 6 months and 1½ to 2 years in patients in whom coiling was performed and at 1½ to 2 years in patients in whom clipping was done. However, because of the length of the follow-up, approximately half the patients did not complete the studies.
Data Collection
Data collected included pretreatment variables of age, sex, and comorbidities (hypertension, smoking, high cholesterol level, diabetes, atherosclerotic disease, any other) of the patient, family history of aneurysms, admission grades (HH, World Federation of Neurosurgical Societies [WFNS], and Fisher), the presence of intracerebral hemorrhage (ICH), the location, size, and dome-to-neck ratio of the aneurysm. Management data included treatment technique (coiling or clipping) and complications related to treatment. Outcome measures involved moderate or severe vasospasm and its management, length of stay in the intensive care unit (ICU), hydrocephalus and brain infarcts, 3-month modified Rankin Scale (mRS), mortality, and discharge destination.
Analysis
We performed statistical analysis after dichotomizing the pretreatment variables with HH (I-II, good; III-V, bad), Fisher (I-II, good; III-IV, bad), and WFNS grades (I, good; II-V, bad).
Outcomes of all Patients
We analyzed the outcomes of ruptured aneurysms after classifying the outcomes by the mRS as no disability (mRS, 0–1), mild disability (mRS, 2), disabled for daily activities of living (mRS, 3–5), and dead (mRS, 6). The probability of pretreatment variables to predict 3-month mRS were analyzed by multivariate logistic regression analysis. We analyzed the outcomes after classifying them according to the main pretreatment predictors. The admission WFNS grades of our patients were compared with those of patients in the ISAT study.4 The outcome (3-month mRS) of our patients was compared with the outcome (1-year mRS) of patients as reported in the ISAT study.
Comparison of Patients in the Clipping and Coiling Groups
The clipping and coiling groups were compared with regard to the pretreatment variables and aneurysmal characteristics. The difference in the neck-to-dome ratios and the age of the patients was calculated by the Mann-Whitney Test.
The difference in vasospasm rates, interventions for vasospasm, ICU stay, discharge destination, mortality, and outcome (3-month mRS) between the clipping and coiling groups was analyzed by multivariate logistic regression analysis (linear regression for ICU stay). In addition, the immediate complication rates, incomplete occlusion rates, regrowth, rebleed, and retreatment rates of the clipping and coiling groups were compared.
Results
Patient Profile
A total of 195 patients (204 aneurysms) with aneurysmal SAH were admitted from January 2005 to June 2006. The average age of the patients was 53 ± 13 years, and the male-to-female ratio was 1:1.91. There were 105 (55%) patients who underwent clipping, and 87 (45%) who underwent coiling. Three patients died before they were selected for clipping or coiling. Four patients crossed over from the coiling to the clipping group because of technical difficulty with the procedure. Bypass was used in 11 patients as an adjunct to microsurgical clipping or trapping of the aneurysm. The indications for the performance of a bypass were inability to preserve the parent vessel or a major branch vessel during clipping and inability to successfully coil or clip the aneurysm without a bypass. The subgroups of the aneurysms are shown in Table 2 tabulated by their location and the technique of treatment.
Distribution of aneurysm groups and their location
Outcomes of All Patients
On the basis of the 3-month mRS, 69% of patients had no or mild disability and were not restricted for daily activities of living (Fig 1A). There were 31% of patients who were moderately or severely disabled or had died after treatment of SAH.

Pie chart showing the outcomes in the entire group of patients with SAH (DALY indicates daily activities of living).
Admission HH grades (P = .001) and ICH (P = .013) were significant independent predictors of the 3-month mRS by multivariate analysis. Comorbidity showed a trend toward predicting the mRS at 3 months (Table 3).
Statistical P values of pretreatment variables as predictors of three-month mRS outcomes considered simultaneously
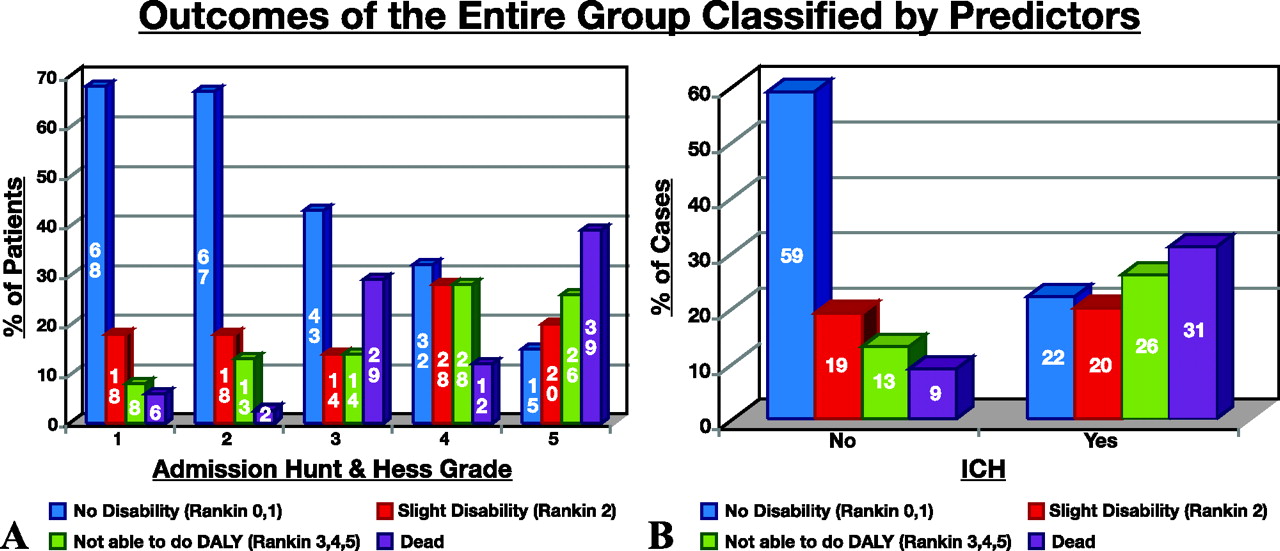
Of the patients who presented with ICH, at 3 months 44% had mRS of 0 to 2 and 56% were disabled (mRS, 3–5) or had died. Of patients who had no ICH, at 3 months 78% had no or mild disability (mRS, 0–2) and 22% were disabled (mRS, 3–5) or had died (Fig 2B).

Graph showing the outcomes and disabilities of patients according to their admission HH (A) and the presence or absence of ICH (B) in the entire group of patients with SAH.
When grouped according to admission HH grades, 85% of patients with grades I and II, 60% of patients with grades III and IV, and 35% of patients with grade V recovered to mRS of 0 to 2 at 3 months. (Fig 2A). Of patients with grade V who were older than 60 years (12/46; 26.1%), 1 recovered to mRS of 1, 4 were disabled (mRS, 3–5), and the remaining patients had died at 3 months. Of patients with grade 5 who were younger than age 60 years (34/46; 73.9%), 15 (44.1%) of 34 had no or mild disability (mRS 0 or 1 in 7 patients and mRS 2 in 8 patients), and 19 (55.9%) were disabled (mRS, 3–5; n = 8) or had died (n = 11) at 3 months.
Comparison with the ISAT Study.
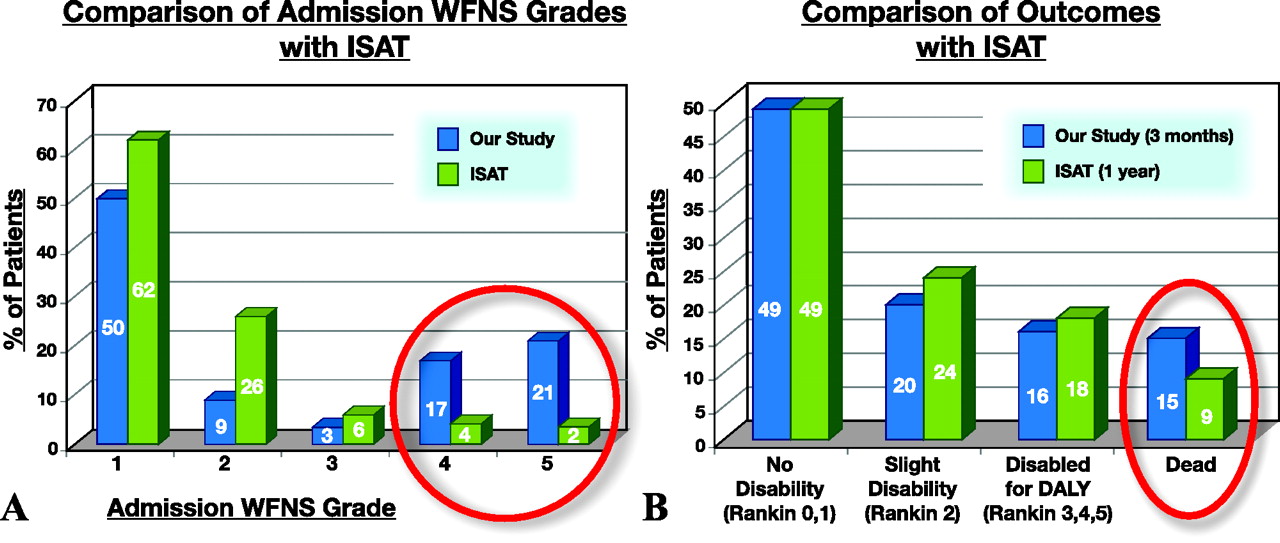
The patients in our study had worse WFNS grades than patients in the ISAT study (Fig 3A). There were 38% of patients in our study who were admitted with WFNS grades IV or V, whereas only 6% of patients in the ISAT study had admission WFNS grades IV of V. The outcomes (mRS) in our patients at 3 months were comparable with the 1-year outcomes (mRS) of patients in the ISAT study (Fig 3B).

A, Graph showing a comparison of the admission WFNS grades in our patients to that of patients in the ISAT study. B, Graph showing a comparison of the outcome in our patients (3 month mRS) to that of patients in the ISAT study (1 year mRS).
Comparison Between Clipping and Coiling Groups
The clipping and coiling groups were different in that the admission HH, WFNS, and Fisher grades were worse in the coiling group as shown in Table 4, and in the locations of the aneurysm (especially the middle cerebral artery, internal carotid artery, and pericallosal aneurysms) as shown in Table 2. The median dome-to-neck ratio was larger in the coiling group at 2.45 (confidence interval, 2.16–2.74) compared with the clipping group at 1.92 (confidence interval, 1.64–2.24), and this was significant (P= 0067; confidence interval, 0.14–0.80).
Pretreatment variables in patients with SAH
The incidence of TCD-diagnosed vasospasm (66% vs 52%) (P = .022) was significantly greater in the clipping than in the coiling group after controlling for the differences in the pretreatment variables (Table 5). There was a larger in-hospital mortality in the coiling group (16% vs 9%), but this was not significant (P = .220) after controlling for the differences in the pretreatment variables (Table 5). A significantly greater proportion of patients were sent to inpatient rehabilitation after the clipping procedure (35% vs 23%; P = 034). A significantly greater proportion of patients were sent home after the coiling procedure (49% vs 44%; P = .022).
Differences in vasospasm rates, ICU stays, discharge destination, and outcomes between clipping and coiling before and after controlling for pretreatment variables
Patients in the coiling group had a worse average mRS (2.28 ± 2.29 vs 1.73 ± 1.81) at 3 months compared with patients in the clipping group, but this was not significant (P = .613) after controlling for the differences in the pretreatment variables by multivariate analysis (Table 5). The mortality at 3 months was much higher in the coiling group (21% vs 9%), but this was not significant (P = .116) after controlling for the differences in the pretreatment variables. The cause of death in all of the patients was directly or indirectly related to SAH and its consequences and not related to clipping or coiling.
Immediate Treatment Failure and Rebleed
Four patients who were chosen for coiling could not undergo the procedure. Two patients had tortuous carotid vessels, which made access to the circle of Willis difficult. In the third patient, who was admitted with HH grade V SAH and a P1 segment aneurysm, the aneurysm could not be selectively accessed for coiling, and this patient died before any further treatment could be done. A fourth patient with a vertebrobasilar aneurysm, who was admitted with a grade I HH SAH, had coil migration into the middle cerebral artery through the posterior communicating artery during coiling and intraprocedural rupture of the aneurysm; this patient subsequently died. The immediate incomplete occlusion rate after coiling was 18 (22.2%) of 81. Of these, 14 patients had only neck remnants (Raymond class II), and 4 patients had neck and sac remnants (Raymond class III). The immediate incomplete occlusion rate after clipping was 7 (7.6%) of 104, all of whom had only neck remnants (Raymond class II).
One (1%) patient in the clipping group who had an apparently complete occlusion of an anterior communicating artery aneurysm on postoperative angiography had a rebleed from aneurysmal regrowth from a posterior neck remnant 1 month later, and the aneurysm was obliterated completely by clipping with an A3-A3 bypass. There were no rebleeds in the coiling group.
Follow-Up Angiograms and Retreatment
Eighteen patients in the coiling group had died at 3 months. Of the remaining 65 patients, 42 (64.6%) had a follow-up angiogram approximately 6 months after the procedure. Of these, 12 patients were found to have had a recanalization of their aneurysms (total occlusion to neck remnant in 11 [Raymond I to II] and coil compaction in a patient who had a neck and dome remnant [worsening of Raymond III]). Of these 12 patients, 6 were treated again, 5 by clipping and 1 by stent-assisted coiling. The patients in whom clipping was performed had no remnants postoperatively; the patient in whom coiling was performed still had a neck remnant.
Nine patients in the clipping group had died at 3 months. Of the remaining 99 patients, 12 (12.1%) had follow-up angiograms approximately 18 months after the procedure. One patient had a rebleed and has been discussed above. The remaining 11 patients did not have a recurrence of the aneurysms.
Procedural Complications
In 1 patient admitted with a P1 segment aneurysm, the aneurysm could not be selectively accessed for coiling, and this patient died before further treatment could be done. Another patient with a vertebrobasilar aneurysm had coil migration into the middle cerebral artery through the posterior communicating artery during coiling and intraprocedural rupture of the aneurysm; this patient subsequently died. One (1.2%) patient in the coiling group had coil perforation (basilar apex aneurysm), which was managed successfully by the inflation of the balloon and the placement of additional coils. Four (4.6%) patients in the coiling group had groin complications.
Two patients in the clipping group (both had anterior communicating artery aneurysms) had minor intraoperative aneurysmal ruptures, which were managed uneventfully by standard surgical techniques. One patient with an anterior communicating artery aneurysm had a rebleed, which was managed by reclipping, and an A4 to A4 bypass (due to occlusion of one A2 vessel). Five (4.8%) patients in the clipping group had postoperative superficial wound infections.
One patient with HH grade V with an anterior communicating artery aneurysm had a rupture of the A1 segment during balloon angioplasty. The catheter was immediately withdrawn, the balloon was inflated on the ipsilateral carotid artery, and the A1 segment was occluded by coils. CT scan after angioplasty showed massive increase in SAH, and the patient died in the hospital. There were no other complications after angioplasty in this series.
Hydrocephalus and Cerebral Infarction
The incidence of shunt-dependent hydrocephalus was 14 (13.3%) versus 13 (14.9%) in patients treated with clipping and coiling, respectively. All patients had follow-up CT scans of the head after their treatment. Seventeen (19.5%) patients in the coiling group and 12 (11.4%) in the clipping group had cerebral infarctions in the vascular territory of the parent vessel of the aneurysm treated on the follow-up CT scans. All of these patients had vasospasm (TCD diagnosed) in the same vascular territories after treatment, and there was no immediate temporal relationship between clipping and coiling and the development of infarction in any of these patients. Of the patients who had cerebral infarctions in the vascular territory of the parent vessel, 1 in the coiling group had a decline in neurologic condition 3 days after coiling, and 2 in the clipping group had neurologic decline 2 days after clipping. All 3 of these patients had vasospasm in the territory of the parent vessel. There was no change in neurologic condition in the other patients with evidence of cerebral infarction on CT.
Discussion
Statistical Analysis
Logistic regression analysis was chosen in an attempt to adequately compare the outcomes despite pretreatment differences in the patients treated by each method. We dichotomized the admission HH, Fisher, and WFNS scores because the levels, though ordered, are not designed to be an equal distance apart. As shown in Table 4, there are substantial pretreatment differences between the groups receiving alternate treatments, some of them in variables related to outcome. These pretreatment differences can confound comparisons (ie, the unadjusted outcome might be reflecting the pretreatment differences), in addition to the effect of treatment. Logistic regression was used to attempt to statistically control for these differences. Although the methods adjust for the pretreatment differences included, they cannot adjust for variables that were not measured and might incompletely adjust if the true relationships among variables are more complex than those included in the model used. These are, however, methods that are commonly used in trying to evaluate treatment effects from nonrandomized studies.6
Outcomes of All of the Aneurysms
In 1993, Longstreth et al,10 conducted a population-based study on the outcomes of SAH in King County, Washington. In that study, 68% survived to 1 month after the bleed and 62% to 1 year. At 1 month after the bleed, approximately one third of patients had died, one third had neurologic deficits, and one third were doing well (mRS, 0–2). In our series, only 31% of patients in the group of all ruptured aneurysms had died or had become disabled (mRS, 3–6) at 3 months, compared with previous reports wherein 70% of patients had either become disabled or had died.1,10–14 Even after accounting for 15% of patients who die before reaching the hospital,2 this outcome is better than all previous reported series.
Outcomes of the Entire Group by Admission Grades
In 1999, Le Roux et al14 from our institution reported that 86% of patients with HH grades I to III return to independent function at 3 months (mRS, 2 or better). Of the patients who were grade IV/V at admission, 38% (54% of those with grade IV and 24% of those with grade V) recovered to good condition at 6 month follow-up (mRS, 0–2). In this series, at 3 months 85% of patients with HH grade I and II, 60% of patients with HH grade III, 57% of patients with HH grade IV, and 35% of patients with HH grade V recovered to mRS of 0 to 2. Thus, the outcome of patients with aneurysmal SAH has considerably improved in the last decade. This may be because of improved expertise in microsurgery, treatment of appropriate patients with coiling, and the aggressive treatment of vasospasms.
Patients with a HH grade IV SAH had outcomes equivalent to patients with HH grade III SAH. Patients with a HH grade V SAH who are older than 60 years had a dismal outcome at 3 months (91.7% having died or become disabled). In patients with a HH grade V SAH who are younger than 60 years, 44.1% recovered to mRS of 0 to 2. In future analyses of outcomes of studies in patients with poor grades, all HH grades should be done separately, rather than by combining groups. In particular, patients with HH grade V patients should be analyzed separately from those with HH grade IV.
Outcomes of the Clipping and Coiling Groups
At discharge, a significantly greater proportion of patients were sent to inpatient rehabilitation after the clipping procedure and home after the coiling procedure. However, there was no significant difference in the mortality and outcomes (mRS) at 3 months between the clipping and coiling groups by multivariate analysis. The higher mortality and worse outcome in the coiling group is the result of the difference in the pretreatment variables (admission grades). These need to be studied with longer follow-up, with more refined outcome measures including cognitive outcomes.
Occlusion and Rebleed Rates
Our incomplete occlusion rates in the clipping (7.6%) and coiling (21.7%) groups were better than those reported for clipping (17.8%, ISAT; 0.0%–26.3%, other studies) and coiling (33.7%, ISAT; 8.3%–70.4%, other studies).15 Our rebleeding rates in the clipping (1%) and coiling (0%) groups are comparable with those reported for clipping (1.21%, ISAT; 0.0%–2.27%, other studies) and coiling (3.26%, ISAT; 0%–5.33%, other studies).15
Vasospasm
Cerebral vasospasm is a major cause of death and disability.7 Several reports6,16–18 describe a lower incidence of cerebral vasospasm in patients treated with coiling compared with clipping of ruptured intracranial aneurysms. One similar study found that the risk for vasospasm was lower with clipping than with coiling.19 In our study, the incidence of TCD-diagnosed vasospasm was significantly lower in the patients who underwent the coiling procedure. The degree of vasospasm may be related to the amount of blood in the subarachnoid space, clearance of blood by surgery (positive impact), and manipulation of vessels during surgery (negative impact). The difference in vasospasm requires further study.
Treatment Protocol
On the basis of our study and experience, we have developed a treatment protocol (not used for patients in this study) that needs further refinement and validation. Certain aneurysms can be managed more safely by clipping: aneurysms of 20 mm or more and less than 2 mm, blister aneurysms, fusiform aneurysms in a vessel that does not have collaterals, 2 or more critical branches incorporated in the aneurysmal neck, and critical branches from the sac or fundus of the aneurysm. A vascular bypass followed by clipping or trapping of the aneurysm may be necessary, when clip reconstruction is not possible in these cases. We restrict the use of stent-assisted coiling in ruptured aneurysms to endovascular emergencies that necessitate placement of a stent during an endovascular procedure. In such a patient, a glycoprotein IIb/IIIa inhibitor has to be administered intravenously, supplemented by oral aspirin and clopidogrel. This may complicate postoperative management.
Limitations and Applicability of this Study
This is a retrospective study conducted on a small number of patients. This may have resulted in multiple biases, particularly with respect to clipping or coiling. The data were collected by chart reviews and not by contacting the patients. The patients were retrospectively matched for their pretreatment variables and were not randomized. The outcomes were measured with 3-month mRS, and cognitive outcomes were not measured. The results of this study can be applied only to centers with a similar expertise in management of these patients and where aggressive management of vasospasm is pursued.
Comparison with ISAT Study
The outcomes at 3 months in our group were comparable with the 1-year outcomes of patients in the ISAT study, despite the fact that the admission grades in our patients were worse. The mortality in our patients was higher than that of the patients in the ISAT study, which may be explained by the fact that there were 38% of patients in our study with admission WFNS grades IV and V, whereas there were only 6% of patients with WFNS grades IV and V in the ISAT study.
There was much controversy and discussion in the worldwide neurosurgical community about the results of the ISAT.20,21 Of the 9559 patients eligible for inclusion, only 2143 (22%) were included in the study. There was no standard protocol for the postoperative management of patients after treatment. Because of these factors, the results of ISAT cannot be generalized to all aneurysms. ISAT is still the best data available and cannot be challenged by our study. In our study, we analyzed all aneurysms managed in our institution. The postoperative management was aggressive and standardized. The results of treatment of aneurysms in our center may be more generally applicable, though this warrants further study in other institutions.
Future Studies
We believe that there is a need for a prospective registry-type study of all patients treated for ruptured aneurysms, with careful analysis of patient outcomes including return to work, adaptation to daily life, caregiver burden, neuropsychologic outcome, angiographic outcome, and the costs of treatment. Such a study could be conducted at a consortium of high-volume aneurysm treatment centers. An ongoing study such as this would take into account any “new developments” in technology or other modalities of treatment. The results of such a study may help us to better select the patients for both endovascular and microsurgical treatment. It is highly improbable that another randomized trial similar to ISAT will be funded or conducted.
Conclusion
The results of treatment of aneurysmal SAH have improved compared with previous reports; 69% of patients recovered to mRS of 0 to 2 at 3 months. More than one third of patients with poorer grades recovered with minimal or no disability at 3 months. Patients with HH grade IV SAH had outcomes equivalent to patients with HH grade III SAH. Patients aged older than 60 years with admission HH grade V SAH had poor outcomes with either technique.
The immediate incomplete occlusion rate (21.7% vs 7.6%) was higher in the coiling group. The immediate occlusion, recanalization and rebleed rates, need for retreatment, and protocol for selection of technique for retreatment have to be studied and taken into consideration for selecting patients for clipping or coiling.
References
- Received July 3, 2007.
- Accepted after revision October 3, 2007.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Clinical outcome after surgical clipping or endovascular coiling for cerebral aneurysms: a pragmatic meta-analysis of randomized and non-randomized trials with short- and long-term follow-up
- Endovascular Management of Distal ACA Aneurysms: Single-Institution Clinical Experience in 22 Consecutive Patients and Literature Review
- Clipping Versus Coiling for Ruptured Intracranial Aneurysms: A Systematic Review and Meta-Analysis
- Clinical predictors of delayed cerebral ischemia after subarachnoid hemorrhage: first experience with coil embolization in the management of ruptured cerebral aneurysms
- Endovascular Treatment or Neurosurgical Clipping of Ruptured Intracranial Aneurysms: Effect on Angiographic Vasospasm, Delayed Ischemic Neurological Deficit, Cerebral Infarction, and Clinical Outcome
- Does treatment modality affect vasospasm distribution in aneurysmal subarachnoid hemorrhage: differential use of intra-arterial interventions for cerebral vasospasm in surgical clipping and endovascular coiling populations
- Coiling of Intracranial Aneurysms: A Systematic Review on Initial Occlusion and Reopening and Retreatment Rates