
Abstract
SUMMARY: Oncocytic neoplasms result from metabolically altered cells that accumulate abundant mitochondria within their cytoplasm by oncocytic metaplasia. In this report, the CT findings are described and correlated with the histopathologic features of a case of oncocytoma involving the parotid gland that arose in a background of nodular oncocytic hyperplasia. When imaging demonstrates multiple small nodules in the parotid gland with a large, solid, or cystic mass, the diagnosis of oncocytic neoplasia should be considered.
Oncocytic neoplasms result from metabolically altered cells that accumulate abundant mitochondria within their cytoplasm to form oncocytes by the process of oncocytic metaplasia. These neoplasms are found rarely in the parotid gland and account for <1% of salivary gland tumors. However, the finding of oncocytic metaplasia is extremely common and occurs in a multitude of organs, including the thyroid gland, parathyroid glands, and kidneys, in addition to salivary glands.
In the parotid gland, oncocytic metaplasia arises along a spectrum of related conditions, including oncocytic hyperplasia, benign oncocytoma, and, rarely, oncocytic carcinoma. Oncocytic hyperplasia may be found in microscopic foci or multiple macroscopic nodules, known as nodular oncocytic hyperplasia. Oncocytoma is a benign tumor comprising bland oncocytes, usually presenting as a single nodule.
To our knowledge, the imaging findings of oncocytic metaplasia of the salivary gland have only limited description in the literature. We present the CT and histopathologic findings of a case of oncocytoma arising in a background of oncocytic hyperplasia of the parotid gland.
Case Report
A 61-year-old white man presented with a 3-year history of painless right parotid gland fullness. One week prior, he developed sudden constant dull aching pain radiating from the right parotid region. Physical examination revealed diffuse enlargement of the parotid gland with a soft nontender right retromandibular mass. Intraoral examination revealed bulging of the right oropharynx. No facial nerve dysfunction or cervical lymphadenopathy was found.
CT revealed enlargement of the superficial lobe and loss of normal architecture of the right parotid gland. Multiple solid masses, most <1 cm in diameter, were seen within the gland. A retromandibular mass demonstrated cystic necrosis with a rim of peripheral enhancement (Fig 1A). The largest mass, in the tail of the parotid gland, measured 1.6 cm and was suggestive of a metastatic lymph node (Fig 1B). A more focal well-defined mildly enhancing tumor was also seen within the deep lobe of the parotid gland, measuring 4.2 cm transversely and 2.6 cm anteroposteriorly (Fig 1A, black arrow). The tumor extended from just below the skull base to the angle of the mandible.

Contrast-enhanced CT scans of the neck at the C1 and C2 levels (A) and below the angle of the right mandible (B). A, Complex masses involving the deep and superficial lobes of the right parotid gland are seen. The tumor involving the deep lobe of the parotid gland demonstrates an inhomogeneous mild degree of enhancement (large arrow). The medial margin of the tumor is well defined and compresses the adjacent parapharyngeal space (arrowheads). The superolateral aspect of the tumor blends with the adjacent lateral pterygoid muscle. The superficial lobe of the right parotid gland demonstrates 2 small masses: a solid one with mild enhancement (small arrow) and the other with cystic necrosis and peripheral enhancement (small open arrow). The parotid tissue at the junction of the superficial and deep lobes also demonstrates an ill-defined mass with feeble enhancement (large open arrow). B, Multiple small masses involving the right parotid tail (small arrows) are apparent, including a mass (large arrow) that measured 1.6 cm just below this level.
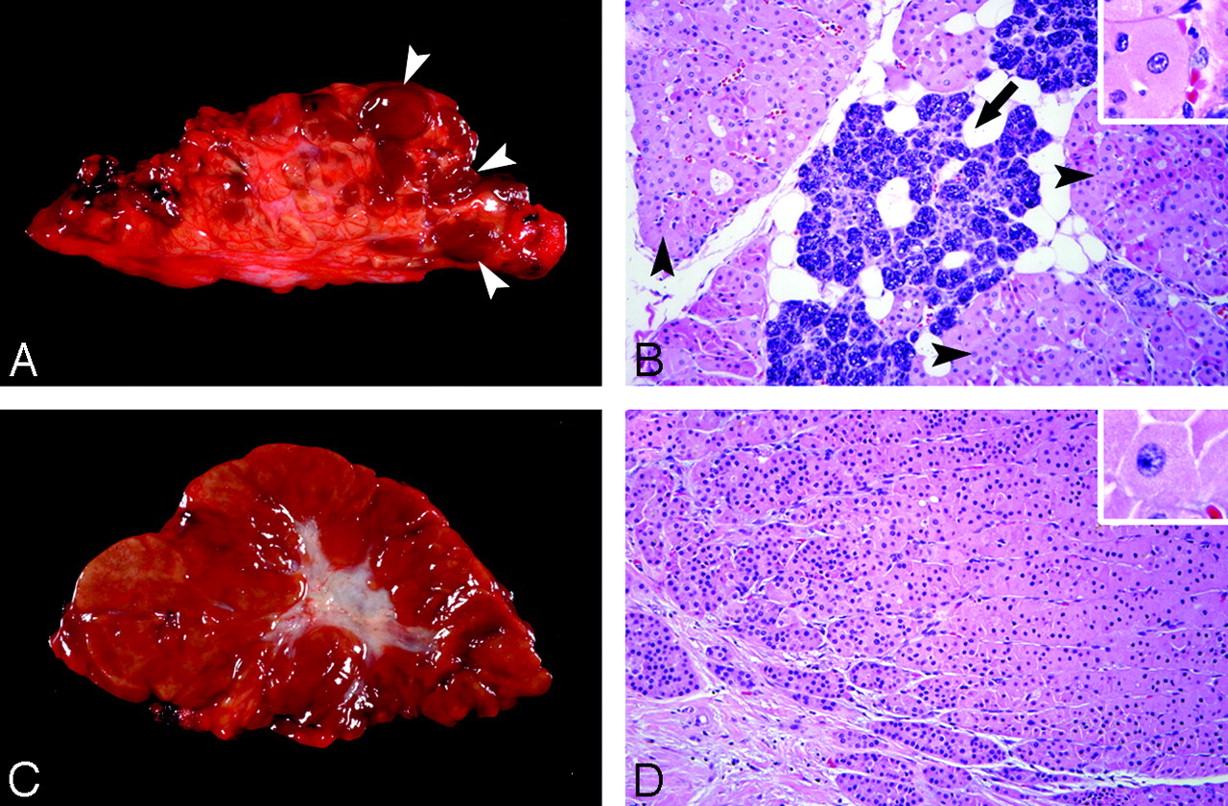
Total parotidectomy was performed by a combined transparotid-submandibular approach, sparing the facial nerve. Multiple enlarged well-circumscribed ovoid masses were found in the periparotid region and parotid tail and appeared as lymph nodes. Frozen-section assessment demonstrated oncocytes without lymph node architecture. The superficial lobe of the parotid gland contained numerous well-circumscribed masses protruding from its surface and multiple homogeneous 0.5- to 1.0-cm nodules throughout the gland parenchyma (Fig 2A). One of the nodules showed central necrosis, corresponding to the imaging findings. The deep lobe of the parotid gland was removed intact by pericapsular dissection from the parapharyngeal space. The resected specimen was a firm light-brown mass with well-circumscribed slightly irregular borders and revealed a prominent central gray scar on cut section (Fig 2C).

A, Superficial parotidectomy specimen (8.0 × 6.0 × 5.0 cm) with multiple mahogany nodules studding the parenchyma, corresponding to oncocytic hyperplasia (arrowheads). B, Corresponding hematoxylin-eosin (HE)-stained paraffin-embedded section from the specimen described in A shows islands of oncocytes (arrowheads) with interspersed normal acini, fat, and ducts (arrow). Insert shows a high-power view of a polygonal oncocyte (100×, insert 400×). C, Parapharyngeal space (deep lobe of the parotid gland) mass with a central scar oncocytoma (5 × 4.0 × 3.0 cm). D, Corresponding HE-stained paraffin-embedded section from the specimen described in C shows solid sheets of oncocytes. Inset shows a high-power view of a bland oncocyte with ample granular cytoplasm and defined nucleoli (40×, insert 400×).
Microscopic examination of hematoxylin-eosin–stained formalin-fixed paraffin-embedded sections revealed extensive nodular oncocytic hyperplasia involving the entire superficial lobe of the parotid gland. Islands of oncocytes forming macroscopic nodules were present, with intervening ducts, acini, and fat in a background of morphologically normal serous acini (Fig 2B). In contrast to the superficial lobe mass, in which intervening normal structures were admixed with oncocytes, the deep lobe parapharyngeal mass contained a solid sheet of oncocytes with a central fibrous scar, consistent with an oncocytoma. No intervening normal parenchyma was identified within the mass (Fig 2D). At a higher magnification, both the superficial- and deep-lobe oncocytes were found to have increased eosinophilic cytoplasm, with granular composition, polyhedral outlines, and prominent nucleoli. The oncocytes in both the hyperplastic and oncocytoma areas were bland, with no atypia or mitoses. Focal central necrosis of one of the hyperplastic nodules was noted, but the nodules were otherwise unremarkable. The enlarged parotid tail nodule, thought to be a metastasis-containing lymph node on imaging, showed an oncocytic hyperplastic nodule on histologic examination. Examination of 7 intraparotid nodes revealed oncocytes with no lymphoid tissue.
At 4-month follow-up, the patient reported no symptoms related to the right parotid gland but had noted a left parotid mass. On physical examination, the right preauricular and neck incisions were well healed, and we found no evidence of recurrence. However, a 2-cm freely movable mass was palpable in the tail of the left parotid gland. A left superficial parotidectomy was performed, and pathologic analysis revealed salivary gland nodular oncocytosis.
Discussion
To our knowledge, few reports on the imaging of oncocytic neoplasms of the salivary glands have been published, owing to the rarity of the condition. Sakai et al1 reported an oncocytoma in the deep lobe of the parotid gland that was well-defined and solid on CT. It demonstrated decreased signal intensity on both T1- and T2-weighted MR images, attributed to the high cellularity and low free water content. According to the authors, Warthin tumor, which is a common benign parotid gland tumor in patients older than 60 years, can be differentiated from oncocytoma by its MR imaging appearance. Warthin tumors conversely demonstrate decreased signal intensity on T1-weighted images and increased signal intensity on T2-weighted images.1 Both Warthin tumors and oncocytomas show intense uptake of the nuclide on technetium-Tc99m pertechnetate radionuclide scans of the salivary glands.2
The histomorphologic findings of oncocytes include an enlarged polygonal shape with granular intensely acidophilic cytoplasm, a round uniform nucleus with distinct nucleoli, and a low nucleus-cytoplasm ratio. These cytomorphologic features are associated with marked mitochondrial hyperplasia, pleomorphism, and a paucity of other organelles, as reported by Johns et al3 in ultrastructural studies. Mitochondrial dysfunction and defective cellular metabolism have been proposed as the basis for the characteristic findings of oncocytic mitochondrial hyperplasia and pleomorphism.4 Hamperl5 suggested that oncocytic metaplasia represents a final common pathway of cellular differentiation due to functional enzyme exhaustion or ≥1 mitochondrial enzyme.
Despite the nearly universal finding of oncocytic metaplasia in the salivary glands of patients 70 years of age or older, oncocytic neoplasms are rare in the salivary glands.6 The World Health Organization defines 3 categories of oncocytic neoplasms of the salivary gland. Oncocytoma, the most frequent form, is as a well-circumscribed benign tumor composed of monotonous sheets of oncocytes, frequently with a central scar. Nodular oncocytic hyperplasia (or oncocytosis), which was first described by Schwartz and Feldman,7 is a multifocal process, with diffuse replacement of the parotid gland with oncocytic lobules and intervening small foci of residual normal serous glands and ducts. Oncocytic carcinoma is the rarest of the oncocytic neoplasms, with only 36 cases reported in the English-language literature through 1999.
At 61 years of age, the patient in our report had both oncocytic hyperplasia and an oncocytoma in the same parotid gland. Moreover, oncocytic hyperplasia involved the surface and tail of the parotid gland and led to a pedunculated nodule that presented as a neck mass. The synchronous multiple morphologic variants of oncocytic neoplasms in a single parotid specimen have been reported by Capone et al.8 Their findings and ours support the theory that a common mitochondrial defect allows progression between the morphologic variants. Although that theory of parotid oncocytopathy is attractive, no molecular data have yet supported a link between the morphologic variants of oncocytic neoplasms.
Our case supports the recommendation that when multiple small nodules are found in the parotid gland with a large solid or cystic mass evident on CT or MR imaging, a diagnosis of nodular oncocytic hyperplasia and oncocytoma should be considered, particularly in patients 60 years of age or older. After parotidectomy for oncocytic hyperplasia, patients should be followed for recurrence arising from residual parotid tissue. If nodules are found on subsequent clinical examination or imaging, fine-needle aspiration biopsy can confirm oncocytic metaplasia by the presence of the bland oncocytes.
Footnotes
This work was supported in part by the National Institutes of Health grants DE13594 and T32 CA60374, MD Anderson Cancer Center Specialized Programs of Research Excellence (SPORE) in Head and Neck grant CA97007, Cancer Center Support grant CA16672, the Alando J. Ballantyne Distinguished Chair in Head and Neck Surgery Award, the Michael A. O'Bannon Endowment for Cancer Research, an American Academy of Otolaryngology-Head and Neck Surgery Foundation Percy Memorial Grant (G.L.C.), and an American Society of Clinical Oncology Young Investigator Award (T.D.S.).
- Received October 17, 2007.
- Accepted after revision November 12, 2007.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}