
Article Figures & Data
Figures
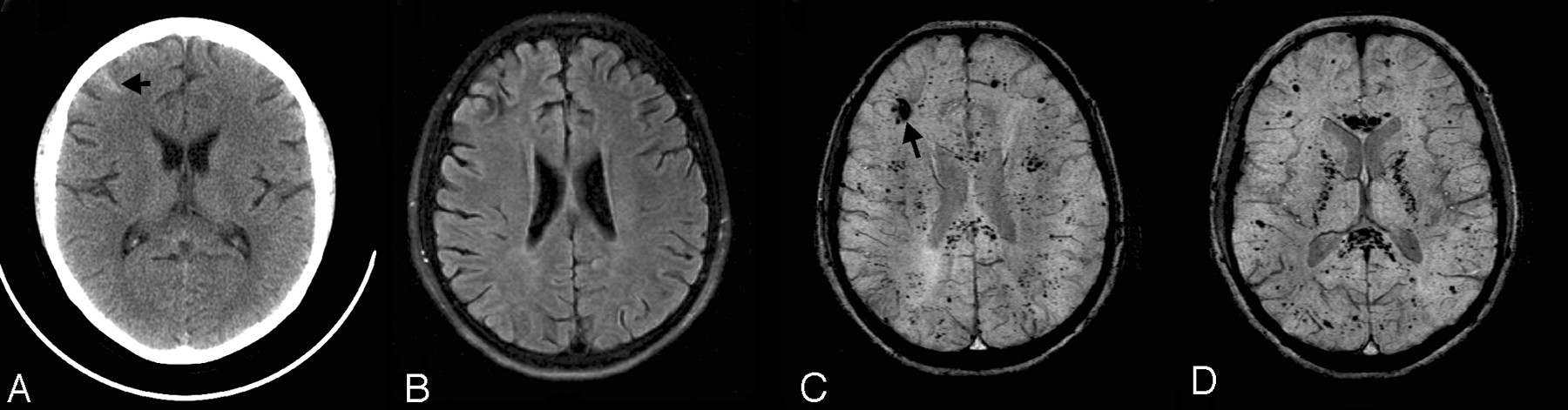
- Fig 1.
Diffuse axonal injury. This 17-year-old boy had a severe TBI in a motorcycle crash and had an initial GCS score of 5. Intracranial pressure was normal. Axial T2 and SWI images at the level of the centrum semiovale (A and B) and at the level of the lateral ventricles (C and D) are depicted. Small hemorrhagic shearing injuries in the left frontal subcortical white matter (arrows) are more are visible on SWI (B). At the lower level, SWI (D) shows additional small hemorrhagic shearing foci (open arrows) in the left frontal white matter, right subinsular region, and left splenium that are only partly visible on T2-weighted images. He was discharged 16 days after admission with moderately impaired cognition. Two years after injury, he continues to have fine-motor deficits. He has significant impairments on measures of verbal functioning (verbal comprehension, learning, and memory).
- Fig 2.
Leukemic hemorrhage. This 6-month-old boy presented with fever, leukocytosis thrombocytopenia, anemia, and hepatosplenomegaly. Axial FLAIR (A), T2-weighted (B), and SWI (C) images show a large hematoma in the left frontal lobe (asterisks). A few small hemorrhages with surrounding edema were also visible in the right subcortical white matter (open arrows) on the FLAIR and T2-weighted images. There is also a small right convexity subdural collection with hemorrhage (arrows). However, numerous additional hemorrhagic foci throughout the bilateral hemispheric white matter are only visible on SWI. He was subsequently diagnosed with acute lymphocytic leukemia. The multiple intracranial hemorrhages were thought to be associated with seizures that were difficult to control, with profound cognitive and motor impairments, and hydrocephalus that required ventriculoperitoneal shunting. Several years later, he remains profoundly impaired.
- Fig 3.
Vasculitis. This 16-year-old girl with systemic lupus erythematosus, chronic pancreatitis, nephritis, hypertension, cerebritis, and epilepsy presented with a 2-day history of chest pain and headache and a seizure on the day of admission. She was hypertensive and treated with methylprednisolone (Solu-Medrol) and cyclophosphamide (Cytoxan). Her complete blood count and chemistry profiles were normal, and she had no evidence of acute infection. Axial CT (A), FLAIR (B), and SWI (C and D) images are shown. A small hemorrhage is present in the right frontal lobe (arrows) on CT (A) and SWI (C). However, only the SWI images demonstrate numerous additional tiny hypointense foci suggestive of petechial hemorrhages or possibly microthrombi throughout the white matter, particularly within the corpus callosum and internal capsules. She was placed on a higher dose steroid regimen and discharged 1 week after admission. Although the etiology of the lesions was undetermined, vasculitis or Cytoxan therapy were considered as possibilities.
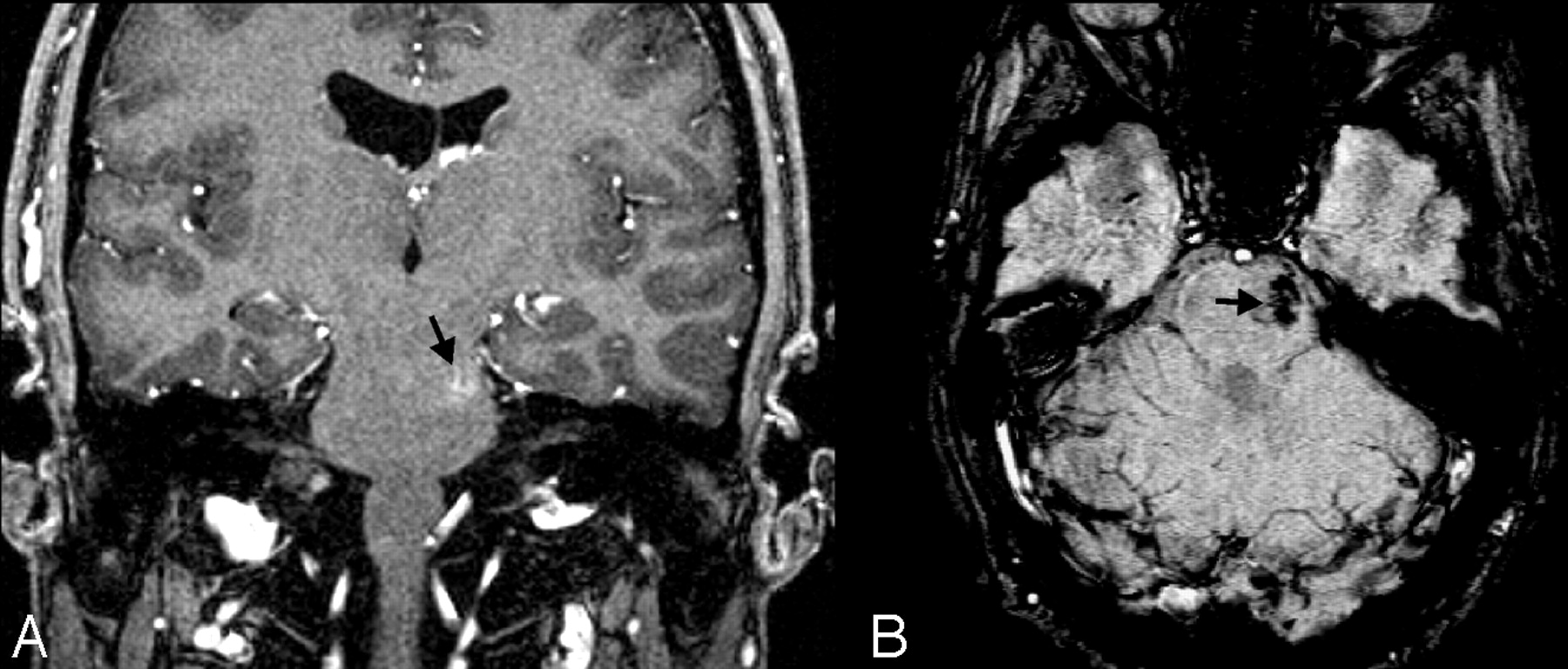
- Fig 4.
Cavernoma/telangiectasia. This 24-year-old student was being evaluated for partial complex seizures, and an MR image revealed a left temporal lobe lesion (not shown) that was thought to be a low-grade glioma, as well as an incidental lesion in the left pons. Contrast-enhanced coronal GRE T1-weighted image (A) depicts a small mildly enhancing lesion in the left pons (arrow). The lesion was not visible on T2-weighted images (not shown) but appears on axial SWI (B) as a markedly hypointense area. The ill-defined blush is commonly seen in low-flow vascular malformations, and the marked hypointensity of the lesion on the SWI sequence suggests that this represents an occult vascular malformation. Although there was no pathologic confirmation, given the location and size, it likely represents a cavernoma that had not bled.
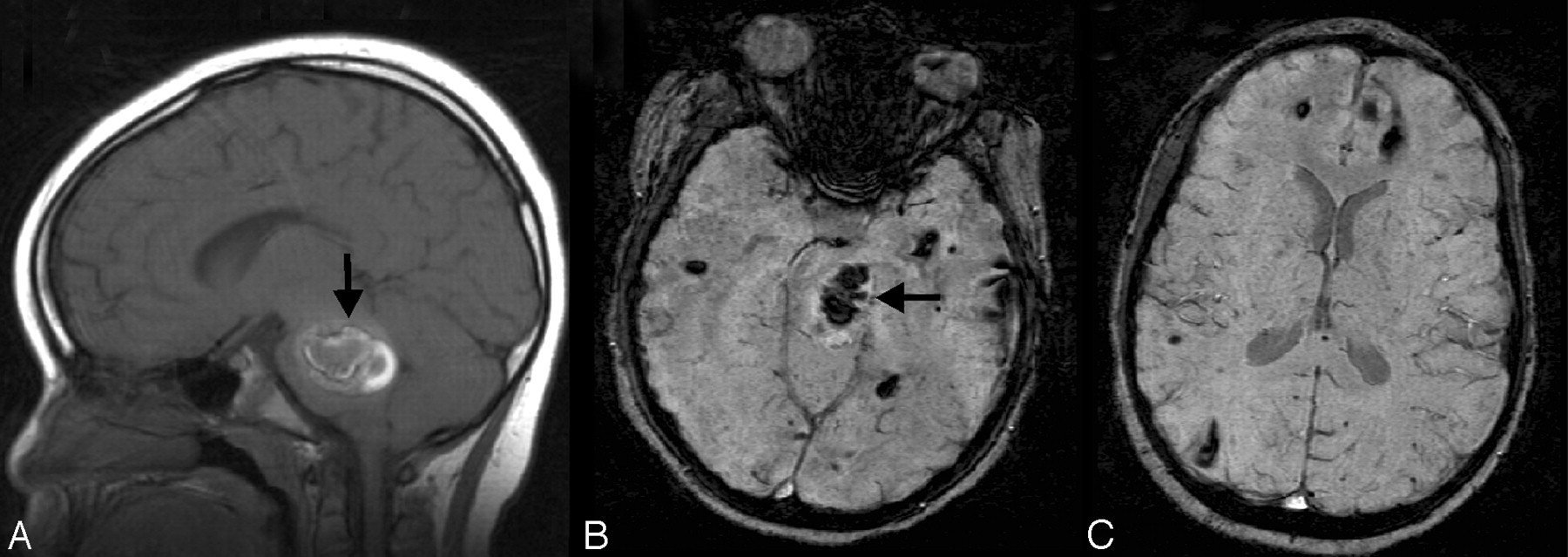
- Fig 5.
Multiple cavernous angiomas. This 7-year-old boy was admitted for evaluation of ataxia, dizziness, blurred vision, and alternating facial droop. MR imaging shows a large pontine hemorrhage (arrow) the on sagittal T1-weighted image (A) and axial SWI (B). Axial SWI at a higher level (C) shows numerous additional scattered small hypointense lesions, consistent with multiple cavernomas. The pontine hemorrhage and cavernoma were subsequently surgically resected. He has been clinically stable.
- Fig 6.
Radiation telangiectasias. This 11-year-old boy was diagnosed with medulloblastoma and had undergone surgical resection, radiation, and chemotherapy. He presented 8 years later with intermittent pulsating parieto-occipital headaches and complete loss of hearing in the left ear. Multiple serial MR imaging studies during the course of several years (not shown) showed a few scattered small faintly hypointense foci in the white matter but no other significant abnormalities. On his most recent MR imaging study, an axial T2-weighted image (A) again shows a few small hypointense foci in the white matter (arrows), similar to those in prior studies. However, axial SWI (B) shows numerous hypointense foci throughout the white matter, suggestive of radiation-induced telangiectasias.
- Fig 7.
SWS. This 7-year-old boy was originally seen at 18 days of life and diagnosed with SWS on the basis of findings of bilateral port-wine stains involving the face, trunk, back, and thigh without evidence of hemihypertrophy. Findings of his electroencephalography were normal as were the findings of his neurologic examination. A CT scan in the neonatal period (not available) suggested prominent veins in the right meninges near the Sylvian fissure. His first MR imaging scan at 7 months (not shown) demonstrated intense contrast enhancement of the vascular structures of the right parietal and occipital regions. Follow-up MR imaging at age 5 years is shown. A mildly enlarged deep subependymal vein along the right lateral ventricle is visible (arrows) on a T2-weighted image (A), contrast-enhanced T1-weighted image (B), and SWI (C). The postcontrast T1-weighted image (B) also reveals additional prominently enhancing right subcortical and deep medullary veins (open arrows). However, SWI (C) best delineates these prominent veins related to abnormal venous drainage in this condition and also shows a subtly prominent left subependymal vein (arrowhead), indicating early contralateral involvement. He has been developing normally, and his facial lesions have been treated with cosmetic laser surgery. He has had no evidence of seizures or other neurologic symptoms but is being treated for glaucoma.
- Fig 8.
Cortical vein thrombosis. This 16-year-old boy with acute lymphoblastic leukemia presented with emesis, headache, and impaired speech. On the postcontrast coronal T1-GRE image (A), there is a large irregular acute hemorrhage in the left parietal lobe with surrounding edema and adjacent sulcal effacement. Tubular filling defects are also visible on either side of the superior sagittal sinus (white arrows), consistent with thrombosed cortical veins. An axial FLAIR image (B) shows symmetric bilateral edema, adjacent to large hypointense cortical veins (black arrows) on SWI (C). In this case, the enlarged cortical veins were due to thrombosis, which was thought to be secondary to coagulopathy associated with PEG-asparaginase administration.
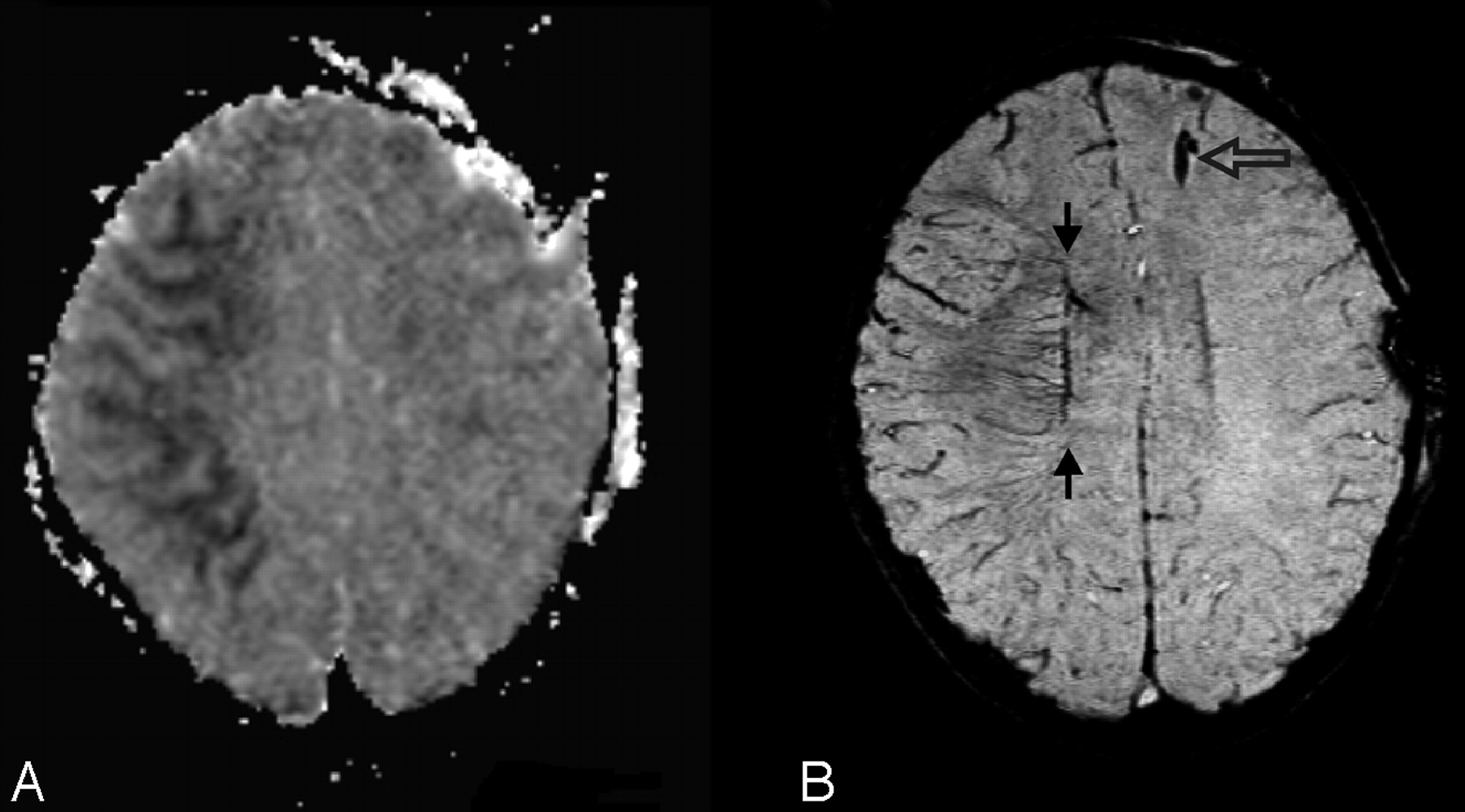
- Fig 9.
Prominent veins with infarct. This 3-year-old boy was ejected in a motor vehicle crash and was initially unresponsive with a GCS score of 3. MR imaging 3 days after injury revealed diffuse axonal injury and contusions. Axial apparent diffusion coefficient map (A) demonstrates dark signal intensity in the right middle cerebral artery territory, confirming a recent infarct. On SWI (B), there are asymmetrically prominent deep medullary veins in the right hemisphere (arrow), suggestive of increased oxygen extraction. A ventriculostomy catheter is present in the left frontal region (open arrow). He was treated with 3% normal saline for increased intracranial pressure for 2 weeks, required mechanical ventilation for 3 weeks, and evolved from coma to a vegetative and then a minimally conscious state with severe bilateral spasticity without further improvement.
- Fig 10.
Prominent veins in brain death. This 8-year-old boy was ejected in a motor vehicle crash and sustained severe TBI with an initial GCS score of 3, nonreactive pupils, and markedly elevated intracranial pressure despite aggressive treatment. Anteroposterior view of nuclear medicine brain scan 5 days later (A) demonstrates decreased but not absent cerebral blood flow as evidenced by activity in the superior sagittal sinus. MR imaging was obtained 11 days later. Axial SWI (B) shows scattered small hypointense hemorrhages (arrows) in the subcortical white matter and corpus callosum, consistent with shearing injuries. In addition, there are prominent deep medullary veins (open arrows) throughout the bilateral hemispheres. He subsequently met clinical criteria for brain death and was taken off ventilatory support 2 weeks after admission.
- Fig 11.
Calcification in tumor. This 12-year-old girl had a 2-month history of intermittent headaches, emesis, and left hemiparesis. Her initial CT scan (not available) showed moderate hydrocephalus and a fourth-ventricular mass. Conventional MR imaging images (not shown) demonstrated a partly cystic and partly solid enhancing mass. A smaller nonenhancing heterogeneous component in the right dorsal pons is noted to have a round area of markedly hypointense signal intensity (arrow) on SWI (A) that corresponds to coarse calcification (arrow) on the postbiopsy CT (B). Dilation of the temporal horns (asterisks) due to obstructive hydrocephalus is also observed. Pathology revealed a diffusely infiltrating low-grade (I-II) astrocytoma with pilocytic features. The dark signal intensity on SWI was due to calcification in this low-grade glioma.
- Fig 12.
Increased vascularity in a tumor. This 8-year-old girl presented with headache, nausea, ataxia, and vomiting. CT imaging demonstrated a large mildly lobulated hyperattenuated mass arising from the right lateral ventricle with marked surrounding white matter edema and hydrocephalus. Axial postcontrast T1-weighted image (A) shows patchy irregular enhancement of the lesion. The mass is largely isointense on the T2-weighted image (B), except for a circular dark region (open arrow) that likely reflects an area of hemorrhage. On SWI (C), the hemorrhage (open arrow) is markedly hypointense due to “blooming” effect. There are also small irregular hypointense areas in the posteromedial tumor, suggestive of increased venous vascularity (arrow). A mildly enlarged subependymal vein (arrowhead) is seen on all MR images. Pathology revealed a choroid plexus tumor with areas of anaplasia, including a high proliferative index, necrosis, and loss of architecture; most are consistent with choroid plexus carcinoma.
- Fig 13.
Fahr disease. This 15-year-old girl presented with tics, migraine headaches, and seizures. There is no significant abnormality on the T2-weighted (A) image. However, SWI (B) reveals corresponding marked symmetric hypointensity in the anteromedial globus pallidi (arrows) that corresponds to irregular coarse calcification (arrows) on the CT image (C)—both of which are much greater than expected for her age. Without the SWI, the underlying disease might not be suspected. On the basis of the imaging findings and other affected family members, she was diagnosed as having Fahr disease (idiopathic basal ganglia calcification).













In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Frequency, Extent, and Correlates of Superficial Siderosis and Ependymal Siderosis in Premature Infants with Germinal Matrix Hemorrhage: An SWI Study
- Endothelial depletion of murine SRF/MRTF provokes intracerebral hemorrhagic stroke
- Improved T2* Imaging without Increase in Scan Time: SWI Processing of 2D Gradient Echo
- Deep Medullary Vein Involvement in Neonates with Brain Damage: An MR Imaging Study
- "Brush Sign" on Susceptibility-Weighted MR Imaging Indicates the Severity of Moyamoya Disease
- Quantitative Diffusion-Weighted and Dynamic Susceptibility-Weighted Contrast-Enhanced Perfusion MR Imaging Analysis of T2 Hypointense Lesion Components in Pediatric Diffuse Intrinsic Pontine Glioma
- Attenuation of Cerebral Venous Contrast in Susceptibility-Weighted Imaging of Spontaneously Breathing Pediatric Patients Sedated with Propofol
- Demonstration of Cerebral Venous Variations in the Region of the Third Ventricle on Phase-Sensitive Imaging
- Hypoperfusion and Ischemia in Cerebral Amyloid Angiopathy Documented by 99mTc-ECD Brain Perfusion SPECT
- Pneumocephalus Mimicking Cerebral Cavernous Malformations in MR Susceptibility-Weighted Imaging
- Acute Ischemic Infarction Defined by a Region of Multiple Hypointense Vessels on Gradient-Echo T2* MR Imaging at 3T
- Imaging Cerebral Malaria with a Susceptibility-Weighted MR Sequence
- Susceptibility-Weighted Imaging: Technical Aspects and Clinical Applications, Part 2
- Susceptibility-Weighted Imaging: Technical Aspects and Clinical Applications, Part 1