
Abstract
SUMMARY: We present an unusual case of a man with human immunodeficiency virus (HIV) with pulmonary aspergillosis and spinal invasion and compression of the spinal cord occurring during a long period (3 years), as documented by MR imaging and surgical intervention. Invasive pulmonary aspergillosis with cord compression has been reported in the past, but, to the best of our knowledge, none of these have been in a patient with HIV.
Host defense against the Aspergillus species is considered to be a function of neutrophils. As such, invasive aspergillosis is relatively uncommon in human immunodeficiency virus (HIV), a disorder of lymphocyte function. We describe a case in which a man with well-controlled HIV presented with invasive pulmonary aspergillosis with cord compression. We will provide several reasons why invasive aspergillosis is thought to occur in patients with HIV, as well as describe the MR imaging features of this case, which can serve as important diagnostic clues.
Case Report
A 39-year-old man was diagnosed in 1997 with HIV. He was started on stavudine (Zerit) and lopinavir and ritonavir (Kaletra) with good control of his disease. In May 2003, his white blood cell (WBC) count was 5800 cells/uL with 58% neutrophils (reference range >34%). CD4 count was 507 (reference range >400 cells/uL) with a quantitative serum HIV count of less than 20.
In September 2003, he presented with cough and chest pain. Plain films and chest CT revealed a right upper lobe mass without definite chest wall or mediastinal invasion. He had a WBC count of 9200 with only 5.8% neutrophils and an absolute neutrophil count (ANC) of 0.5 (normal >1.6). Results of 2 CT-guided percutaneous biopsies revealed only chronic inflammation and fibrosis. Results of an open biopsy in January 2004 revealed fibrosis and “ribbonlike” fungal elements with occasional septations, for which he was given intravenous amphotericin B and, later, oral voriconazole for presumed aspergillosis. His WBC count was 6300 with 40% neutrophils and an ANC of 2.8.
The patient remained on antifungal therapy for the next 2½ years. During this time, he had a stable chest CT, WBC, and neutrophil and CD4 counts. MR imaging showed an isointense to hypointense mass on T2-weighted images, with invasion into the chest wall and mediastinum, extension into the right T1-T2 and T2-T3 neural foramina, subtle bony involvement, and minimal ventral epidural spread. Lost to follow-up, the patient presented 7 months later to the emergency department with severe right shoulder and thoracic back pain, as well as weakness in the bilateral lower extremities. Thoracic MR imaging revealed invasion into the T1–T3 vertebral bodies and posterior elements, widening of the right T1–T2 through T3–T4 neural foramina, and epidural extension with severe cord compression from T1 to T3. Again, the signal intensity of this soft tissue mass was characterized by isointensity to hypointensity on T2-weighted images with heterogeneous enhancement after administration of contrast (Figs 1 and 2). An emergency decompressive laminectomy of T1–T3 was performed with subtotal resection of the mass. Pathologic examination revealed large amounts of attenuated connective tissue with acute and chronic inflammation as well as fungal organisms with pseudohyphae. Staining confirmed aspergillosis; culture medium grew the Aspergillus fumigatus species (Fig 3).

On axial T2-weighted images (A) and postcontrast T1-weighted images (B), MR shows isointensity to hypointensity of the mass with spinal invasion, widening of the neural foramen, severe cord compression, and heterogeneous enhancement.

Sagittal postgadolinium, fat-saturated image demonstrates avid enhancement of the mass, the epidural space circumferentially, and the T1–T3 vertebral bodies.

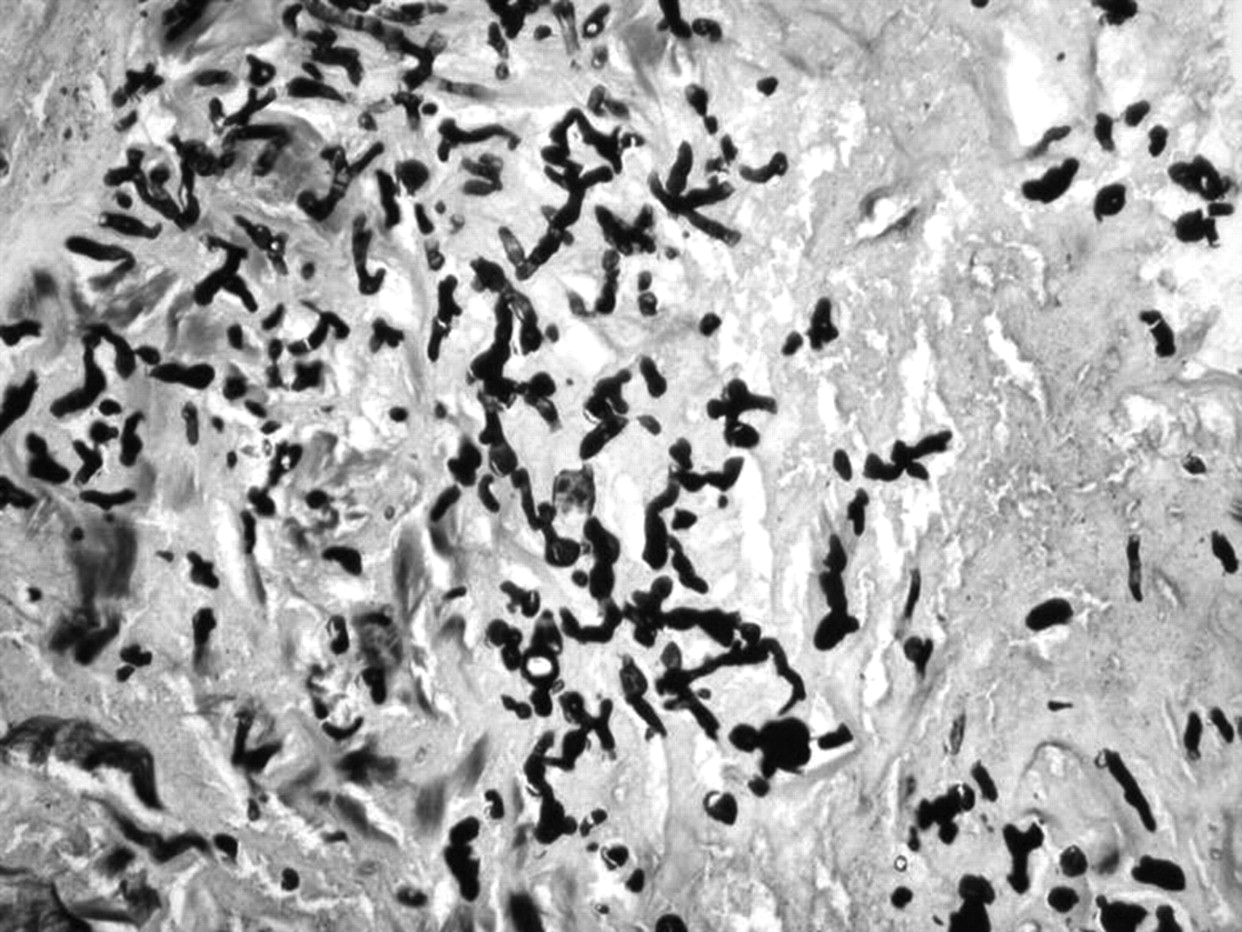
Gomori methenamine silver (GMS) stain for fungus showing branching hyphae. The fungal elements stain black (silver).
Discussion
Invasive aspergillosis has not traditionally been considered a complication of well-controlled HIV infection.1 Host defense against the Aspergillus species is postulated to be a function of neutrophils.2 As such, the frequency of Aspergillus infection is increased in patients with neutropenia, such as those with acute leukemia, or in those with abnormal neutrophil function, such as is seen in chronic granulomatous disease.1–3 Patients being treated with corticosteroids, such as transplant recipients, are also susceptible because these drugs potentiate risk for Aspergillus infection by decreasing intracellular killing of spores by macrophages, thereby allowing intracellular germination.4
HIV, on the other hand, is an infection of lymphocytes and, in isolation, should not theoretically place the patient at a higher risk for colonization and infection.2 However, studies have shown a direct relationship between severe HIV infection and neutropenia.1,5 Other possible explanations for infection in patients with HIV disease include the increasing use of corticosteroid treatment, as is used in the treatment of Pneumocystis carinii pneumonia1,6,7; neutropenia-inducing antiretroviral drugs such as zidovudine1,6; and a prolonged life of patients with late-stage HIV disease.1,6,7
We find 3 interesting features of this case. First, direct spinal invasion by pulmonary aspergillosis, though rare, is not unheard of, as several cases of chest wall invasion with epidural aspergillosis have been documented in the past.3,4,8–11 As far as we know, however, there has been only 1 reported case of epidural aspergillosis in a patient with HIV disease, and that patient was not found to have pulmonary involvement.2
Second, the initial presentation and diagnosis of pulmonary aspergillosis in this patient correlates with a relatively acute onset of neutropenia. Our patient maintained a normal neutrophil count between 1997 and early 2003 and, during that period, was asymptomatic. At the time of initial presentation, however, he was found to have significant neutropenia with only 5.8% neutrophils and an ANC of 0.5 (normal >1.6). This finding correlates with the hypothesis that host defense against the Aspergillus species is at least, in part, because of neutrophil function. It is not known why the patient became neutropenic, and it is not fully understood why the patient had progression of disease despite subsequent maintenance of normal neutrophil counts, treatment with appropriate antifungal therapy, and maintenance of CD4 counts well above 200.
Finally, the presence of isointensity to low intensity on T2-weighted images in the lesion is of interest. A study by Herold et al12 described the “targetlike” appearance of pulmonary nodular infiltrates, with low signal intensity centrally and increased intensity peripherally on both T1- and T2-weighted images. The central low signal intensity was attributed to both central cavitation and coagulative fungal necrosis, whereas the rim of increased signal intensity was attributed to subacute hemorrhage or hemorrhagic infarction. A study by Kawashima et al3 reported MR imaging findings in 2 patients with chronic granulomatous disease, pulmonary aspergillosis, and invasion into the chest wall. In both cases, the lesions were increased in T2 signal intensity. Finally, a case report by Fujimoto et al13 described low T2 signal intensity of an aspergilloma located within a cavitary lung neoplasm that showed high T2 signal intensity. In our patient, the areas of pulmonary consolidation and invasion into the chest wall were uniformly low or isointense on T2-weighted images. On pathologic examination, the resected epidural mass was found to have large amounts of attenuated connective tissue with areas of both acute and chronic inflammation. We postulate that good control of HIV in this patient allowed for production of an effective immune response, thereby producing chronic inflammatory changes and fibrosis. The fibrosis, in turn, may account for the decreased T2 signal intensity. Furthermore, the presence of paramagnetic and ferromagnetic elements intrinsic to the fungi may contribute to the T2 hypointensity.14
In summary, invasive aspergillosis is felt to have a generally poor outcome. As such, early diagnosis and treatment are imperative to survival. The radiologist should be aware of the imaging characteristics and clinical presentation of invasive aspergillosis in patients with HIV. We conclude that epidural aspergillosis should be considered even in the setting of well-controlled HIV and that the isointense to hypointense signals on T2-weighted images are a helpful diagnostic clue.
References
- Received June 20, 2007.
- Accepted after revision June 28, 2007.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.