
Abstract
BACKGROUND AND PURPOSE: Percutaneous polymethylmethacrylate (PMMA) vertebroplasty has become a common procedure for treatment of pain and disability associated with vertebral compression fractures. We reviewed the experience with our first 1000 consecutively treated vertebral compression fractures in an attempt to demonstrate both the short- and long-term safety and efficacy of percutaneous vertebroplasty.
MATERIALS AND METHODS: The first 1000 compression fractures treated by vertebroplasty at our institution were identified from a comprehensive prospectively acquired vertebroplasty data base. All patients treated with vertebroplasty were included, regardless of the underlying pathologic cause. Chart reviews of the procedure notes, imaging studies, clinical visits, and follow-up telephone interviews were performed for each patient. Evaluation at each follow-up time point included pain response (subjective and visual analog pain score), change in mobility, change in pain medication usage, and modified Roland-Morris Disability Questionnaire. Statistical analysis was performed on the pain response and change in the Roland-Morris score at each follow-up time point. Significant procedure-related complications that occurred from the time of the procedure were also specifically extracted from the patients’ charts.
RESULTS: There was a dramatic improvement in all the evaluated parameters following percutaneous vertebroplasty. The improvement in pain, mobility, medication usage, and Roland-Morris score was noticed immediately after the procedure and persisted through the 2-year follow-up. There was a low rate of complications from the procedure, the most common being rib fractures.
CONCLUSION: According to our results, practitioners can quote a high success rate and low complication rate for vertebroplasty when making treatment recommendations for painful spinal compression fractures.
Vertebral compression fractures are a common cause of pain and disability.1-5 There are many causes of vertebral compression fracture, including osteoporosis, trauma, and neoplasm. Osteoporosis among postmenopausal women and patients on long-term steroid therapy are the most frequent causes.6-8 Percutaneous polymethylmethacrylate (PMMA) vertebroplasty was introduced in the United States approximately 10 years ago, and since that time, it has become the standard of care for treatment of medically refractory vertebral compression fractures.9
Conservative management of compression fractures has traditionally included analgesics, braces, immobilization, and physical therapy.10-14 In its infancy, vertebroplasty was often deferred in favor of medical management to spare patients from a potentially risky procedure. However, bed rest and heavy narcotic usage carry a significant set of risks that are potentially avoided with early treatment, and practitioners are performing the procedure earlier as they become more experienced.
The literature contains many small case series on the effectiveness of percutaneous vertebroplasty.15-20 Most of these reports are confined to the treatment of osteoporotic compression fractures and contain a limited evaluation of follow-up results. We provide a comprehensive review of the experience with vertebroplasty at a large academic center and evaluate multiple outcome measures over both short- and long-term follow-up periods.
Materials and Methods
Patient Population
There were 552 patients treated between February 1999 and October 2005. These 552 patients underwent 673 sessions to treat 1000 spinal compression fractures. Sixty-three percent of the treatment sessions (425/673) involved treatment of a single level, whereas 27% (180/673) involved 2 levels, 9% (58/673) involved 3 levels, and 1% (9/673) involved 4 levels. A single case involved treatment of 5 levels, but there were no cases in which treatment of more than 5 fractures was performed in a single session. The average age of patients in our study was 74 years (SD, 10.8 years) with a range of 28–96 years. As expected, a significant percentage of the patients were women. Sixty-nine percent (379/552) were women, whereas 31% (173/552) were men.
Selection Criteria
Institutional review board approval was granted for this study. Vertebroplasty was offered to patients with imaging evidence of an acute or subacute compression fracture of the thoracolumbar spine. Patients with all causes of compression fracture were included in the study. Exclusion criteria for vertebroplasty typically included response to medical management, noncorrelating pain, systemic or spinal infections, and technical factors such as gracile pedicles or vertebra plana. Patients with other causes for pain such as disk herniation, spinal stenosis, or foraminal narrowing were also excluded unless a coexistent compression fracture was thought to contribute significantly to their symptoms. Although most patients were treated initially with conservative medical management, inpatients with intractable pain were offered the procedure earlier than those with pain of less severity. Even patients with prolonged symptoms occurring for many months were offered vertebroplasty if they had correlating pain with evidence of an unhealed fracture. An unhealed fracture was diagnosed if there was persistent edema on MR imaging or corresponding radiopharmaceutical uptake on bone scintigraphy studies. Rarely, patients without vertebral edema on MR imaging or radiopharmaceutical uptake were considered to have an unhealed fracture if there was focal pain with palpation at fluoroscopy corresponding to a known vertebral compression fracture. The average duration of symptoms before treatment was 3.6 months.
Vertebroplasty Procedure
All vertebroplasty procedures were performed by neuroradiologists with expertise in spinal interventions. A preprocedure consultation was performed by a neuroradiologist usually within a few days of the procedure, and this consultation included a focused physical examination with fluoroscopic confirmation of correlating pain. Depending on the patient's underlying medical condition, procedures were performed with the patient under conscious sedation, deep sedation, or general anesthesia. Conscious sedation consisted of intravenous fentanyl and midazolam and was usually begun before placing the patient prone on the fluoroscopy table. Biplane fluoroscopy was used in all cases. After placing the patient prone on the table, we confirmed the fractured level with previously obtained imaging studies and the level to be treated was localized by counting from above and below. Local anesthetic consisted of subcutaneous 1% lidocaine and 0.25% bupivacaine into the deep soft tissues and periosteum with a 22-gauge spinal needle. An 11- or 13-gauge needle with an inner stylet was then advanced under fluoroscopic guidance by using a transpedicular or parapedicular approach into the vertebral body. When the needle was at the junction of the pedicle and body, a biplane digital radiograph was obtained to confirm an appropriate trajectory and exclude a breech of the medial pedicle. The needle was then advanced into the anterior one third of the vertebral body in an attempt to reach the midline. At this point, biplane images were again obtained before PMMA injection. Under a vented hood, a mixture of PMMA, barium, and 1 g of gentamicin was prepared. The cement was injected with an injection device or with 1-mL syringes under biplane fluoroscopic observation until it reached the posterior one fourth of the vertebral body.
The injection was terminated if venous, disk space, or epidural extravasation was encountered. If inadequate filling of the contralateral hemivertebra was noted, a 2nd needle was placed into the contralateral side and additional cement was injected. Patients were instructed to remain supine for 2 hours after the procedure to allow for cement hardening and resolution of sedation. After 2 hours of bed rest, they were evaluated at the bedside and were allowed to ambulate. Outpatients were then discharged, whereas inpatients were allowed to ambulate as tolerated. Up to 5 levels were treated at a single session in the early days of our practice. However, we now typically bring patients back for a 2nd procedure if more than 3 fractures need treatment.
Outcome Measures
At the time of the preprocedure consultation, patient mobility, pain medication usage, visual analog pain scale (0–10) at rest and with activity, and a modified Roland-Morris Disability Questionnaire score were obtained by trained vertebroplasty nurses and neuroradiologists. The Roland-Morris scale was routinely instituted in our practice halfway through the study period because of its specificity in evaluating patients with compression fractures.21 The visual analog scale was answered in the standard fashion, with 0 being no pain and 10 being the worst pain ever experienced. Preprocedure pain medication type (narcotic versus nonnarcotic), frequency, and route (oral versus intravenous) were recorded. Two hours after vertebroplasty, patients were examined and a visual analog pain score was obtained at rest and with activity. Follow-up telephone interviews were conducted by vertebroplasty nurses at 1 week and 1, 6, 12, and 24 months postprocedure. The inability to contact a patient for 1 time point did not preclude contact at later follow-up time points. Data recorded from the follow-up telephone interviews included subjective and visual analog pain scores at rest and with activity, Roland-Morris score, changes in medication use and mobility, and any complications or new fractures that were encountered.
Statistical Analysis
Statistical analysis was applied to the visual analog pain scores at rest and with activity as well as to the Roland-Morris score response. A nonpaired 2-tailed t test was applied to each follow-up time point to assess the significance of pain response and improvement in the Roland-Morris score.
Results
General Patient Characteristics
In the course of our study, 1000 thoracolumbar vertebral compression fractures were treated during 673 procedures in 552 patients. The average cement volume injected was 3.3 mL per level. Conscious sedation was used in 85% (574/673) of patients, with general anesthesia in 12% (79/673) and deep sedation in 3% (20/673). Most of the patients who underwent general anesthesia did so early in the course of the study (Fig 1). As we became more experienced with the procedure, patients were more likely to be treated under conscious sedation. There was a slight decrease in the number of procedures performed during the last year of the study. This is explained, in part, by the inclusion of only 10 months of data during 2005. Additionally, we have recently noticed a small decrease in our vertebroplasty volumes as the procedure is increasingly performed at more institutions. Patients who were referred to our institution early in the course of our study are now more often treated locally as experience with the procedure expands.

Number of procedures performed with the patient under general anesthesia with time.
Eighty-four percent (562/673) of procedures were performed for compression fractures related to osteoporosis. Compression fractures related to neoplastic involvement were the next most common and accounted for 11% (74/673) of procedures. The remaining 5% (37/673) of patients had fractures caused by hemangiomas or trauma. Although osteoporosis was the most common cause of vertebral compression fracture in both sexes, neoplastic fractures were a more common cause in men (17%) compared with women (8%). Similar to previously reported case series, vertebral compression fractures occurred more commonly at the thoracolumbar junction, with T12, L1, and L2 accounting for 41% of treated levels (Fig 2).22 To obtain a tissue diagnosis for a vertebral compression fracture, we performed a percutaneous biopsy in 9% (61/673) of patients before injection of PMMA. Seventy-nine percent (534/673) of patients underwent vertebroplasty as an outpatient procedure, and 21% (139/673) of procedures were performed on inpatients.

Distribution of treated compression fractures.
Twenty-three percent of the procedures (156/673) were followed by a new compression fracture or fractures, whereas 77% (517/673) did not develop a new fracture. Of the 156 new fractures, 106 (68%) underwent another vertebroplasty procedure.
Outcome Measures
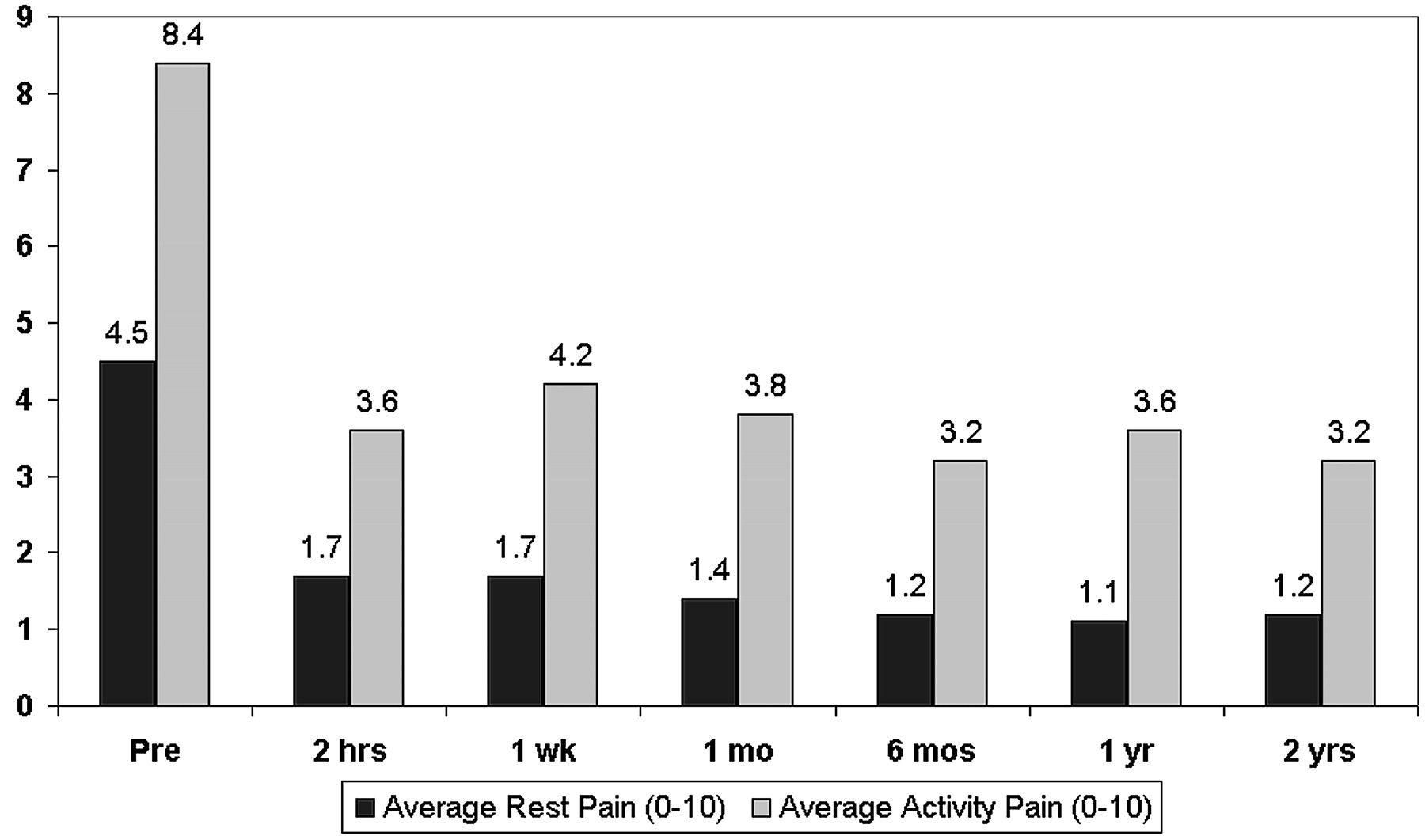
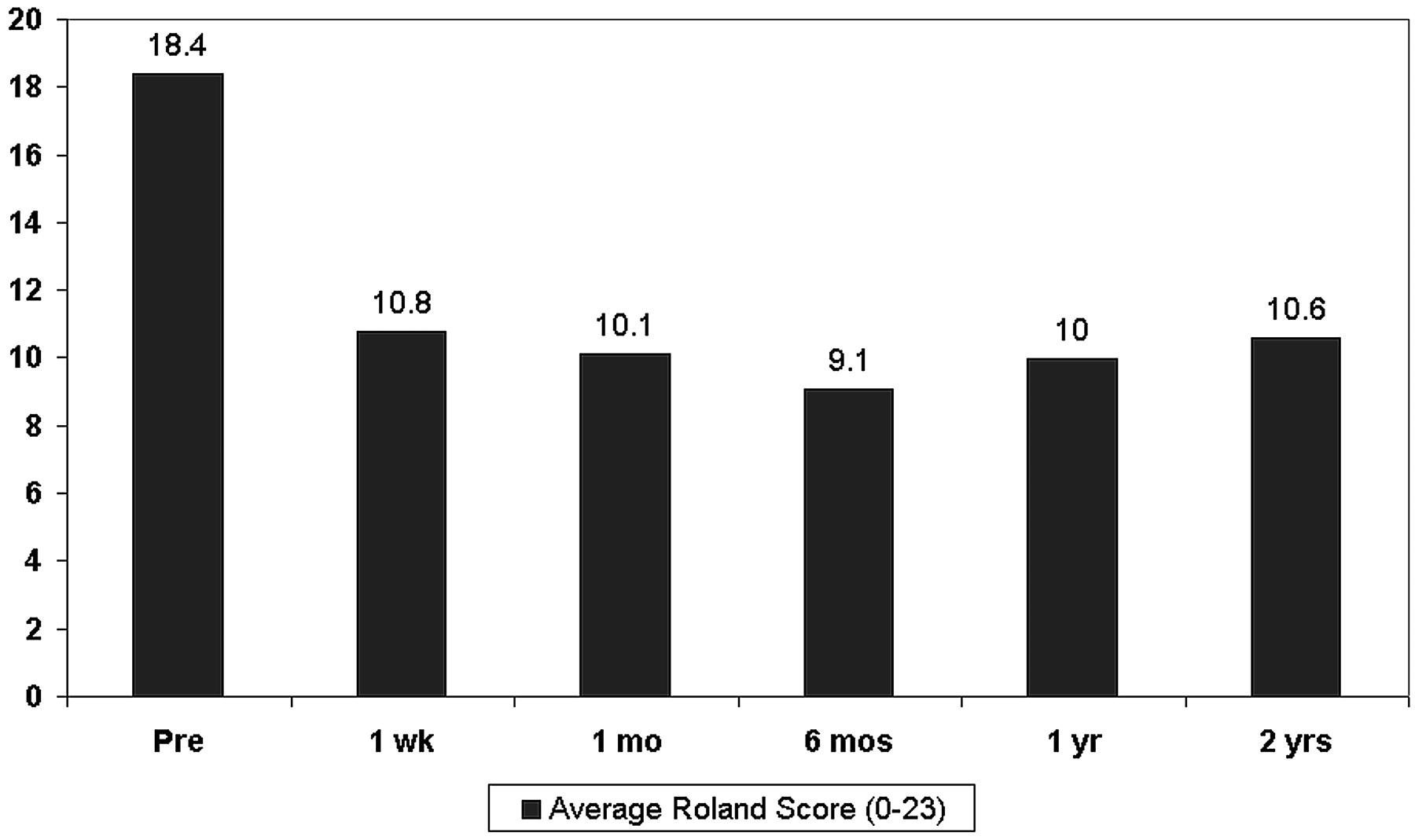
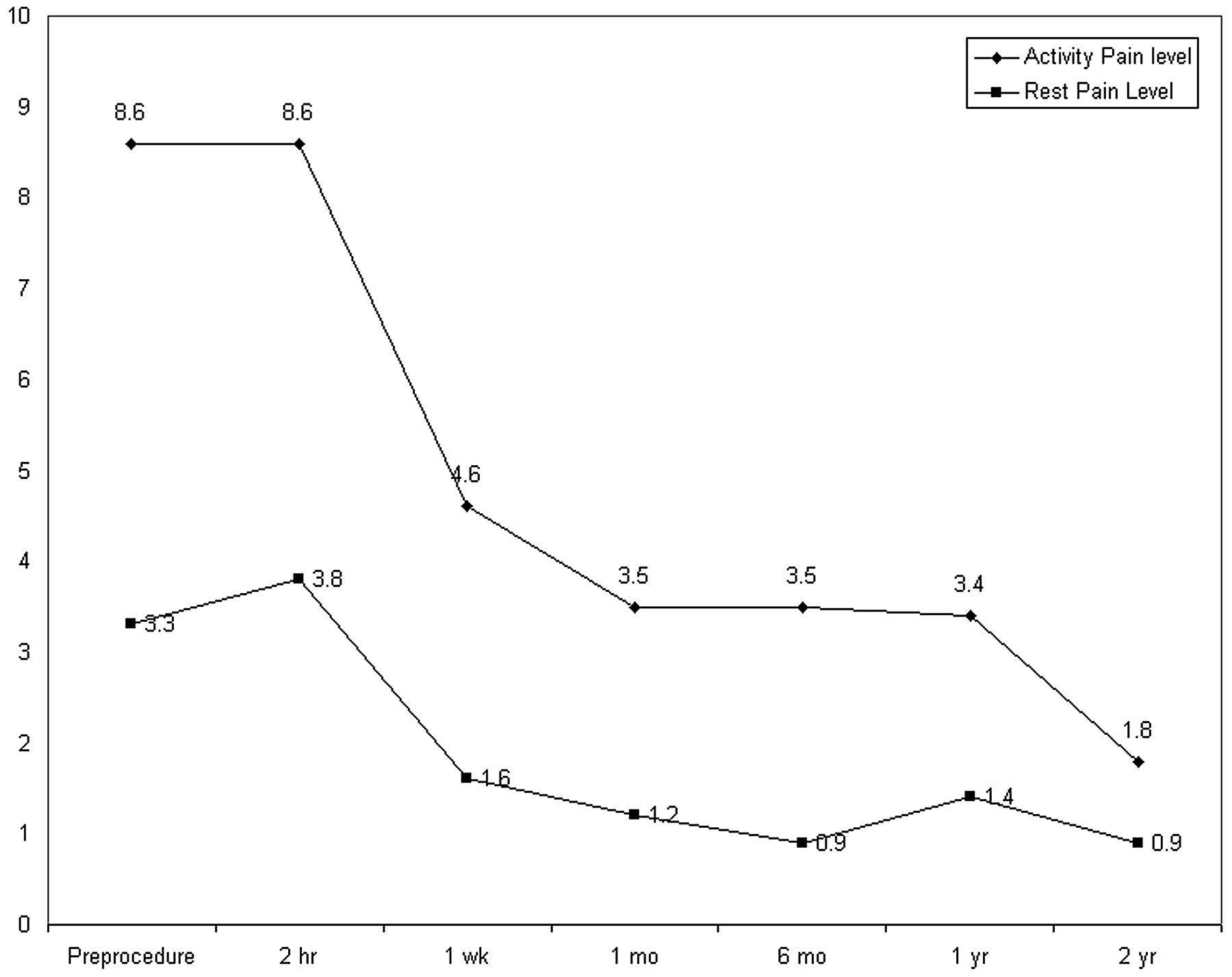
Compared with the preprocedure visual analog pain score, a significant decrease in pain was seen at rest and with activity. The pain response was apparent at the 2-hour postprocedure evaluation and persisted for every follow-up time point up to 2 years (Fig 3). Similarly, there was a significant improvement in the Roland-Morris score that was apparent at the 1-week follow-up, and this was sustained throughout the 2-year follow-up period (Fig 4). Of significance, the decrease in visual analog pain score and the Roland-Morris score was highly statistically significant at every follow-up time point, with a P value of <.001. In our patient population, we had a relatively high rate of follow-up. We were able to obtain follow-up assessments in 89%, 84%, 75%, 67%, and 62% of patients at 1 week and 1, 6, 12, and 24 months, respectively. Most patients also reported an improvement in their mobility, a decrease in pain medication usage, and a qualitative decrease or complete resolution of their pain throughout the 2 years of follow-up (Table). Occasionally, patients reported no change in their pain at the initial 2-hour follow-up examination. We specifically evaluated this subset of patients to determine what their pain response was at later follow-up time points. Despite reporting no pain relief or worsening of pain at the 2-hour follow-up, most of these patients did get eventual pain relief as demonstrated by a similar decrease in visual analog pain scale at the 1-week through 2-year follow-up time points when compared with that of the entire patient population (Fig 5).

Pain relief following vertebroplasty by using the visual analog pain scale.

Comparison of the average Roland-Morris score before and after vertebroplasty.

Visual analog pain score changes in the subset of patients who did not experience any pain relief at the 2-hour postprocedure evaluation. Despite no pain relief at 2 hours, these patients experienced significant pain relief at the remaining follow-up time points up to 2 years.
Percentage of patients with improvement in mobility, pain medication usage, and subjective pain after vertebroplasty.
Complications
Clinically significant complications were encountered in only 12 patients (1.8%). Rib fractures related to lying prone on the fluoroscopy table for the vertebroplasty procedure were the most common complication encountered and occurred in 7 patients (1%). Any patient with focal chest wall pain that occurred after the procedure and was clinically referable to the ribs was considered to have a fracture, even if rib radiographs could not confirm a definite fracture. Therefore, it is possible that some of the rib fracture complications recorded could have been related to muscle pain rather than an actual fracture. A single patient was noted to have a transverse process fracture on the side of vertebroplasty needle placement that resulted in 2 weeks of paraspinal pain.
One patient had a clinically significant cement pulmonary embolus. This small embolus was immediately recognized because it occurred during the cement injection, resulting in termination of further cement injection. The patient reported pleuritic chest pain after the procedure and became dyspneic. Although a chest CT did reveal a cement pulmonary embolus, there were no long-term sequelae and the patient made a full recovery.
Five patients had new-onset radiculopathy in our study. However, 3 of these incidents were transient and without a radiographically identifiable cause, and only 2 clinically significant radiculopathy complications were encountered. In these 2 patients, the radiculopathy persisted for several months, and there was radiographic evidence for cement in or very near the neural foramen at the treated level.
A single patient had central spinal canal compromise in a neoplastic fracture. The posterior cortex of the vertebral body was disrupted on a preprocedure CT scan. Although cement was cautiously placed in the vertebral body and no extravertebral leakage was observed, the patient became symptomatic after the procedure, with evidence for neural compression. A postprocedure CT demonstrated interval posterior displacement of tumor into the canal, which required surgical decompression.
Of significance, no infectious complications were encountered in our study population, and no deaths were attributable to the vertebroplasty procedure.
Although we do not consider minimal asymptomatic extravertebral cement extravasation to be a complication of vertebroplasty, any aberrant cement placement during the procedures was recorded. Cement leakage into paravertebral veins, epidural veins, intervertebral disk space, and pulmonary vasculature was encountered in 170 patients (25%). There were 8 patients with cement leakage, with migration of a small amount of cement to the pulmonary vasculature. However, only 1 of these patients (discussed previously) became symptomatic. In the remaining 7 patients, there was no change in pulse oximetry readings or clinical status. This was likely due to the immediate recognition of cement extravasation and termination of injection. In 503 procedures (76%), no aberrant cement placement was encountered (Fig 6).

Distribution of cases with cement leakage outside the vertebral body.
Discussion
Our study addressed both the short- and long-term outcomes for patients treated with vertebroplasty for vertebral compression fractures of all causes. In our study, most of the patients undergoing vertebroplasty were women, and the most common cause for vertebral compression fracture was osteoporosis. We found an immediate improvement in the degree of pain after vertebroplasty that was present even at the 2-hour postprocedure follow-up evaluation. This improvement in pain continued for all follow-up time-points up to 2 years and was accompanied by a similar improvement in spine-related disability, mobility, and pain medication usage.
There was a low complication rate in our study, and no procedure-related infection or death was encountered. All of the complications that we encountered have been described in previous vertebroplasty case reports.9,23,24 Rib fractures occurring at the time of vertebroplasty accounted for most of our complications and are not surprising given that the patients who undergo vertebroplasty procedures are predisposed to rib fractures. In fact, many patients who were treated with vertebroplasty were noted to have rib fractures from minor trauma present before the procedure. We began performing percutaneous vertebroplasty in 1999, and much of our early experience was gained at a time when vertebroplasty literature was sparse and techniques were still evolving. Because we included the procedures at the beginning of our experience, the complication rate for vertebroplasty would be expected to decrease even further because of the experience we have gained with our first 1000 levels.
To our knowledge, this is the largest reported comprehensive series on the outcomes related to percutaneous vertebroplasty. Previous articles on vertebroplasty outcomes have focused on specific etiologies such as osteoporosis or neoplasm. We reported on our experience with vertebroplasty in all patients, regardless of the underlying pathologic process. Patients in our study were followed up at specific intervals that included both short-term 2-hour evaluation and long-term 2-year follow-up interviews. This consistent extended follow-up allowed us to document both the short- and long-term outcomes associated with vertebroplasty and a sustained response to treatment. In an attempt to accurately document the complication rate of vertebroplasty, we performed a thorough chart review. Besides evaluating the radiology reports and radiology department follow-ups, we also reviewed all clinical follow-up visits with all clinical care providers in our institution. This was easily performed because of a systematic electronic medical record at our institution that includes all follow-up contacts, either in person or by telephone. Such a rigorous follow-up is needed to document completely all potential complications.
There are numerous outcome measures recorded in the vertebroplasty literature that attempt to validate this procedure in the treatment of vertebral compression fractures. However, there is significant variability in the outcome measures used to assess the viability of vertebroplasty. The most commonly reported measure is the visual analog pain score, which does provide important information to practitioners. However, relying on pain alone as an outcome measure fails to assess completely the adequacy or inadequacy of vertebroplasty for treating compression fractures. In a report by Trout et al, 21 the importance of a comprehensive tool for spine-related disability, the Roland-Morris Disability Questionnaire, was documented. Any assessment of vertebroplasty should include an analysis of spine-specific measures of pain and disability. Our study incorporated the Roland-Morris Disability Questionnaire and an assessment of mobility and pain medication usage in a large number of patients.
Reported complication rates from percutaneous vertebroplasty have been low.9,17,25,26 Even with an extensive review of the patients’ charts in our study, we report a clinically significant complication rate of only 1%–2%. The low complication rate in our series is likely related to the expertise and subspecialization of the operators. All of the procedures included in our study were performed by neuroradiologists with a specific interest in spine intervention. Epidural, paraspinal, intradiskal, and venous cement extravasation rates for percutaneous vertebroplasty are relatively high and have been documented to occur in up to 88% of patients.27-30 In our study, 25% (170/673) of patients had some form of cement leakage documented. The documented cases of cement leakage in our study were based on fluoroscopically visualized cement outside the vertebral body at the time of the procedure. Our patients do not routinely undergo CT evaluation afterward, but this percentage would likely be higher if CT were performed to detect smaller areas of cement extravasation. On the basis of our and others’ results, it is apparent that small amounts of cement leakage alone should not be considered a complication of vertebroplasty. It is important to recognize cement leakage during the procedure so that it can be terminated or the contralateral pedicle entered, but cement leakage should be considered a stopping point for injection rather than a complication. Despite a cement leakage rate of at least 25% in our series, the clinically significant complications related to cement leakage occurred in only 3 patients (0.45%) and included 2 patients with radiculopathy and a single cement pulmonary embolus. Therefore, claims that kyphoplasty is safer than vertebroplasty because of a decreased rate of cement leakage are unfounded.31,32
Our study has several limitations. Although we report on a large patient population with consistent outcome measures, our study is a retrospective review of a prospectively acquired data base. As with most studies on vertebroplasty, there is a potential for bias when patients are evaluated at follow-up. It is possible that the nurse or physician administering the follow-up questions could unintentionally influence the responses that patients gave, depending on how the questions were asked. Because many of the patients were older and resided in nursing homes, it is possible that responses to the follow-up questions were occasionally provided by family members or healthcare providers who interacted with the patients on a daily basis. In those cases in which the patient was unable to give responses to the follow-up questions because of disability or dementia, the responses recorded on follow-up from a surrogate interviewee may not accurately reflect the response intended by the patient. Although we did include responses from surrogate interviewees during follow-up interviews, these responses were limited to a basic assessment of pain, mobility, and medication usage. Surrogate responses were not recorded for the quantitative visual analog pain scores or Roland-Morris Disability Questionnaire.
Although vertebroplasty is considered to be the treatment of choice for painful vertebral compression fractures by many physicians, it has yet to be validated by a prospective randomized study. There are randomized prospective studies currently underway in the United States and internationally, such as the Investigational Vertebroplasty Efficacy and Safety Trial (INVEST), that will address this shortfall in the current vertebroplasty research.33 It is only after the results of these studies are available that we can unequivocally state that vertebroplasty has been validated as a treatment option for patients with painful compression fractures.
Conclusion
On the basis of our results, percutaneous PMMA vertebroplasty is a safe and effective method to treat vertebral compression fractures. An immediate improvement in pain can be expected for most patients, and disability, mobility, and pain medication use are improved during the short- and long-term periods. The complication rate of vertebroplasty is low, with rib fractures being the most common clinically significant complication.
Footnotes
A subset of the data in this manuscript was presented at: American Society of Spine Radiology Annual Symposium, February 23–26, 2006, Las Vegas, Nev, where it won the Mentor Award for Best Paper Presentation. It was also previously presented at: NER Foundation & Annual Meeting of the American Society of Neuroradiology, April 29–May 5, 2006; San Diego, Calif.
References
- Received April 19, 2006.
- Accepted after revision June 17, 2006.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Is Severe Pain Immediately after Spinal Augmentation a Predictor of Long-Term Outcomes?
- Percutaneous vertebroplasty for subacute and chronic painful osteoporotic vertebral compression fractures can safely be undertaken in the first year after the onset of symptoms
- Extending the Arm of Augmentation Beyond the Neuroaxis
- The Association between the Duration of Preoperative Pain and Pain Improvement in Vertebral Augmentation: A Meta-Analysis
- Mortality in the Vertebroplasty Population
- Discharge Disposition Following Vertebroplasty
- Treatment of painful osteoporotic vertebral compression fractures: A BRIEF REVIEW OF THE EVIDENCE FOR PERCUTANEOUS VERTEBROPLASTY
- Asymptomatic and Unrecognized Cement Pulmonary Embolism Commonly Occurs with Vertebroplasty
- Have Referral Patterns for Vertebroplasty Changed since Publication of the Placebo-Controlled Trials?
- Palliation of compression fractures in cancer patients by vertebral augmentation: a retrospective analysis
- Social responsibility in medical reporting
- Percutaneous Vertebroplasty Is Not a Risk Factor for New Osteoporotic Compression Fractures: Results from VERTOS II
- P.S. Augmentation
- Randomized Vertebroplasty Trials: Bad News or Sham News?
- Baseline Pain and Disability in the Investigational Vertebroplasty Efficacy and Safety Trial
- Kyphoplasty and Vertebroplasty Produce the Same Degree of Height Restoration
- Clinical Outcomes with Hemivertebral Filling during Percutaneous Vertebroplasty
- Percutaneous vertebroplasty for the treatment of osteoporotic vertebral compression fractures: EVALUATION AFTER 36 MONTHS
- Vertebroplasty for the Treatment of Traumatic Nonosteoporotic Compression Fractures
- Efficacy of Percutaneous Vertebroplasty for Multiple Synchronous and Metachronous Vertebral Compression Fractures
- Vertebroplasty for osteoporotic vertebral fracture