
Abstract
BACKGROUND AND PURPOSE: Our purpose was to evaluate the differential findings of tuberculous otomastoiditis (TOM) and nontuberculous chronic otomastoiditis with or without middle ear cholesteatoma on high-resolution CT of the temporal bone.
MATERIALS AND METHODS: We reviewed 19 cases of TOM, 30 cases of chronic otomastoiditis (COM), and 30 cases of COM with cholesteatoma (CHOM), all of which had been confirmed by pathologic examination after surgery or middle ear mucosal biopsy. Two neuroradiologists analyzed the findings of temporal bone CT.
RESULTS: The soft tissue attenuation in the entire middle ear cavity, preservation of the mastoid air cells without sclerotic change, and soft tissue extension to the external auditory canal (EAC) or mucosal thickening of the bony EAC, had statistical significance (χ2 test, P < .05) between the TOM group and the COM group and between the TOM group and the CHOM group. Erosion of the ossicles and scutum was statistically significant (χ2 test, P < .05) between the TOM group and the CHOM group.
CONCLUSION: Findings of soft tissue in the entire middle ear cavity, preservation of mastoid air cells without sclerotic change, soft tissue extension, or mucosal thickening of the EAC with intact scutum seemed to be helpful in differentiating TOM from COM and CHOM.
High-resolution CT (HRCT) of the temporal bone has commonly been used in the evaluation of the chronic suppurative otitis media because of its high sensitivity in the presence of soft tissue disease and bone erosion.1,2 However, specific diagnosis of middle ear disease on HRCT of the temporal bone is difficult because of the insensitive soft tissue contrast of this technique. CT is the best imaging technique available for diagnosing tuberculous otomastoiditis (TOM); CT provides more information than do standard plain films, and it is more accurate and useful than polycycloidal tomography and MR imaging.3
TOM is a rare cause of chronic suppurative otitis media. The early diagnosis of TOM is not easy because of its low prevalence, ambiguous clinical signs, and false-negative culture.4–7 There is frequently a considerable delay before diagnosis, which can lead to irreversible complications such as permanent hearing loss and facial nerve paralysis. Knowledge of the clinical manifestation and radiologic findings of TOM is needed for early diagnosis of TOM, because this is important to initiate medical treatment to eradicate the infection and is helpful for determining whether surgical intervention is necessary to prevent potential complications.8,9 Most reports of TOM are in regard to its clinical aspects4–6,10–18 and only briefly discuss the radiographic4,11,12 and CT findings.14–18 However, radiologically focused reports have been rare.3,19
In this study, we evaluate the differential findings of TOM compared with nontuberculous chronic otitis media with or without cholesteatoma on HRCT of the temporal bone.
Materials and Methods
We searched computerized pathology reports and found 38 cases of TOM, proved by operative or middle ear mucosal biopsy, at Masan Samsung Hospital over the past 10 years. The criteria for histopathologic diagnosis of the TOM included characteristic central caseation necrosis surrounded by epithelioid and multinucleated giant cells with or without positive stain of the acid fast bacilli. When mycobacteria could not be identified by histologic examination or by culture of biopsy specimens, results of the histologic examination showed tuberculoid granuloma, and other causes of granulomatous infection (such as fungal infections, Wegener granulomatosis, midline granuloma, sarcoidosis, syphilis, histiocytosis X, and necrotizing otitis extern) must be considered in the differential diagnosis. If these possibilities are excluded, and because Masan City, Korea is endemic in tuberculosis, a course of antituberculous chemotherapy should be given. The diagnosis of TOM can be also justified by the good response.7,11,12,14,15
However, only 19 of these patients underwent CT scanning. Our study population included 7 men and 12 women. Patient ages at the time of diagnosis ranged from 5 to 49 years (mean age, 30 ± 12.5 years). The time interval from the CT scans to surgery or mucosal biopsy ranged from 1 to 90 days (mean, 22 ± 29 days). We also searched pathologic reports over the last 10 years and randomly selected 30 cases of nontuberculous otitis media (COM) and 30 cases of nontuberculous otitis media with middle ear cholesteatoma (CHOM) for comparison groups. The COM group consisted of 14 men and 16 women, aged 17 to 58 years (mean age, 36.5 ± 9.5). The CHOM group included 13 men and 17 women, aged 24 to 58 years (mean age, 37.5 ± 7.4). The time interval from the CT scans to surgery ranged from 1 day to 2 months (mean, 20 ± 15 days) and from 3 to 70 days (mean, 18 ± 20 days).
CT examination of the middle ear was then conducted, taking 1- or 1.5-mm axial and coronal images with 1- or 1.5-mm intersection gaps. The CT scanners used were the GE 9800 or the HiSpeed Advantage (General Electric Medical Systems, Milwaukee, Wis). The axial and coronal images were obtained at angles of approximately 30° and 120°, respectively, to the infraorbitomeatal line.
The CT scans were interpreted without clinical information and operative findings by 2 radiologists whose major job for several years had been interpretation of head and neck imaging. Two experienced radiologists read retrospectively the CT scans in consensus. The following imaging findings were evaluated: 1) soft tissue location (mastoid antrum, middle ear cavity; epitympanum, mesotympanum, hypotympanum); 2) mucosal thickening of the bony external auditory canal (EAC) or soft tissue extension to the EAC (ie, soft tissue beyond the tympanic eminence); 3) preservation of mastoid air cells without sclerotic change; 4) erosion of ossicles; 5) erosion of the scutum; 6) erosion of the bony labyrinth; 7) erosion of the facial nerve canal; 8) erosion of the tegmen tympani; and 9) erosion of the sigmoid sinus plate.
Statistical analysis was undertaken to determine the validity of the differential findings between the tuberculous and nontuberculous otitis media. The χ2 test was used to determine the statistical significance between the TOM and COM groups and between the TOM and CHOM groups. Fisher exact test was performed if the cell (expected value <5) was more than 25%. A P value <.05 was considered statistically significant.
Results
Table 1 shows HRCT findings of these 3 groups. In TOM, 18 of 19 patients exhibited a soft tissue attenuation lesion in the entire middle ear cavity, the mastoid antrum, and the mastoid cells. In 14 patients, the mastoid air cells were well preserved without significant sclerotic change in the surrounding mastoid bone (Fig 1). The soft tissue extension to the EAC or mucosal thickening of the bony EAC was present in 12 patients (Fig 2). Erosion of the middle ear ossicles was seen in 6 patients. Only 1 patient had erosion of the lateral semicircular canal on temporal bone CT.

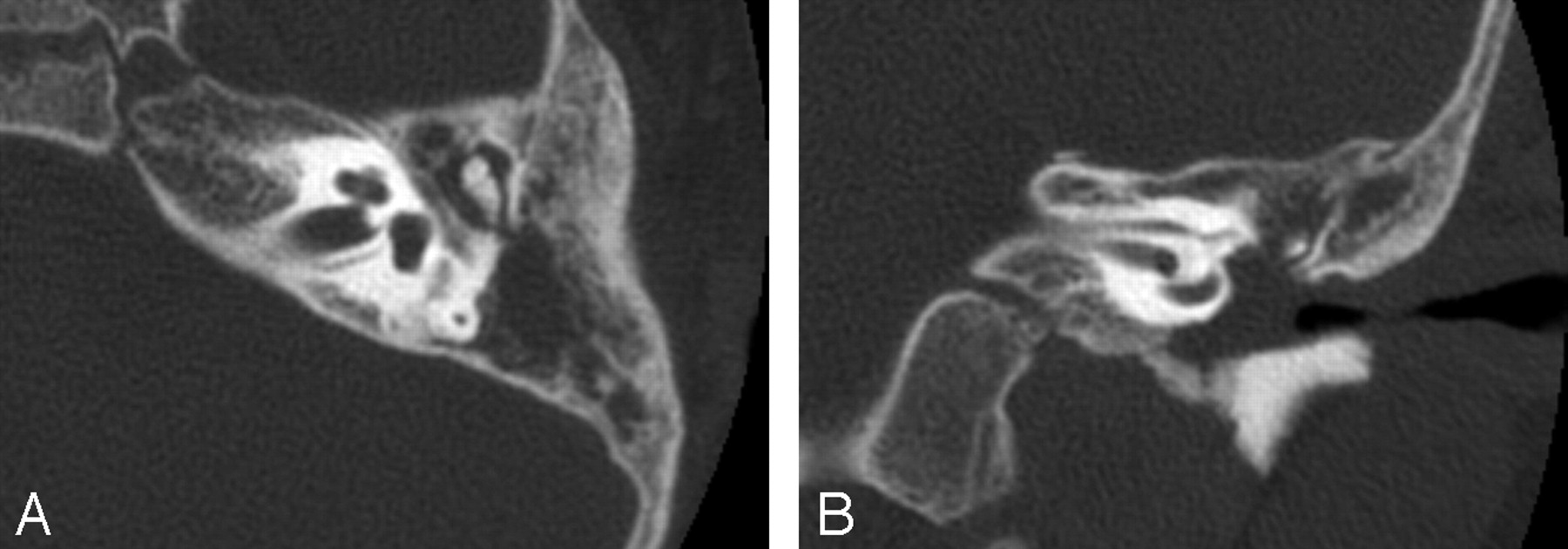
A 32-year-old woman presented with recurrent otorrhea for several years. Postoperative histologic diagnosis was tuberculous otomastoiditis. Axial (A) and coronal (B) CT scans of the temporal bone show a soft tissue attenuation lesion in the entire middle ear cavity, the mastoid antrum, and the cells. The mastoid air cells were well preserved without significant sclerotic change in the surrounding mastoid bone.

A 6-year-old boy presented with otorrhea of several months’ duration. Otoscopic examination of the ear showed total perforation of the tympanic membrane. Postoperative histologic diagnosis was tuberculous otomastoiditis. Axial (A) and coronal (B) CT scans of the temporal bone show soft tissue masses in the tympanic cavity with extension to the external auditory canal and mucosal thickening of the bony external auditory canal.
HRCT findings for tuberculous otomastoiditis and nontuberculous otomastoiditis
The soft tissue attenuation in the entire middle ear cavity, preservation of the mastoid air cells without sclerotic change, and soft tissue extension to the EAC or mucosal thickening of the bony EAC had statistical significance (P < .05) between the TOM group and the COM group and between TOM group and the CHOM group. Erosion of the ossicles and scutum was statistically significant (P < .05) between the TOM group and the CHOM group.
Discussion
Our HRCT findings of TOM in this study were soft tissue in the entire middle ear cavity, preservation of mastoid air cells without sclerotic change, and soft tissue extension or mucosal thickening of the EAC with intact scutum. These CT findings were consistent or not consistent with other reports.3,14–19
Radiographic findings may include destruction of the ossicles, sclerosis of the mastoid cortex, or opacification of the middle ear and mastoid air cells, which are seen on COM. Sclerosis of the mastoid is denser and more widespread in the case of TOM than in COM of other cause.4 However, the relatively high incidence of normal cellular development of mastoid bone has been noted in other studies11,12 and seems to be a significant finding. In our study, preservation of mastoid air cells without sclerosis of the mastoid bone was noted in 14 of 19 patients and agreed with the radiologic findings of TOM in the Windle-Taylor and Ma studies.11,12 Cavallin and Muren19 demonstrated widespread soft tissue densities in the tympanic cavity and in the mastoid process, with bone erosions in the latter on CT scans. Hoshino et al3 reported that a cochlear fistula seemed to be characteristic of advanced TOM. We were unable to observe cochlear fistula in our patients because of the earlier stage of TOM in our patients than in the patients in the studies by Hoshino et al3 or Cavallin and Muren.19 In recent studies,16,17 CT scans demonstrated soft tissue masses in the tympanic cavity, the antrum, and the mastoid cells without evidence of bone erosion in 15 of 18 cases. A large amount of soft tissue in the middle ear cavity was noted in TOM and CHOM compared with COM, but in patients with CHOM, erosion of the scutum and ossicles was frequently coexistent. Mucosal thickening of the bony EAC or soft tissue extension to the EAC were other statistically significant findings in TOM. Mucosal thickening of the EAC in CHOM is usually responsive to medical treatment, but the mucosal thickening in TOM may persist despite antibiotic therapy. Therefore, the persistent mucosal thickening of EAC despite antibiotic therapy may be a finding of TOM.
TOM is considered a prototype disease for most of the true granulomas that can occur in the temporal bone. Histologic studies of tuberculous lesions generally reveal caseous foci that are surrounded by epithelioid or histiocytic cells, multinucleated inflammatory cells, and mixed acute and chronic inflammatory cells as well as fibrous granulation tissue. Definitive diagnosis, however, requires identification of the acid-fast bacilli by either culture or appropriate tissue staining.20 Yaniv4 reported that only 4 patients were positive on a microscopic examination of ear discharge for acid- and alcohol-fast bacilli in 28 of their study patients. In the series of Windle-Taylor and Bailey,11 the diagnosis was established by histologic examination in 20 of 22 patients. Recently, Nishiike et al16 also described that smears of patients’ otic secretion for acid- and alcohol-fast bacilli were examined in 11 ears but were positive in only 3 ears. Six microscopic examinations showed that in only 1 granuloma should acid-fast bacilli be present. Only 5 of our 19 patients had positive results for acid-fast bacilli staining on histologic examination. However, most patients showed typical caseation necrosis and Langerhans giant cells. This area is endemic in tuberculosis and most patients had a good response to antituberculous chemotherapy.
The pathogenesis of TOM is postulated to involve 3 mechanisms: 1) aspiration of mucus through the eustachian tube, 2) hematogenous dissemination from other tuberculosis foci, or 3) direct implantation through the EAC and a tympanic membrane perforation.11,15,16,20 We think that many of our patients were infected by direct implantation because they showed no evidence of tuberculosis in other sites, except 1 case with pulmonary tuberculosis and 1 case with cervical lymphadenitis. Mycobacterium tuberculosis can affect multiple sites in the head and neck (ie, the cervical lymph nodes, larynx, pharynx, oral cavity, nasal cavity, salivary glands, cervical spine, middle ear, and the mastoid). Cervical lymphadenopathy, the most common manifestation of this disease in the head and neck, affected 5%–10% of all patients with tuberculosis.21 Over the last 10 years, we obtained histopathologic diagnosis of cervical tuberculous lymphadenitis in more than 100 patients by sonographically guided biopsy performed at our hospital. In one of our cases, a 5-year-old male patient complained of left otorrhea and ipsilateral cervical lymphadenopathy. Neck CT showed multiple calcified enlarged lymph nodes in the left jugulodigastric chain, posterior triangle, and skull base. The tuberculous lymphadenopathy was diagnosed by tissue biopsy.
We believe that TOM in uncomplicated cases should be treated with antituberculous drugs. Surgery is indicated for complicated cases, such as those involving subperiosteal abscess of the mastoid, facial palsy, postauricular fistulas, or CNS extension of infection.12–14 Saunder et al9 also suggested that failure to respond to drug therapy even in the absence of demonstrable complications should be added to the list of indications for surgical intervention. We believe that most surgeries were done to obtain histologic material for diagnosis. Middle ear mucosal biopsy can be performed for histologic diagnosis through the perforated tympanic membrane.
Conclusion
Although specific findings of TOM in HRCT of temporal bone may not exist, the soft tissue in the entire middle ear cavity, preservation of mastoid air cells without sclerotic change, mucosal thickening of the bony EAC, or a soft tissue extension to the EAC without erosion of scutum seemed to be characteristic CT findings and would be helpful for the early diagnosis of TOM.
References
- Received February 7, 2006.
- Accepted after revision May 15, 2006.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}