
Abstract
PURPOSE: The authors report their experience using HydroCoils in the treatment of cerebral aneurysms.
METHODS: We performed a retrospective review of the first 100 nonrandomized patients (104 coiled saccular cerebral aneurysms) treated with HydroCoils during a 27-month period.
RESULTS: The average percentage of HydroCoil by length detached in treated aneurysms was 45.5% (range, 9.9–100%). Immediate postprocedure angiography demonstrated complete aneurysm occlusion in 34%, neck remnant in 35%, and incomplete occlusion in 32%. Immediate procedure-related morbidity and mortality rates were 5.8% and 0%, respectively. Angiographic follow-up was obtained in 51% (51/100 patients; 53/104 aneurysms; average, 10.3 months; range, 0–31 months). In these 53 angiographically followed aneurysms, the overall recanalization rate was 21%: no recanalization occurred in 23 aneurysms with small size (<10 mm)/small neck (<4 mm) (S/S); 4 recanalizations occurred in 7 aneurysms with small size/wide neck (>4 mm) (S/W); 6 recanalizations (27%) occurred in 22 large (L) aneurysms (>10–25 mm, 70% angiographic follow-up); and 1 giant (G) (>25 mm) aneurysm recanalized. A large proportion of aneurysms that were not initially completely occluded were completely occluded on follow-up (15/43 [35%]). Clinical follow-up was obtained in 73 patients (73%; average, 5.3 months; range, 0–24 months): 93% of these patients were neurologically improved or unchanged. Three patients rehemorrhaged and 3 patients with unruptured aneurysms developed delayed hydrocephalus.
CONCLUSIONS: The overall safety profile of HydroCoils appears acceptable. Preliminary midterm observations suggest less coil compaction/aneurysm recanalization in large aneurysms. However, HydroCoil-related delayed hydrocephalus is a concern.
From its clinical introduction in 1991 in nonsurgical patients with ruptured cerebral aneurysms, the Guglielmi detachable coil (GDC; Boston Scientific Neurovascular, Natick, Mass) and other bare platinum coils have been increasingly used in patients worldwide to occlude ruptured and unruptured cerebral aneurysms.1–8 The short-term clinical results of endovascular treatment of cerebral aneurysms with platinum coils continue to improve and are comparable to those of microsurgical clipping.1,6,8–10 In particular, aneurysm occlusion with detachable inert bare platinum coils has been shown to decrease the risk of rebleeding during the acute phase and at 1-year follow-up with acceptable procedural risk.1,4–6,8,10 However, the long-term permanence of coil occlusion and relative effectiveness of aneurysm coiling in preventing delayed rehemorrhage are still in question.8,11
Despite advances in platinum coil technology11,12 and in coiling techniques,13 important limitations of coiling with bare platinum coils persist.11 In cerebral aneurysms that are wide-necked or >10 mm, complete aneurysm occlusion with bare platinum coils is achieved in <50% of patients.1,8,11 When aneurysms are not completely occluded, the risk of coil compaction and aneurysm recanalization is significant, estimated at 5%, 20%, 35%, and 60% overall for small (<10 mm) narrow-necked (<4 mm) (S/S), small wide-necked (>4 mm) (S/W), large (>10–25 mm) (L), and giant (>25 mm) (G) aneurysms, respectively.11 Given this persistent shortcoming of bare platinum coils, we believe that a new coil that resists coil compaction and decreases the risk of aneurysm recanalization would be a major advance in the treatment of cerebral aneurysms.
The HydroCoil (Microvention, Aliso Viejo, Calif) is a hybrid hydrogel polymer/platinum coil that has the property of volumetric swelling with time (maximal volume achieved in approximately in 20 minutes) (Fig 1). The rationale for its use and development is that increased volumetric filling with hydrogel leads to more densely packed aneurysms and results in less coil compaction and aneurysm recanalization. In a recent study of HydroCoils in a canine bifurcation large aneurysm model, HydroCoils compacted less than bare platinum coils.14

HydroCoil after hydrogel (translucent) coating has fully expanded around a platinum core.
This study describes the early anatomic and clinical outcomes of the first 100 patients with intracranial saccular aneurysms treated with HydroCoils at our institution. We investigated the safety profile of HydroCoils and whether it was associated with less coil compaction/aneurysm recanalization.
Patients and Techniques
Patient Selection
Between November 2002 and February 2005, 277 patients with cerebral aneurysms were treated with endovascular coil embolization at the Beth Israel Hyman-Newman Institute for Neurology and Neurosurgery in New York. During this period, the first consecutive 100 patients in whom HydroCoils were detached in 104 intradural saccular cerebral aneurysms were identified. Patients with HydroCoil and treated extradural cavernous aneurysms, fusiform aneurysms, and distal aneurysms treated primarily with parent artery sacrifice were excluded. Most patients were referred from neurologic and neurosurgical centers for aneurysms or were believed to have a higher risk for surgical treatment, after failed surgical attempt, after prior evaluation by both endovascular surgery and vascular microsurgery teams recommended coiling, or because of patient refusal of surgery.
There were no strict inclusion criteria. On the basis of operator preference, the coiling procedure was augmented with HydroCoil filling coils in selected cases. In general, the tendency of the operators was to treat larger aneurysms with HydroCoils, with the rationale of decreasing the total number of coils used. Review of records could not accurately nor reliably identify patients in whom HydroCoil placement was attempted but not deployed; therefore, the exact number of patients with failed HydroCoil deployments was not recorded. The anatomic and clinical outcomes of this cohort of 100 patients with 104 HydroCoil-treated cerebral saccular aneurysms were retrospectively studied. The patient clinical and aneurysm data are summarized in Table 1. Aneurysms were divided into 4 categories11: S/S, S/W, L, and G aneurysms.
Patient and aneurysm characteristics
Endovascular Treatment
The technique for endovascular coil treatment has been previously described.11,15 Eighty-seven patients were treated on a biplane angiographic system (Siemens, Erlangen, Germany) with 3D-rotational digital subtraction angiography; 13 patients were treated on a single-plane angiographic system without 3D-rotational angiography (Philips Medical Systems, Best, the Netherlands). In general, intravenous heparin infusion was continued for 24–48 hours after the procedure, with maintenance pulse transit time goal of 50 seconds. HydroCoil size and length selection were based on operator preference, and preparation was performed as specified by the manufacturer. HydroCoils were used primarily as filling coils in this series. GDC bare platinum coils were used almost exclusively initially to frame the aneurysm. Balloon-remodeling technique was used in 21 (20%) procedures.13 Stent-assisted coiling was performed in 8 (8%) procedures.16,17
Complications
Procedure-related morbidity was recorded as a permanent new neurologic deficit after embolization. Procedure-related death was recorded as death directly related to procedure (eg, intraoperative rupture or procedure-related morbidity leading to death). Delayed rehemorrhage of treated aneurysm was recorded. Clinical follow-up data were collected by review of hospital charts, evaluation at last clinic visitation or follow-up angiography, or by telephone interview. Patients’ neurologic outcome at last evaluation was recorded as unchanged, improved, or worse, compared with pretreatment status.11
Angiographic Evaluation
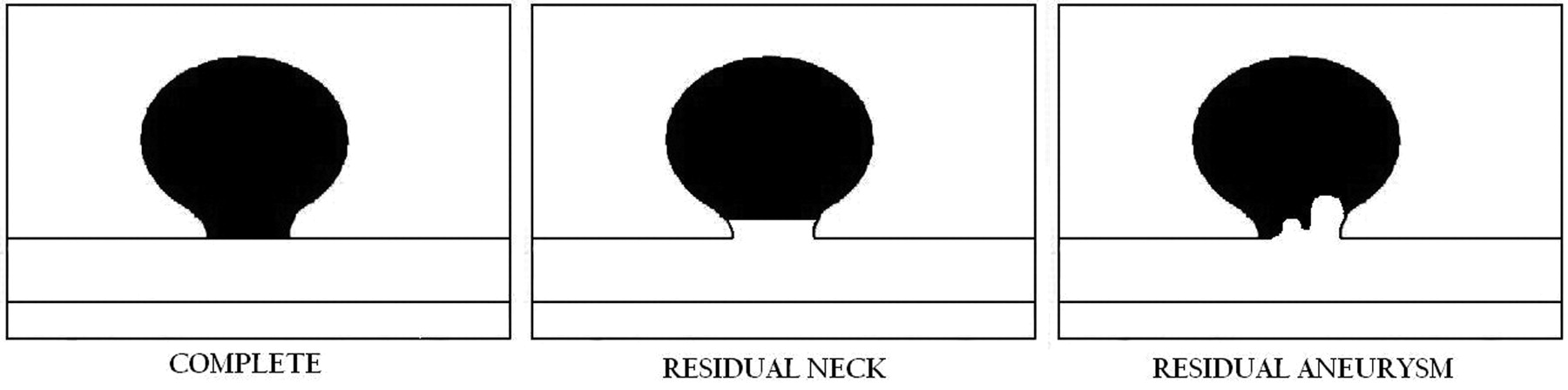
Angiographic results were recorded immediately and on last follow-up. Multiple projections with selective contrast injections were reviewed for angiographic complete occlusion, defined as no contrast within the aneurysm dome, body, and neck. We used the classification of angiographic results as defined by Roy et al7: class 1, complete occlusion; class 2, persistence of any portion of the original defect of the arterial wall as seen on any single projection but without opacification of the aneurysm sac; class 3, aneurysm sac opacification (Figs 2 and 3). For each patient, the pre- and postembolization and follow-up (if available) angiograms were independently reviewed by 2 attending interventionalists for initial and follow-up aneurysm occlusion grades. The interventionalists were blinded as to the type and percentage length of the HydroCoil used for each patient. Written reports were not reviewed for aneurysm occlusion grade determination. For discordant grades, the worse of the 2 occlusion grades was recorded.

Diagrams of angiographic occlusion classes, adapted from Roy et al7: class 1, complete; class 2, residual neck; and class 3, aneurysm filling.

Example of angiographic occlusion classes 1, 2, and 3: class 1, complete occlusion; class 2, persistence of any portion of the original defect of the arterial wall as seen on any single projection but without opacification of the aneurysm sac; and class 3, aneurysm sac opacification.
Angiographic Follow-Up Strategy and Evaluation
For patients with all treated aneurysms, follow-up skull x-rays were requested at 3 months. If skull x-rays showed evidence of coil compaction, angiography was recommended immediately. Compared with the postembolization unsubtracted coil mass, visual recognition of a change in coil mass configuration on skull x-rays, either flattening, rotation, loosening, reorientation, and so forth, indicated coil compaction.18 Otherwise, for patients with ruptured aneurysms, a 6-month follow-up angiogram was recommended. For patients with unruptured aneurysms, a 1-year follow-up angiogram was recommended. Angiograms were also recommended at 3-year and at 5-year follow-up.
To better compare recanalization results with GDC bare platinum coils, we used the same definition of recanalization as that used in the 11-year UCLA experience11: Recanalization was defined as more than 10% increase in contrast filling of the aneurysm; less than 10% increased filling was defined as unchanged. Also for this follow-up group, class (1, 2, or 3) angiographic results were compared immediately after embolization and at last follow-up.
Results
Patient Population
Table 1 summarizes patient and aneurysm characteristics. Sixty percent of patients were women. The mean age was 54 years. Fifty-four percent of the treated aneurysms were unruptured. Three fourths of the treated aneurysms were located in the anterior circulation. S/S aneurysms composed 40%; S/W, 26%; L, 32%; and G, 3%.
Clinical Outcome
Table 2 summarizes procedural complications. Procedure-related morbidity was 5.8% and procedure-related death was 0%. One aneurysm perforation (<1%) occurred (first bare platinum coil framing coil; HydroCoil used to seal re-ruptured site) and led to permanent neurologic deficit in a surviving patient.
Procedural complications
Thromboembolism occurred in 9 procedures, leading to 3 permanent neurologic deficits. In a 65-year-old man, a ruptured anterior communicating artery aneurysm was coiled with 20% HydroCoil by length; after the coiling procedure, thromboembolism of the left frontal and parietal cortical branches occurred and was treated with intra-arterial thrombolysis, with improved perfusion to the parietal middle cerebral artery (MCA) branches but not in the left prefrontal MCA territory, leading to a permanent language deficit. In a 22-year-old woman with a ruptured basilar trunk aneurysm, intraoperative aneurysm rupture occurred during placement of the first bare platinum coil. Heparin was reversed. A single HydroCoil was used to seal the aneurysm rupture site, but 1 of the coil loops protruded into the parent vessel. An emergent ventriculostomy catheter was then placed in the angiography suite. After ventriculostomy placement, a control angiogram showed thrombus about the coil loop, which was treated with 2 mg of intra-arterial abciximab (ReoPro). Follow-up MR imaging with diffusion imaging showed no infarct; however, the patient did not recover from the rehemorrhage and was eventually discharged to a skilled nursing facility, not cognitively able to participate in her care.
In the third patient, a 67-year-old woman with a ruptured large right posterior communicating artery aneurysm, 22% HydroCoil by length was used; the last coil, a bare platinum coil, stretched and was eventually removed without movement of the coil mass. On the postembolization control angiogram, a distal right inferior parietal branch occlusion was present. The patient was treated with intravenous heparin for 48 hours but had a mild sensory deficit. Parent artery occlusion occurred in 1 procedure, but this did not lead to a new neurologic deficit. Follow-up angiography performed 3 days later showed complete recanalization of the occluded artery.
Clinical follow-up was obtained in 73 patients from <1 month to 24 months; average, 5.3 months. Of these 73 patients, 68 (93%) had improved or unchanged neurologic status at last follow-up. Thirty-two patients had improved neurologic status, 36 patients had unchanged neurologic status, and 5 patients had worse neurologic status. Three patients experienced rehemorrhage after coiling (Table 3). Of the patients who rebled, 2 died. Three patients who did not have aneurysm rupture developed symptomatic hydrocephalus requiring ventriculoperitoneal shunt surgery, with recovery in all 3 (Table 4).
Characteristics of 3 ruptured aneurysm patients who rehemorrhaged
Characteristics of 3 unruptured aneurysm patients who developed delayed hydrocephalus with symptoms of confusion and gait disturbance
Immediate Angiographic Outcome
Immediate postprocedure angiography demonstrated overall class 1 complete aneurysm occlusion in 35 (34%), class 2 neck remnant in 36 (35%), and class 3 incomplete occlusion in 33 (32%). Table 5 summarizes class 1, 2, and 3 angiographic results for S/S, S/W, L, and G aneurysms. In general, more complete closure was seen in S/S aneurysms. On average, HydroCoils composed 45.5% by total length of detached coils within treated aneurysms.
Immediate angiographic occlusion classification
Follow-Up Angiographic Outcome
Follow-up angiography was performed in 51 patients with 53 HydroCoil-treated aneurysms. Table 6 lists the clinical and aneurysm characteristics of this group of patients. Angiographic follow-up was obtained from 0 to 31 months; average, 10.3 months. Forty-two of the 51 patients (82%) had >6 month follow-up. In this angiographically followed group, 1 aneurysm was G; 22 (46%) were L; 7 were (13%) S/W; and 23 were (43%) S/S. On the basis of the initial size distribution of treated aneurysms, angiographic follow-up was obtained in 55% (23/42) of S/S aneurysms, 26% (7/27) of S/W aneurysms, 69% (22/32) of L aneurysms, and 33% (1/3) of G aneurysms. In this angiographically followed group, compared with all patients, the percentage by length of HydroCoils was similar, 51% versus 46%.
Clinical and aneurysm characteristics of 51 patients with 53 aneurysms with angiographic follow-up
Comparison of occlusion class immediately after treatment and at last follow-up showed that 87% of the 53 aneurysms had stable or improved class and 13% had worse class (Table 7). Of the 43 class 2 and class 3 aneurysms, on follow-up, 15 (35%) aneurysms were class 1, completely occluded (Fig 4). Of note, 12/20 (60%) class 3 aneurysms converted to class 1 on last follow-up.

Example of class 3 conversion to class 1. Left accessory MCA aneurysm shows aneurysm filling (class 3) in immediate postembolization angiogram. Ten-month follow-up angiogram shows class 1 complete occlusion.
Angiographic occlusion classification: aneurysm comparison between immediate and last angiographic follow-up
Aneurysm Recanalization
In these 53 angiographically followed aneurysms, overall recanalization rate was 21% (Table 8). No recanalization occurred in 23 S/S aneurysms. Four recanalizations occurred in 7 S/W aneurysms. Recanalization occurred in 6/22 (27%) L aneurysms. One G aneurysm recanalized.
Recanalization rates
Discussion
The overall safety profile of HydroCoils appears acceptable. In our series, the incidence of thromboembolic complication was slightly higher than our experience with bare platinum coils, and most occurred earlier in our experience. This finding may be due to the larger expanded size of HydroCoils rather than any intrinsic thrombogenic propensity of the coil material. The incidence of thromboembolic complication is probably less if the finishing coils are bare platinum coils; use of these coils was our tendency later in our experience. However, using soft platinum finishing coils may increase the risk of coil compaction. Clot at the coil–parent artery interface can usually be successively treated with intra-arterial and/or intravenous platelet glycoprotein IIb/IIIa receptor inhibitors such as ReoPro,19 even in acute subarachnoid hemorrhage but after the aneurysm has been secured. In patients with unruptured aneurysms, antiplatelet agents may be considered to decrease the risk of thromboembolism.
Three patients rehemorrhaged. In 1 patient, a large basilar apex/P1 posterior cerebral artery aneurysm with pseudoaneurysm was incompletely treated (class 3), and this aneurysm rebled within 24 hours of treatment. In 1 patient, a large anterior communicating aneurysm was treated (class 2), despite gram-negative ventriculitis and brain abscess; this patient rebled 4 months after treatment. In the third patient, a neonate, only 1 HydroCoil could be placed among other platinum coils into a large dysplastic aneurysm, which was not completely occluded (class 3); this aneurysm rebled 2 months later.20
The development of hydrocephalus in 3 patients with unruptured aneurysms is concerning and warrants investigation. CSF analysis in 2 patients was consistent with an aseptic nonspecific inflammatory process. All 3 patients had large aneurysms in which a high percentage of HydroCoils was used. Early in our experience, we steamed HydroCoils to induce memory and a tighter coiling profile before advancement into the microcatheter. The contributory role of this practice is unknown. All 3 patients returned to their neurologic baseline after shunt surgery. Steroids administered in the peri- and postprocedure period may decrease this inflammatory risk.21
Given the limitations of our study including selection bias and its nonrandomized and uncontrolled retrospective nature, when we compared results to different studies, the significance of any differences is unknown. With that caveat, observationally in our study, in L and S/S aneurysms, HydroCoils seemed to lead to less coil compaction and aneurysm recanalization than that reported for bare platinum coils.8,11,22 With almost 70% angiographic follow-up for HydroCoil-treated L aneurysms, the recanalization rate of 27% (6/22) appears to be an improvement over that reported for GDC-treated L aneurysms.11 For S/S aneurysms, 0% (0/23) recanalization was found with 55% follow-up. In contrast, for S/W aneurysms, HydroCoils did not appear to reduce recanalization, but only 26% (7/27) follow-up was obtained in this group. Of the recanalized aneurysms, 3 were partially thrombosed at the time of treatment; 1 aneurysm was treated in a patient with gram-negative ventriculitis; and in 1 large aneurysm, only 1 HydroCoil was used. The average percentage length of HydroCoil in the recanalized cases was 42%.
Although the significance of any similarities or differences is not known between the 2 retrospective studies, in our series based on 51% angiographic follow-up, the overall midterm recanalization rate was 21%, which is similar to that reported for GDC.11 Vinuela et al1, recently reported recanalization rates (similarly defined) of their 11-year pioneering experience with GDC therapy for cerebral aneurysms.11 In this series, 53.4% of GDC-treated aneurysms had angiographic follow-up (average 11 months), which revealed an overall recanalization rate of 21%, with 5.1% for S/S, 20% for S/W, 35.3% for L, and 59.1% for G aneurysms, respectively. With similar percentages of angiographically followed aneurysms (51% versus 54%) and similar follow-up periods (10.3 versus 11 months), as in our experience, Vinuela et al also reported that in their experience, most aneurysm recanalizations occurred within 3 months.1,11
This concept of early coil compaction is supported by our canine high-flow bifurcation wide-neck aneurysm model, in which coil compaction was seen at 2 weeks and progressed at 3 months.14 However, in a longer-term retrospective analysis of angiographic recurrences in aneurysms treated with bare platinum coils, Raymond et al23 found that a significant percentage of aneurysms recanalized beyond 6 months. They reported that only 47% of all recurrences had been detected by 6 months, but by 36 months, 97% of all recurrences were detected.23 Their recurrences were associated with treatment after aneurysm rupture; large size, >10 mm; and class 3, incomplete occlusions.23 This discrepancy may be secondary to some extent to measurement bias, with differences in timing, technique, and compliance of follow-up protocol.
Of particular interest is the natural history of a neck remnant in the UCLA GDC experience.22 In 73 coiled aneurysms with neck remnants that had angiographic follow-up (mean, 17.3 months), recanalization rates were remarkably high: 17%, 42%, 87%, and 90% for S/S, S/W, L, and G aneurysms, respectively.22 This is contrasted to our 10 large aneurysms with residual neck (class 2), of which only 30% recanalized. Of note, 2 of these recanalized aneurysms were partially thrombosed at the time of treatment, and 1 was treated in the setting of gram-negative ventriculitis.
Thirty-five percent (15/43) of aneurysms that were not completely occluded (classes 2 and 3) were found to be completely occluded (converted to class 1) on angiographic follow-up (Fig 4). Conversion from class 3 to class 1 is not typical for GDC coiled aneurysms.7,11 Twelve of 20 (60%) of class 3 aneurysms converted to class 1 aneurysms, even in large aneurysms. This change supports the concept that volume-packing plays an important role in recanalization. Despite attenuated packing with the GDC system, the total percentage of volume that GDC or similar bare platinum coils occupy in a treated aneurysm is usually <30%.24 Tamatani et al24 reported that the mean embolized coil volume of angiographically stable aneurysms was 30.8 ± 10.2% and that of recanalized aneurysms was 19.9 ± 10.6% (P = .03). With HydroCoils, volume-attenuation packing can reach >70%.14
In our series, the immediate postembolization complete occlusion rate (class 1) was 35%; residual neck (class 2), 35%; and aneurysm filling (class 3), 30%. Our complete occlusion rate was less than previously reported (average, 54%).1,7,8 This discrepancy, in part, can be explained by the subjective nature of reporting results. Unfortunately, no standardization has been widely adopted. In our analysis, we have adhered to strict criteria for complete occlusion. The relatively high rate of aneurysm filling immediately after embolization can also be explained in part by operator preference. With bare platinum coils, attenuated packing is the goal. However, in our opinion, the last coil to achieve attenuated packing is often the most complication-prone.
One subjective advantage of HydroCoils is that the last coil decision becomes less of an issue. Because of the property of HydroCoils of delayed and increasing volumetric expansion, to achieve a comparable degree of coil packing, one needs relatively fewer and shorter lengths of HydroCoils. Therefore, relative underpacking with HydroCoil can ultimately lead to the same or greater volumetric packing than what is expected with GDC bare platinum coils, but this may not be seen on immediate postembolization angiography. For HydroCoil, 30-minute delayed postembolization angiography would be more accurate in assessing immediate angiographic occlusion. A 30-minute delayed angiogram was not obtained routinely in our series.
One of the limitations of HydroCoil is its relatively decreased effectiveness in partially thrombosed aneurysms. The effectiveness of bare platinum coils is also poor in these aneurysms, particularly in G aneurysms.11 In partially thrombosed aneurysms, if coil compaction/migration and aneurysm recanalization occur despite the use of HydroCoils, additional considerations such as stents,16,17 liquid embolic agent,25 microsurgical clipping, and if G, parent artery sacrifice with or without bypass should be considered.
In addition to the nonrandom uncontrolled retrospective method of the study, further limitations of our study include the small number of patients and treated aneurysms and the relatively low percentage and short duration of angiographic and, to a less degree, clinical follow-up. As a tertiary center and with a larger number of referrals from local, national, and international sources, return visits for clinical and angiographic follow-up could not be uniformly achieved despite requests. We continue to collect angiographic and clinic follow-up data for this cohort of patients. The first framing coils provide mechanical support to allow denser packing and provide a barrier to prevent hydrogel expansion into the parent vessel lumen. The contribution of bare platinum framing and finishing coils is uncertain.
Conclusions
The overall safety profile of HydroCoils appears acceptable. HydroCoil may be a higher risk/higher reward coil. Preliminary midterm observations suggest less coil compaction/aneurysm recanalization in L aneurysms treated with HydroCoil than that reported for bare platinum coils. However, longer and more complete follow-up is necessary for validation. HydroCoil-related delayed hydrocephalus is a concern. The long-term efficacy of HydroCoils is unknown.
Acknowledgments
We thank Angel Arce for film, Anthony Tanzola for data base/computer, and Peter Rappa for administrative assistance during the conduction of the study.
Footnotes
Dr. Berenstein has consulting and/or financial interests in MicroVention and Boston Scientific-Target Therapeutics.
References
- Received October 18, 2005.
- Accepted after revision January 20, 2006.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Optimal first coil selection to avoid aneurysmal recanalization in endovascular intracranial aneurysmal coiling
- Treatment of experimental aneurysms with a new liquid embolic agent and a retrievable stent: proof of concept and feasibility study
- HydroCoils Reduce Recurrence Rates in Recently Ruptured Medium-Sized Intracranial Aneurysms: A Subgroup Analysis of the HELPS Trial
- Reactive tissue proliferation and damage of elastic lamina caused by hydrogel coated coils in experimental rat aneurysms
- Coil Type Does Not Affect Angiographic Follow-Up Outcomes of Cerebral Aneurysm Coiling: A Systematic Review and Meta-Analysis
- Effect of Core Laboratory and Multiple-Reader Interpretation of Angiographic Images on Follow-Up Outcomes of Coiled Cerebral Aneurysms: A Systematic Review and Meta-Analysis
- A multicenter registry of hydrocephalus following coil embolization of unruptured aneurysms: which patients are at risk and why it occurs
- The next generation HydroCoil: initial clinical experience with the HydroFill embolic coil
- Perioperative safety of Hydrosoft coils
- Delayed Hydrocephalus after Embolization of Unruptured Aneurysms Using Bare Platinum Coils: Report of 2 Cases
- Embolization of Intracranial Aneurysms with HydroSoft Coils: Results of the Korean Multicenter Study
- HydroCoils, Occlusion Rates, and Outcomes: A Large Single-Center Study
- Relative cost comparison of embolic materials used for treatment of wide-necked intracranial aneurysms
- Angiographic and Clinical Outcomes in 200 Consecutive Patients with Cerebral Aneurysm Treated with Hydrogel-Coated Coils
- Endovascular Coiling of Cerebral Aneurysms Using "Bioactive" or Coated-Coil Technologies: A Systematic Review of the Literature
- Intradural Saccular Aneurysms Treated by Guglielmi Detachable Bare Coils at a Single Institution Between 1993 and 2005: Clinical Long-Term Follow-Up for a Total of 1810 Patient-Years in Relation to Morphological Treatment Results
- Treatment of Brain Aneurysms
- Predictors of Rehemorrhage After Treatment of Ruptured Intracranial Aneurysms: The Cerebral Aneurysm Rerupture After Treatment (CARAT) Study