
Abstract
SUMMARY: We report 2 cases of nasolabial cyst and a case of schwannoma beneath the alar base that required a differential diagnosis because of clinical features and MR images that resembled the nasolabial cyst. The morphologic analysis on MR images revealed the characteristic appearance of the nasolabial cyst, and the sagittal MR image may be most helpful for diagnosing this rare disease.
Nasolabial cyst or nasoalveolar cyst (NC) presents as a well-circumscribed soft mass beneath the alar base and often causes the elevation of the ala nasi and protrusion of the anterior nasal base. This lesion is quite rare but is also well known because of its characteristic clinical appearance and pathogenesis.1–6 Some reports1,2,7 emphasize the importance of differential diagnosis of NC to distinguish it from other diseases that occur near the ala nasi, such as inflammatory conditions following dental and soft-tissue neoplastic diseases. Because NC is a soft-tissue mass, MR imaging is most helpful for a differential diagnosis. However, few cases have been reported1,8 with detailed MR imaging findings, and little attention has been paid to the presentation of these diseases that show clinical features resembling NC.
Schwannoma is a relatively rare disease in the facial region, and its occurrence in the upper lip is considered to be very unusual.9,10 This lesion presents as a solitary, movable, and elastic-soft subcutaneous spheric mass. MR images of this lesion are not specific11 and are similar to those of NC. It is easy to confuse these features of schwannoma with those of NC, when the schwannoma occurs beneath the ala nasi.
In this report, we describe 2 cases of NC and 1 case of schwannoma located beneath the alar base and discuss the detailed 3D morphologic differences on MR images.
Case Reports
Case 1
A 47-year-old Japanese woman was referred to our department in September 2002 with painless swelling at the left alar base. She had noticed slight swelling in this area since 1989. Because of a sudden increase in the swelling in 2000, she underwent aspiration of the contents in an ear, nose, and throat clinic. After this treatment, she did not feel the presence of the lesion, but she noticed a gradual increase in swelling again in August 2002. Clinical examination revealed the presence of an elastic-soft mass beneath the left alar base. The lesion continued along the labial vestibule from the left central incisor to the canine. The nasal vestibule was protruded and asymmetric because of the swelling of the left alar base. Conventional radiography did not show any significant change in the bone. MR imaging revealed the presence of a well-defined soft-tissue mass, with homogeneous hypointensity on T1-weighted images and hyperintensity on T2-weighted images. In the posterior portion of the lesion, a slight hyperintensity area on T1-weighted and a hypointensity area on T2-weighted images were observed; this finding was expected to show the presence of fluid (Fig 1A, -B). On the coronal view of the MR images, the lesion was located mainly in the upper lip and did not expand toward the nasal side but instead expanded toward the lateral side (Fig 1C).

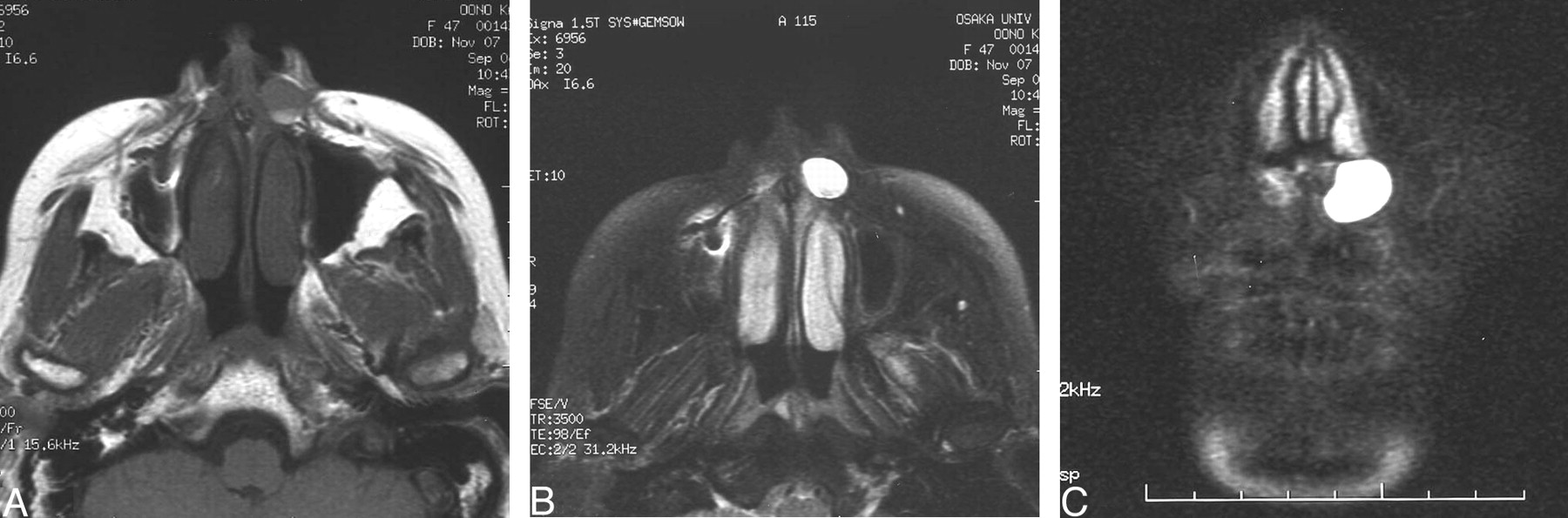
Nasolabial cyst (case 1).
A, The axial T1-weighted image shows the lesion beneath the left alar base with a well-circumscribed homogeneous isointensity containing a sedimentation level.
B, The axial T2-weighted image shows the homogeneous hyperintensive lesion, in which the sedimentation level is also observed.
C, The coronal T2-weighted image shows a bean-shaped homogeneous hyperintensive lesion, which does not expand toward the nasal side but instead expands toward the lateral side.
Extirpation was performed with local anesthetic by an intraoral approach. The lesion was easily removed from the surrounding soft tissue, except from the nasal mucosa because of adhesions. The lesion contained brown mucous fluid. Histopathologic examinations revealed the cyst wall lined by pseudostratified columnar epithelium with scattered goblet cells and cilia, and this lesion was diagnosed as NC. The postoperative course was uneventful.
Case 2
A 54-year-old Japanese woman was referred to our clinic with a swelling beneath the left alar base in February 2005. She noticed the swelling and was referred to an ear, nose, and throat clinic in November 2004. The tumor was suspected to be of odontogenic origin, and she visited a dental clinic. However, because of lack of the clear evidence of the odontogenic origin, she was referred to our clinic. The clinical examinations revealed the presence of a painless soft mass beneath the left alar base and the protrusion of the anterior nasal vestibule. Conventional radiographs showed the central and lateral incisors, with root canal filling but no radiolucent lesion. MR imaging revealed a well-defined soft-tissue mass, with homogeneous isointensity on T1-weighted and hyperintensity on T2-weighted images (Fig 2A, -B). The coronal view revealed the expansion of the lesion toward the nasal side along the lateral wall of the nasal cavity (Fig 2C), and on the sagittal view, this lesion also expanded toward the posterior of the nasal cavity beyond the anterior edge of the nasal base of the maxillary bone (Fig 2D). The lesion, containing yellowish viscous fluid, was extirpated via an intraoral approach using local anesthetic. The histopathologic diagnosis was NC, with the finding of cyst wall–lined pseudostratified columnar epithelium with abundant goblet cells. The postoperative course was uneventful.

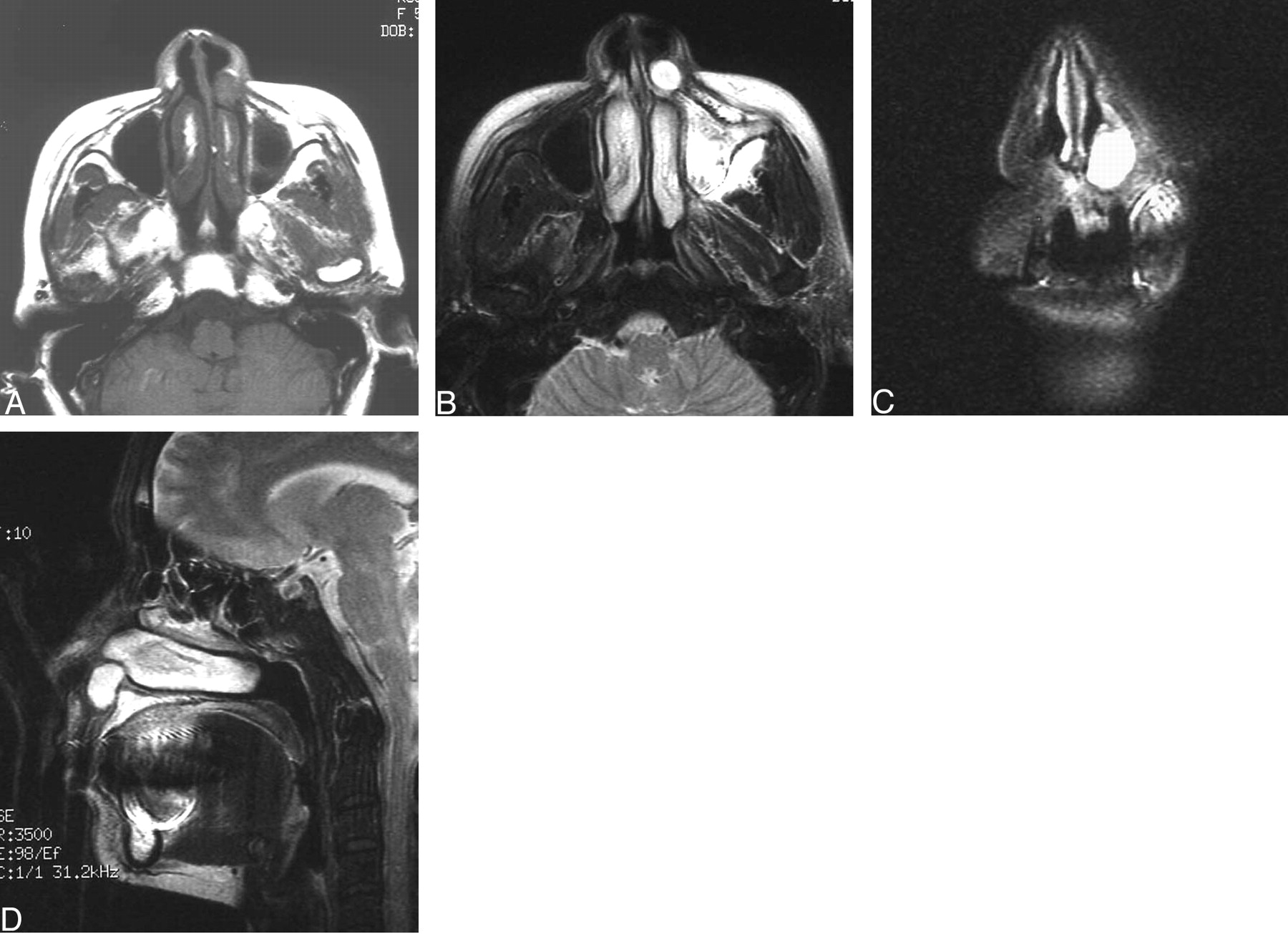
Nasolabial cyst (case 2).
A, The axial T1-weighted image shows the well-circumscribed lesion with a homogeneous isointensity in the anterior nasal fold.
B, The axial T2-weighted image shows the well-circumscribed lesion with a homogeneous hyperintensity.
C, The coronal T2-weighted MR image shows the lesion extending toward the nasal cavity along the lateral nasal wall.
D, The sagittal T2-weighted MR image shows the expansion of the lesion toward the posterior of the nasal cavity, and the lesion appears as a bean shape because of the anterior edge of the nasal base of the maxillary bone.
Case 3
A 16-year-old Japanese boy was referred to our clinic with a mass beneath the right alar base in April 2005. He had a left cleft lip and palate and had undergone several surgical corrections for this condition in our department since childhood. He noticed the presence of the painless mass on October 2004, and the mass gradually grew. Clinical examination revealed a painless, movable, rounded, and elastic-soft mass of 15 × 10 mm beneath the right alar base. The protrusion of the alar base was not remarkable. MR imaging revealed the presence of a rounded well-defined soft-tissue mass, with homogeneous hypointensity on T1-weighted images and hyperintensity on T2-weighted images (Fig 3A, -B).

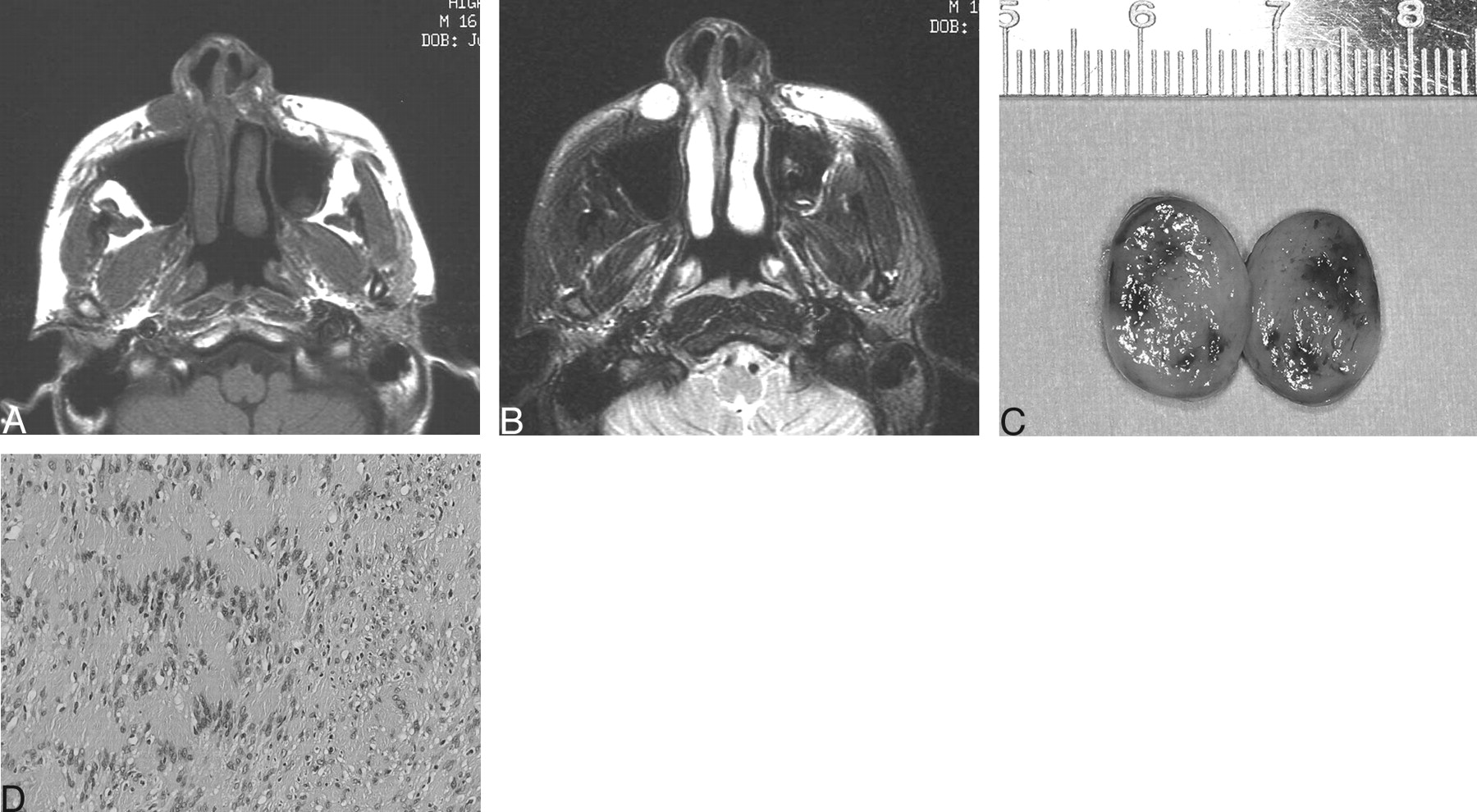
Schwannoma (case 3).
A, The axial T1-weighted image shows the rounded well-circumscribed lesion beneath the right alar base.
B, The axial T2-weighted images reveals the presence of a homogeneous well-circumscribed rounded lesion beneath the right alar base. The lesion is not attached to the nasal structures.
C, The excised specimen shows that the tumor consists of a yellowish jellylike mass encapsulated by thin fibrous tissue.
D, Histopathologically, the tumor is composed of proliferating spindle-shaped cells showing a palisaded arrangement and diagnosed as schwannoma Antoni A type (hematoxylin-eosin, original magnification ×20).
Extirpation was performed via an intraoral approach using local anesthetic. The tumor consisted of a yellowish jellylike tissue encapsulated by thin fibrous tissue (Fig 3C). Histopathologically, the tumor was composed of proliferating spindle-shaped cells showing a palisaded arrangement and was diagnosed as schwannoma Antoni A type (Fig 3D). The postoperative course was uneventful.
Discussion
Schwannoma is a benign neoplasm originating from schwann cells of the nerve sheath. This lesion is rather common in the head and neck region9,11 but is rare in the upper lip,9 and only 7 cases have been reported in the English-language literature.9,10 Histopathologically, the cells are arranged in both a cellular palisaded pattern (Antoni A) and a loose poorly cellular pattern (Antoni B). The lesion clinically appears as a movable soft mass, often painful but generally asymptomatic. On CT, the lesion appears as a well-circumscribed attenuated homogeneous soft-tissue mass that exhibits contrast enhancement. MR images are isointense or hypointense relative to muscle on T1-weighted and hyperintense on T2-weighted images,10,11 with strong enhancement after contrast administration.11
On the other hand, NC is a well-known non-odontogenic cyst that occurs in the alar base and has a predilection for women,2,12–14 especially those older than 40 years.12,14 It often appears bilaterally and shows rather uniform clinical features. It is located beneath the ala nasi and anterior nasal fold and appears as a painless, mobile, elastic-soft, and fluctuating mass with defined margins and causes the protrusion of the upper lip, an elevated nasal alar, and the effacement of the nasolabial fold. This lesion is usually noted for several years because of its slow growth but develops a painful swelling when infection occurs.
The pathogenesis of this cyst is still controversial. One early theory was that the lesion was a retention cyst arising from an inflamed mucous gland.5 Recent theory, suggested by Klestadt,4 was that embryogenic nasal epithelium was trapped between the merging maxillary process and the medial and lateral nasal process. His hypothesis was well supported,2,14 and NC was categorized as a fissural cyst in the classification of the World Health Organization (WHO) in 1971,15 which also included a globulomaxillary cyst. The reliability of this hypothesis has, however, decreased because of the lack of evidence for embryonic epithelial entrapment in this region.13,16 The hypothesis advocated by Brüggeman,6 that this cyst forms from the anlage of the nasolacrimal duct, is now well supported because of the similarity of histopathologic findings, among them that both tissues have walls lined by pseudostratified columnar epithelium.13,16 The new classification by the WHO in 1991 has accepted this pathogenesis.17 However, Lopez-Rios et al,3 who showed a case with extensive apocrine changes, suggested a review of this theory because of the lack of evidence for apocrine cells in nasolacrimal ducts. Discussions will continue.
Because the NC appears as a soft-tissue mass, CT and MR imaging examinations are helpful to confirm its location. Recently, some reports1,8 presented detailed MR images of this lesion and showed that the appearance of NC on MR imaging is homogeneous hypointensity to intermediate intensity on T1-weighted images and hyperintensity on T2-weighted images. However, the images of postenhancement are also different among reports. Tanimoto et al8 indicated that the enhancement was observed at the periphery, but Curé et al1 showed that postcontrast T1-weighted images revealed no enhancement of contents or of the wall of the cyst.
Curé et al1 also presented a case showing the sedimentation level of the contents of the cyst, which appeared with mild hyperintensity on T1-weighted images and mild hypointensity on T2-weighted images, suggesting milk of calcium. This finding is in agreement with the MR imaging finding of our case 1 but was not observed in case 2. In the former case, the contents were a brown mucous fluid, and in the latter case, the contents were a yellowish mucous fluid. Kuriloff2 indicated that NC generally contains mucoid or yellowish serous fluid, but some cases with acute infection contain brown fluid. This difference of contents may influence the MR imaging findings.
Any lesion appearing as a well-circumscribed soft mass occurring beneath the alar base should raise the possibility of NC. Many diseases that include NC in the differential diagnosis have been described in past reports,1,2,7 but there have never been reports comparing the detailed findings of these lesions. Our report may be the first showing detailed clinical and MR imaging findings of diseases requiring a differential diagnosis that includes NC.
Generally, the most common differential diseases may be odontogenic lesions, especially inflammatory conditions following dental disease.7 Odontogenic lesions can be easily differentiated by the dental radiographic appearance. However, soft-tissue tumors require CT and MR imaging examinations to assess the characteristics of these lesions, including the location. In the past, the most common technique to help in the diagnosis of NC was aspiration of the cyst fluid and replacement of the fluid with contrast medium to visualize the lesion on radiographs. This procedure is a standard examination for confirming the cystic character of the lesion. However, the recent popularity of MR imaging has diminished the advantages of this diagnostic technique because it carries the risk of infection.13 So, the importance of the assessment of the location and the 3D form of the lesion on MR images is increasing, as well as the assessment of the contents of the lesion. Our case of schwannoma located beneath the ala nasi showed clinical features and simple MR imaging findings resembling NC. However, the lesion was located laterally compared with NC, and the tumor was round, without any interference from surrounding anatomic structures. On the other hand, in our patients, NC appeared as a rounded mass but with some deformities, which may be influenced by its development pattern. These 3D morphologic differences are helpful for the diagnosis of NC.
On the basis of the MR imaging findings of our presented cases and past reported cases in the literature,1,8 the appearances of NC on MR images may be summarized as follows: The axial view reveals a rounded mass located between the outline of the ala nasi and the anterior nasal spine, often with scalloped bone resorption in large lesions. The lesion is likely to extend to the nasal cavity and often contacts the inferior nasal concha. The sagittal view of a section including the nasal cavity shows a bean shape in cases extending toward the nasal cavity beyond the edge of the base of the nasal aperture. This view also shows well the protrusion of the anterior nasal vestibule. The coronal view can show well the location of the lesion, which is limited to a location between the lateral outline of the alar nasi and the midline. The anterior nasal spine interferes with the growth of the lesion, and this interference often results in a beanlike appearance in this view.
Sagittal and coronal views of MR images show the characteristic features of NC, in which the lesion grows on the bone, and this appearance may show the close relationship between NC and the nasal structures and may aid in the diagnosis, in addition to the histologic findings of NC. Future analysis of the varying sizes of this lesion by MR imaging may contribute to the clarification of the origin of this lesion.
Footnotes
This work was partly supported by a grant from the Ministry of Education, Science and Culture of Japan (No.17659633).
References
- Received June 24, 2005.
- Accepted after revision October 5, 2005.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}