
Abstract
SUMMARY: Digital subtraction angiography through the central artery of the ear was performed to show elastase-induced aneurysms in 34 rabbits. Twenty-eight (82%) aneurysms in which common origins of the bilateral common carotid artery (CCA) were found were well shown. All 6 other aneurysms not well shown had separate origins of the CCAs from the aortic arch (P < .001). This method can be used for angiographic follow-up when there is a common origin of the CCAs.
Currently, conventional intra-arterial digital subtraction angiography (IADSA) through the femoral artery is the standard technique to examine the dimensions of an aneurysm in rabbits,1–4 though it is invasive and expensive. As a less-invasive, simple, and economic technique, IADSA through the central artery of the ear was reported recently.5 We set out to validate the use of IADSA through the ear artery for evaluation of elastase-induced aneurysm models in rabbits.
Description of the Technique
Elastase-induced saccular aneurysms created at the origin of the right common carotid artery (RCCA) in 34 New Zealand white rabbits (body weight, 3–4 kg) were analyzed in this study, including 8 uncoiled aneurysms and 26 aneurysms previously embolized with platinum coils. All procedures were approved by our Institutional Animal Care and Use Committee. Detailed procedures for aneurysm creation have been described.6 Briefly, the stump of the RCCA was converted to an “aneurysm” cavity by distal ligation and intraluminal incubation of porcine elastase. Aneurysm embolization, when performed, was done from a transfemoral approach, as previously described in detail.1–2
IADSA
IADSA through the central ear artery of the left ear was performed in all 34 aneurysms. The left ear was chosen because the contrast can flow retrogradely into the aortic arch through left common carotid artery (LCCA) (Fig 1). On the right side, the RCCA was occluded during aneurysm creation, so retrograde flow to the aortic arch would be difficult.

Ear IADSA showing contrast from the left ear artery (left block arrow) to the parent artery of the aneurysm.
A 24-gauge angiocatheter was placed in the central artery of the left ear. Digital subtraction angiography (DSA) (Advantx, GE Healthcare, Milwaukee, Wis) at 2 frames per second was performed after injection of 7 mL of iodinated contrast material (iohexol, Omnipaque 300, GE Healthcare, Piscataway, NJ) through the catheter for 2 seconds; the injection rate was approximately 3 mL/s. Radiopaque sizing markers, consisting of metallic spheres ranging from 2–7 mm in diameter, were placed over the chest, as close as possible to the brachiocephalic artery but not obscuring the region of the aneurysm.
Conventional IADSA from a transfemoral approach was also performed in 22 of the 34 aneurysms. Briefly, a cut-down was performed over the right common femoral artery, and a 5F sheath was placed in the artery. The side-port of the sheath was flushed with heparinized saline; then, a bolus of heparin (100 U/kg) was delivered through the sheath. A 5F Envoy catheter (Cordis Endovascular, Miami Lakes, Fla) was advanced into the brachiocephalic artery through the sheath under fluoroscopy. DSA at 2 frames per second was performed with a hand injection of 5 mL of iodinated contrast material (Omnipaque 300) at a rate of approximately 3 mL/s.
Intravenous DSA (IVDSA) was performed in the other 12 aneurysms. Detailed procedures for IVDSA have been described elsewhere.7
Image Quality Evaluation
Image quality of the central ear artery DSA was evaluated. Two categories were classified for consideration: grade A, in which both the aneurysm and parent artery were clearly shown; and grade B, in which any portion of the aneurysm and/or parent artery was not well shown. All DSA images for any given subject were viewed separately by the 2 experienced observers, an experienced neuroradiologist (D.F.K.) and a trained research fellow (Y.H.D). Agreement was reached between the 2 observers for all aneurysms.
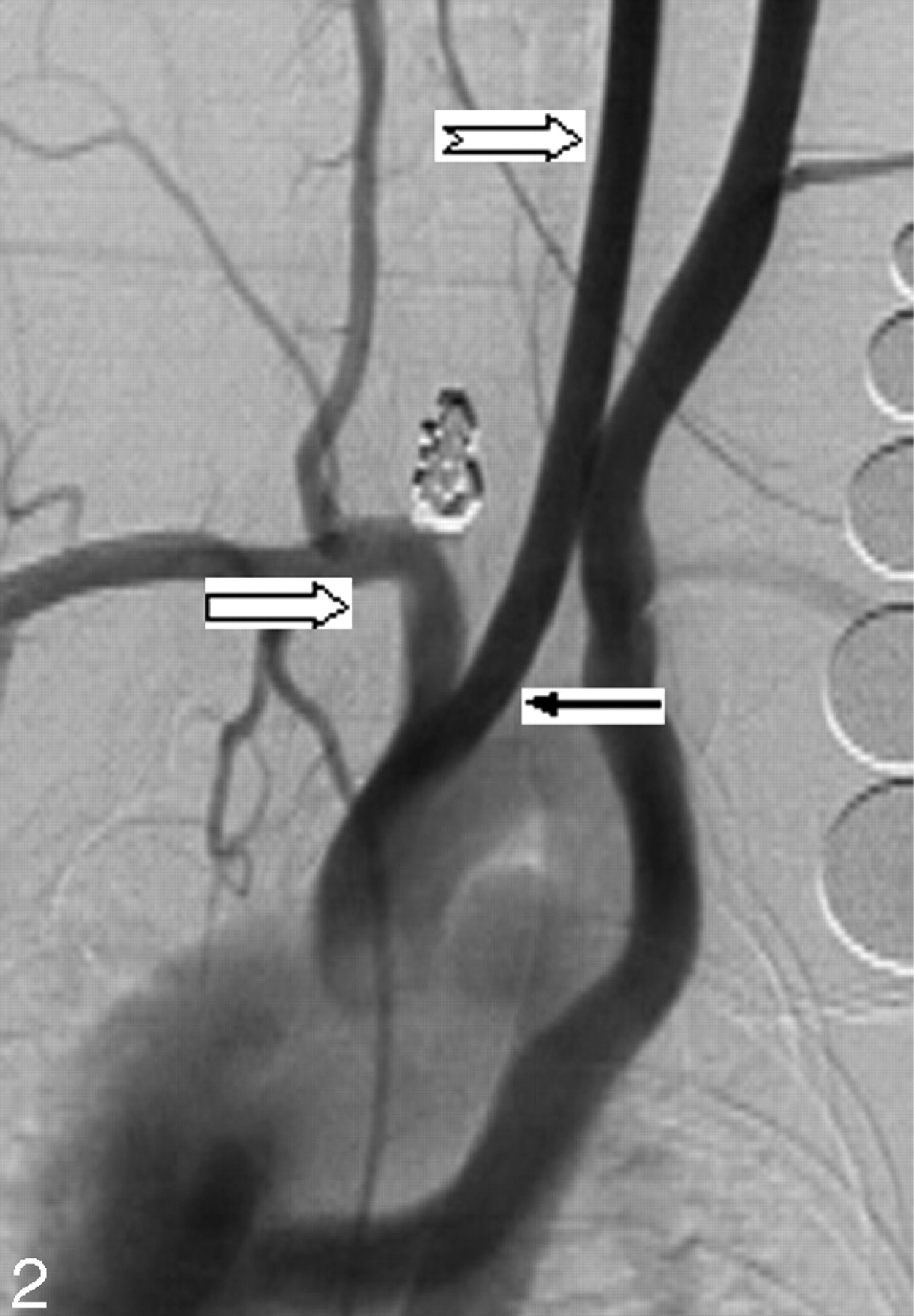
Twenty-eight (82%) of the 34 cases were considered grade A, or good, image quality (Fig 2). Six (18%) of 34 aneurysms were judged grade B, or poor, image quality. Of these 6 cases, 2 had poor opacification of the aneurysm neck region, 3 had poor opacification of the parent artery, and 1 had poor opacification of both the parent artery and neck region (Fig 3).

Ear IADSA. Both embolized aneurysm and parent artery (right block arrow) are well shown. Note that more contrast fills the LCCA (notched right arrow) because contrast material is injected through the left ear artery. In addition, LCCA and RCCA originate at the same location from the aorta (black arrow).

IADSA through the left ear artery. Both embolized aneurysm and parent artery (right block arrow) are not well shown. Note that the LCCA (notched right arrow) is seriously opacified. On the contrary, the parent artery is very faint. LCCA and RCCA, originating separately from the aorta (black arrow).
Anatomic Evaluation
There were 2 types of vessel origination: type A, with a common origin for the RCCA and LCCA; and type B, with separate origins of the RCCA and LCCA from the aortic arch. All 28 aneurysms with grade A image quality had type A anatomic configuration (Fig 2). In all 6 cases with poor opacification (grade B), anatomic configuration type B was shown (Fig 3).
Statistical Analysis
The relationship between image quality and anatomic configuration was compared by using the Fisher exact test. Image quality was coordinated with vessel origination (P < .001).
Discussion
Elastase-induced aneurysms in rabbits have been proved to be an excellent model for preclinical device development and basic neurovascular research.7–11 Unfortunately, because of the small size of the femoral artery, placement of arterial catheters usually requires ligation of the access vessel. Thus, serial studies by using conventional angiographic follow-up are either extremely difficult or impossible. The current study showed that most aneurysms can be well shown by IADSA through the central artery of the left ear.
The observation that separate origin of the carotid arteries leads to poor image quality could be predicted on the basis of the pattern of contrast opacification with ear artery DSA. The contrast fills retrograde down the LCCA into the aortic arch. If the origin of the LCCA is separate and downstream from the RCCA, then opacification of the aneurysm is poor. In the cases of common origins of the carotid arteries, the contrast traverses the brachiocephalic artery before entering the aortic arch. Then the contrast is carried antegrade to opacify the aneurysm.
IADSA through the central artery of the ear artery offers numerous advantages compared with IADSA from a transfemoral approach. IADSA through the ear artery is less invasive and economic, and most important, it can be repeated many times in each rabbit subject. Thus, this method is especially useful for studies using multiple time point follow-ups. In addition, it offers high concentrations of intravascular contrast, which we consider superior to that achieved by using IVDSA.
There are several technical limitations that decrease the accuracy of IADSA through the ear artery. In most cases, the concentration of intravascular contrast is less than that achieved with transfemoral angiography, with the catheter placed in the brachiocephalic artery. Another factor is motion artifact, which may be substantial in some cases because contrast may irritate the subject during injection. Third, anatomy variation, such as separate origin of the carotid arteries from the aortic arch, impacts the image quality. Previous series of ear artery DSA noted favorable anatomy in approximately 60% of 23 rabbits.5 Our series, which was slightly larger, had favorable arch anatomy for ear DSA in more than 80% of cases. Variation may depend on the source of the rabbits, though the New Zealand white rabbit represents a highly out-bred species.
Other investigators have used noninvasive methods such as CT angiography and MR angiography for follow-up of experimental aneurysms in rabbits.12 Also, in intraoperative angiograms obtained clinically, the superficial temporal artery may be accessed to allow retrograde opacification of the carotid arterial system.13 We offer IADSA through the ear artery as a complementary technique, especially in laboratories without MR and CT scanners available for animal research.
Conclusion
Angiographic follow-up of right-sided elastase-induced aneurysms in rabbits can be performed by using the central artery of the left ear when there is a common origin of the CCAs from the aortic arch.
Footnotes
This study was supported by NIH grant NS42646.
References
- Received July 29, 2005.
- Accepted after revision April 2, 2006.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.