
Abstract
BACKGROUND AND PURPOSE: Unilateral vocal cord paralysis (UVCP) occurs after iatrogenic injury or disease process and is associated with dysphonia and aspiration. Various surgical options are available for treatment of UVCP, including vocal cord medialization thyroplasty and injection laryngoplasty. These augmentative procedures improve phonation and airway protection. Our purpose was to demonstrate the CT appearance of implants used for the treatment of UVCP.
METHODS: Twelve patients treated surgically for UVCP were studied with helical CT. The vocal cords were augmented by using Silastic implants (n = 7), polytetrafluoroethylene (Gore-Tex) implants (n = 2), Teflon injections (n = 2), or fat injection (n = 1). Augmented vocal cords were characterized by size, shape, and Hounsfield units (HU). Two other patients with failed medialization thyroplasty were evaluated for the position of the extruded implant relative to the paralyzed vocal cord.
RESULTS: The 7 Silastic implants were triangular and hyperattenuated (293.4 ± 90.4 HU). The 2 Gore-Tex implants were heterogeneous with lobulated medial margins and were hyperattenuating (320 and 414 HU). The injected materials demonstrated ovoid/masslike configurations: the 2 Teflon injections were hyperattenuated (107 and 429 HU), and the fat injection was hypoattenuated (−102 HU). Inferior displacement of the implant was demonstrated relative to the true vocal cord in 2 patients with failed Silastic thyroplasties.
CONCLUSION: CT can distinguish various types of vocal cord augmentation. Silastic implants are recognized by their characteristic triangular configuration. The Gore-Tex implants had unique heterogeneous attenuation with lobulated medial margins. Fat and Teflon injections both appear ovoid/masslike. Teflon injection should not be mistaken for tumor.
Unilateral vocal cord paralysis (UVCP) can cause dysphonia and aspiration because of glottic incompetency. UVCP is often the result of recurrent laryngeal nerve involvement from iatrogenic injury following thyroid surgery or from direct tumor extension. With the exception of the cricothyroid, the intrinsic muscles of the larynx are innervated by the recurrent laryngeal nerve. Injury to the nerve results in diminished vocal fold tone, bulk, and mobility.1 CT can be used to characterize UVCP. In a representative patient, UVCP presented as a flaccid atrophic left vocal cord. It was paramedian in position, and there was associated dilation of the glottic airway (Fig 1).

Postcontrast axial CT image of a flaccid atrophic left vocal cord (arrow). It is paramedian in position, and there is associated dilation of the glottic airway.
Surgical options for treatment of UVCP include vocal cord medialization by injection laryngoplasty or by thyroplasty.2 Injection laryngoplasty involves direct injection of a biocompatible material into a paralyzed true vocal cord guided by endoscopic visualization. This provides bulk to the affected vocal cord, thereby improving its opposition to the unaffected contralateral vocal cord. It is a minimally invasive technically simple procedure that can be performed with the patient under local anesthesia.2 Injection laryngoplasty is the oldest method of treatment of UVCP. Paraffin was used as an injection material as early as 1911.3 A number of other substances have been used to augment vocal cords. However, foreign body reactions to substances such as polytetrafluoroethylene (PTFE) (Teflon; Dupont, Wilmington, Del) and migration from injection sites have limited the substances currently acceptable for injection laryngoplasty primarily to collagen and fat.4
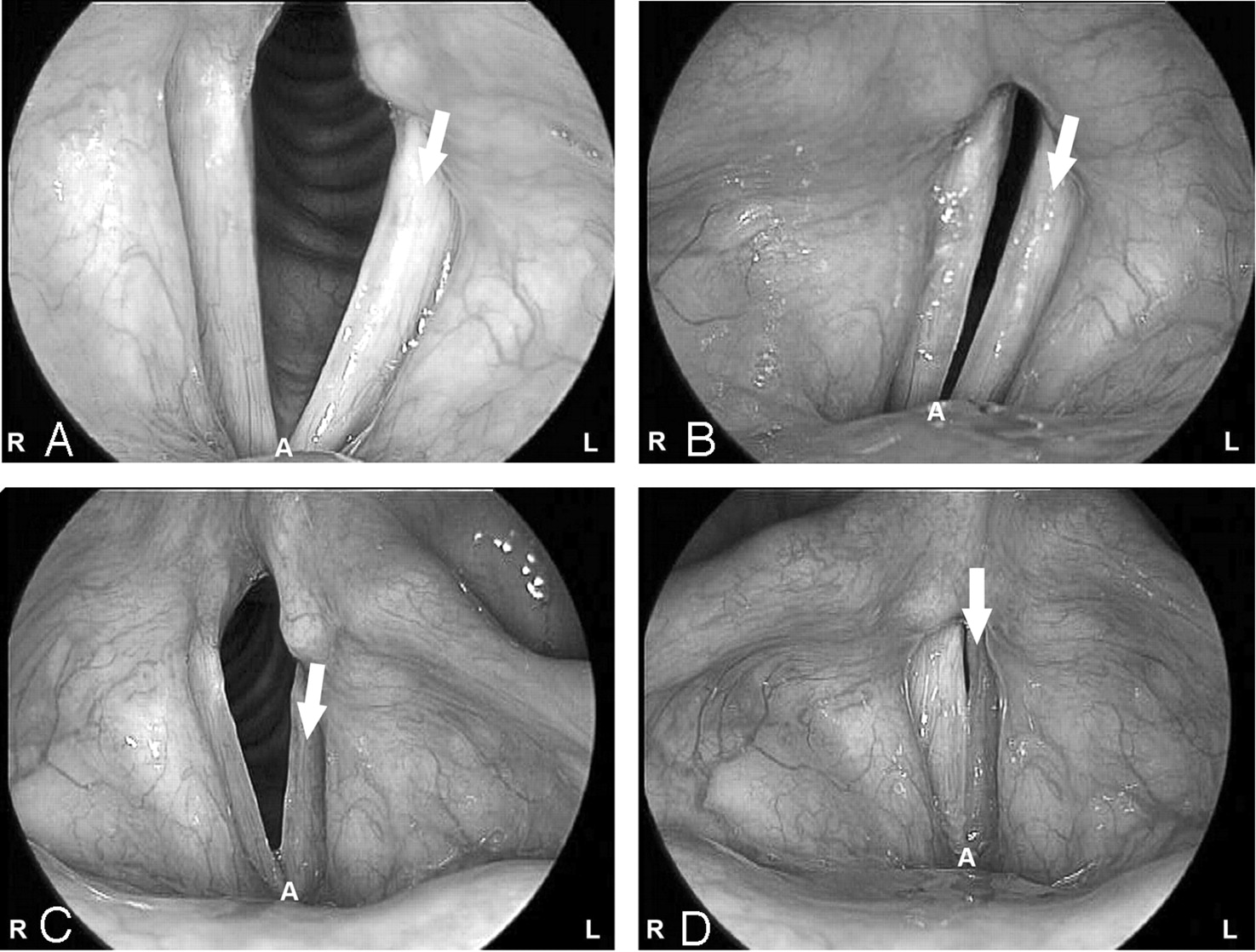
Medialization thyroplasty was first described by Payr5 in 1915 and was later described by Isshiki et al6 in 1975. The technique was modified by Montgomery in 1997.7 The Montgomery prosthesis is Silastic (Dow Corning, Auburn, Mich) and is constructed of triangular plastic. It is inserted surgically through a window in the thyroid lamina at the level of the vocal cord. The contour of the implant is designed to medialize the true vocal cord, thereby improving glottic competency and facilitating phonation and airway protection.7 Videostroboscopy evaluates vocal fold movement and vibration in patients with vocal cord paralysis.8 Videostroboscopy is often used to assess patients with vocal cord augmentation and help determine which type of procedure will provide the most benefit. Fig 2A, -B shows the preoperative videostroboscopy in a patient with cervical esophageal cancer, demonstrating a paralyzed left vocal cord. Following medialization thyroplasty using a Montgomery Silastic implant, videostroboscopy (Fig 2C, -D) demonstrated that the left vocal fold was midline and glottic closure was improved during vocal fold adduction.

A and B, A 57-year-old woman status postresection of cervical esophageal cancer, with left vocal cord paralysis. Preoperative videostroboscopy demonstrates the paralyzed vocal cord (arrow) during abduction (A) and adduction (B). Note the complete lack of glottic closure during vocal cord adduction. A indicates anterior commissure.
C and D, Postoperative videostroboscopy in abduction (C) and adduction (D), in the same patient following medialization thyroplasty performed using a Montgomery Silastic implant. The left vocal fold is now midline, and glottic closure is improved during vocal cord abduction (arrow in C) and adduction (arrow in D). A indicates anterior commissure.
The CT appearances of the medialization thyroplasty and injection laryngoplasty are unique. The purpose of this study was to demonstrate the CT appearance of vocal cord augmentation procedures performed by otolaryngologists and head and neck surgeons. An understanding of the appearance of vocal cord augmentations is useful to avoid misinterpretation of implants as pathology. In addition, accurate localization of extruded implants with high-resolution CT is helpful before revision surgery.
Methods
A retrospective analysis of 12 patients at our institution who had undergone augmentation for vocal cord paralysis was performed with axial CT (General Electric, Milwaukee, Wisc). The section thicknesses used were 1.25, 2.5, or 5.0 mm. Augmented vocal cords were characterized by size, shape, and Hounsfield units (HUs). The images were reviewed by an experienced head and neck radiologist (L.E.G.). Measurements were obtained by using a calibrated CT ruler. Mean CT attenuation values of the vocal cord augmentations were obtained by means of region of interest analysis. The 2 patients with failed medialization thyroplasty were studied with 1.25-mm high-resolution CT of the larynx with coronal and sagittal reformations. The position of the extruded implants was evaluated relative to the paralyzed true vocal cord.
Results
Patient demographics included thyroid cancer,8 esophageal cancer,2 lung cancer,1 and neck lymphoma.1 Ages ranged from 34 to 75 years with a mean age of 60 years. Sex distribution was 1:1. Seven patients had right vocal cord paralysis (VCP) and 5 patients had left VCP.
Seven Montgomery Silastic implants were triangular and visually hyperattenuated (Fig 3). The mean dimensions were 1.4 ± 0.2 cm (length) and 1.2 ± 0.3 cm (width). The mean HU was 293.4 ± 90.4. The 2 polytetrafluoroethylene implants (Gore-Tex, W.L. Gore & Associates, Newark, Del) had medial lobulated borders, and were heterogeneous (Fig 4). They measured 1.8 × 0.7 cm, 414 HU; and 1.6 × 0.9 cm, 320 HU, respectively. The 2 Teflon injections were visually hyperattenuated and masslike (Fig 5). One measured 1.2 × 1.1 cm, 107 HU; the other measured 1.4 × 0.7 cm, 429 HU. The fat injection was ovoid and hypoattenuated (Fig 6), and it measured 1.5 × 0.9 cm, −102 HU. In 2 patients, the extruded Silastic was found inferior to the level of the paralyzed true vocal cords. (Fig 7A, -B).

A 57-year-old patient with mediastinal lymphoma resulting in left vocal cord paralysis status postmedialization thyroplasty. Axial CT image (noncontrast) demonstrates the typical attenuated triangular configuration of a Montgomery Silastic implant (arrow).

A 62-year-old patient status postresection of medullary thyroid cancer and right vocal cord medialization with Gore-Tex. Axial, postcontrast CT image demonstrates a heterogeneous hyperattenuated material in the right true vocal cord with a lobulated medial margin (arrow).

A 73-year-old patient with metastatic squamous cell cancer of the esophagus, status post XRT and left-sided Teflon injection. Axial noncontrast CT image demonstrates masslike hyperattenuated material in the left true vocal cord (arrow).

A 71-year-old patient with recurrent papillary thyroid cancer status post fat injection. Axial postcontrast CT image shows an ovoid hypoattenuated mass in the right vocal cord (arrow) with attenuation values corresponding to the surrounding subcutaneous fat (−102 HU).

A and B, Axial and coronal high-resolution CT images of the larynx in a 73-year-old patient with papillary thyroid cancer and left vocal cord paralysis. A left-sided Silastic implant is extruded lateral (large white arrow in A) and inferior to the level of the true vocal cord (large white arrow in B). The block arrow indicates the true vocal cord; small white arrow, inferior thyroid cartilage.
Discussion
The recurrent laryngeal nerves innervate the abductors and adductors of the true vocal cords. Iatrogenic injury or invasion of the recurrent laryngeal nerve results in paralysis of the ipsilateral vocal cord. UVCP can present in many ways. Direct signs of UVCP include vocal cord atrophy, paramedian displacement, anteromedial deviation of the arytenoid cartilage, and/or atrophy of the posterior cricoarytenoid muscle. Indirect signs of UVCP include dilation of the glottic airway, an inwardly positioned aryepiglottic fold, and/or ipsilateral enlargement of the pyriform sinus or laryngeal ventricle.
Medialization by thyroplasty and injection laryngoplasty are 2 methods used by otolaryngologists and head and neck surgeons to improve phonation and airway protection. CT imaging can distinguish between various types of vocal cord augmentations.
Montgomery Silastic medialization thyroplasty is a popular external framework surgery. Silastic implants are constructed of silicone. The base of the implant projects posteriorly to contact the base of the vocal process of the arytenoid, thus improving closure of the posterior commissure. The CT appearance of the Silastic implants we studied were hyperattenuated and were distinguishable by their classic triangular configuration.9 The axial plane best captured its shape.
Gore-Tex10 has multiple uses, including applications in vascular surgery and cosmetic surgery. Similar to Silastic implants, Gore-Tex is inserted through a window in the thyroid cartilage in the form of strips that are layered, which provide bulk to the vocal cord. The Gore-Tex implants we reviewed had hyperattenuated heterogeneous attenuation with lobulated medial margins that distinguished them from Silastic implants. The development of inflammatory foreign body reactions seen in Teflon injections is less frequent with Gore-Tex because of the absence of free particles.10
Teflon injection laryngoplasty was first introduced in the 1960s. Teflon injections were a popular form of vocal cord augmentation in the 1980s. They achieved good voice results and were thought to be inert. However, Teflon injections fell out of favor because of delayed inflammatory foreign body reactions. This inflammatory reaction (Teflon granuloma) can produce intense fluorodeoxyglucose false-positive uptake on positron-emission tomography imaging.11–13 The 2 Teflon injections evaluated in our study were masslike and hyperattenuated. On enhanced CT, Teflon injections can be mistaken for enhancing tumor or malignant tumoral calcification. Teflon granulomas can be infiltrated with enhancing scar tissue simulating tumoral enhancement. If a Teflon granuloma is suspected, MR imaging can be helpful. Harrigal et al13 demonstrated that Teflon granulomas display low-to-intermediate T2 signal intensity, whereas tumor typically displays high T2 signal intensity.
Autologous fat can be used in patients who are expected to regain some vocal cord function. It may also be used as a bridge to surgical medialization with Silastic or Gore-Tex. It is often harvested from the paraumbilical region. The single fat injection studied was ovoid and was easily recognized because of its characteristic low attenuation (isoattenuated to subcutaneous fatty tissue). Fat injection is ideal when the glottic gap is relatively small and the volume of fat needed to rebulk the vocal fold is less than or equal to 1 mL.4 Fat injections do not result in granuloma formation as documented with Teflon injections. Fat resorption is generally thought to be inevitable; overinjection of fat is usually recommended.14 However, Brandenburg et al15 used MR imaging to verify that fat survives transplantation in the vocal cord. In addition, they showed that even when damage to fat cells occurred; fibrous connective tissue replaced damaged fat, maintaining the contour and bulk of the vocal fold.
In our study, failed medialization thyroplasty was observed in 2 patients. In both patients, the Silastic implant was displaced inferior to the paralyzed true vocal cord. Implant dislodgement can also occur posteriorly and superiorly. Axial sections (1.25 mm) of the larynx were performed with sagittal and coronal reconstruction for preoperative evaluation of the extruded implants. Woo et al16 found that the most common cause of failed medialization thyroplasty was arytenoid malrotation, resulting in a persistent posterior glottic gap. They found high-resolution CT of the larynx useful in determining the degree of arytenoid rotation and the position of the arytenoid cartilage on the cricoid facet. This complication was amenable to arytenoid adduction and revision medialization thyroplasty. Other causes of medialization thyroplasty failure include movement of the implant, an improperly sized implant, or an improperly placed implant. These problems can be identified on high-resolution CT and potentially corrected with revision medialization thyroplasty.16
Conclusion
CT can distinguish various types of vocal cord augmentation. Silastic implants are recognized by their hyperattenuated triangular configuration. Gore-Tex implants have unique heterogeneous attenuation with irregular medial margins. Fat injection has a low-attenuation ovoid mass. Teflon injections are hyperattenuated and masslike and should not be mistaken for tumor. Finally, high-resolution CT of the larynx is useful for localization of extruded implants before revision thyroplasty.
Footnotes
Presented at the 38th annual meeting of the American Society of Head and Neck Radiology (ASHNR), Philadelphia, Pa, Sept 29–Oct 3, 2004.
References
- Received October 8, 2005.
- Accepted after revision December 2, 2005.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}