
Abstract
Summary: Enlarged parietal foramina are believed to be benign and familial and due to a variable degree of defective intramembranous ossification of the parietal bones. We report 2 patients with this condition in whom fetal and neonatal MR imaging studies illustrate the antenatal and perinatal evolution of this condition and the associated persistence of a falcine sinus. We discuss its relationship to the spectrum of cephalocoeles.
Enlarged symmetrical parietal or frontal foramina and cranium bifidum are believed to represent variable expression of the same genetic defect, depending on the age and phenotypic heterogeneity of the patient.1 They are remnants of arrested fetal cranial development and can be very large and midline at birth but usually close during mid-childhood, leaving only paired foramina in the parietal or frontal bones, which may persist throughout life. Because high-resolution antenatal sonography and MR imaging (MRI), as well as neonatal MRI, allow early detection of cranial and intracranial anomalies, the developmental features of this benign condition should be recognized. The MRIs of 2 infants who presented to our institution with findings compatible with enlarged parietal foramina were reviewed.
Case Reports
Case 1
An abnormal, large parietal skull defect crossing the midline was detected in the fetus on a routine 19-week obstetric sonography (Fig 1). A cyst was noted in the place of the bone defect, with the inner surface being intact dura and the outer surface being in continuity with the bone. The cyst measured 27 × 16 × 9 mm (transverse × anterior–posterior × cranio–caudal). The brain was sonographically normal. Fetal MRI was performed at 23 weeks (Fig 2, upper) to further evaluate the abnormality and the brain. At that time bilateral symmetrical defects of the calvarium were noted in the parietal bones along the midline, measuring 13 × 10 × 5 mm each and filled with CSF. The underlying brain was normal for gestation. Follow-up imaging at 36 weeks gestation (Fig 2, middle) demonstrated normal maturation of the brain, with ongoing calvarial defects, but less prominence of the associated CSF spaces. The infant was clinically normal at birth. Postnatal MRI of the brain at 1 month of age (Fig 2, lower) still demonstrated the calvarial anomalies, with the surface of the brain conforming to the contour anomaly of the overlying skull. In addition the venous drainage was shown to be anomalous, with absence of the straight sinus and a persistent falcine sinus draining into the sagittal sinus at the level of the skull defects. This venous anomaly was also evident on the 2 fetal MRI studies (black arrows).

Patient 1. Obstetric sonogram at 19 weeks gestation.
Parasagittal image of the brain shows the calvarial defect and cyst covered by dura and skin (white arrow).



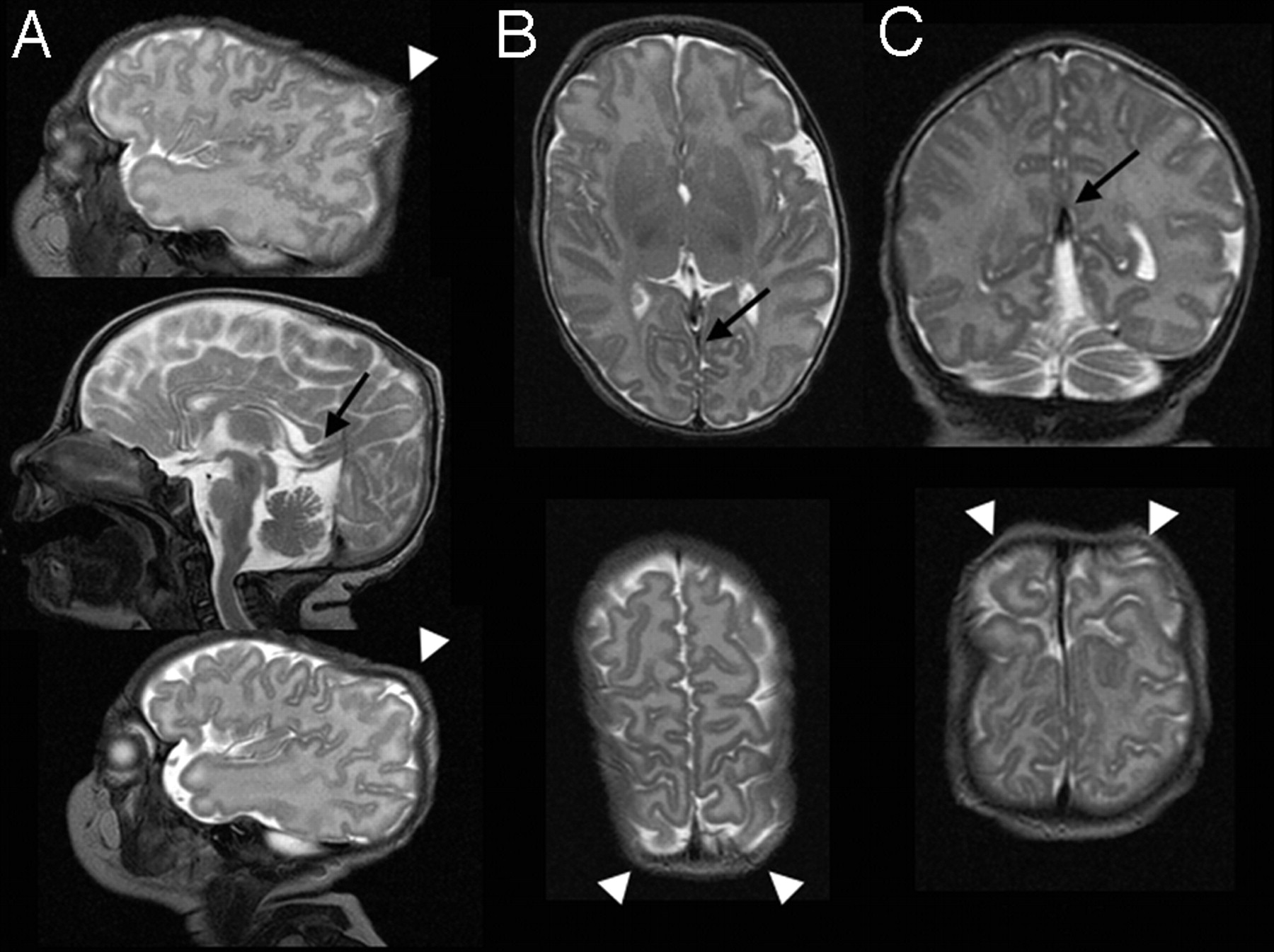
Patient 1. Fetal and neonatal brain MRIs.
Upper, Fetal MRI at 23 weeks gestation (single-shot, fast spin-echo).
Middle, Fetal MRI at 36 weeks gestation (single-shot, fast spin-echo).
Lower, Neonatal MRI (fast spin-echo T2).
A, Sagittal images.
B, Axial level of the thalami (upper) and parietal bones (lower).
C, Coronal level with the posterior lateral ventricles (upper) and parietal bones (lower).
Note: White arrows, parietal foramina with calvarial defects initially filled by CSF and then brain; black arrows, course of the abnormal interhemispheric venous drainage. Note the absence of the normally positioned straight sinus.)
Case 2
A healthy female infant born at 35 weeks’ gestation presented at birth with a palpable parietal skull defect. MRI performed at 1 month of age to assess the underlying brain demonstrated similar imaging findings to patient 1 with bilateral parietal skull defects, slight herniation of the underlying brain to conform to the defects, and absence of the straight sinus with a persistent falcine sinus flowing into the sagittal sinus at the level of the anomaly (Fig 3).

Patient 2. MRI at 1 month of age (FSE T2; white arrows, parietal foramina with calvarial defects; black arrows, course of the abnormal interhemispheric venous drainage, note absence of the normally positioned straight sinus).
A, Sagittal images.
B, Axial level of the thalami (upper) and parietal bones (lower).
C, Coronal level with the posterior lateral ventricles (upper) and parietal bones (lower).
Discussion
The normal calvarium is formed by intramembranous ossification, where bone is formed directly from mesenchyme. “Cranium bifidum” and giant parietal and frontal foramina are believed to be variable expressions of a disorder of calvarial ossification. During development, a single defect initially involves the bones on either side of the midline and is subsequently divided into 2 foramina by parasagittal islands of ossification. At birth, either a large midline or bilateral skull defects are present. The underlying brain is covered by a membrane of dura and pericranium, and the overlying scalp is intact. The defects tend to close during mid-childhood, often leaving symmetrical foramina. A familial incidence with autosomal dominant inheritance is recognized and more recently specific gene mutations have been identified.1–3
There are few previous reports of brain MRI in individuals with giant parietal foramina, with imaging confined to adults and children.3,4 Although the condition is believed to be benign, cross-sectional imaging with CT and MRI has uncovered associated intracranial anomalies, in particular abnormal venous development, as seen in our patients. In a series of 7 patients (adults and children) who had undergone either CT or MRI, 6 had a persistent falcine sinus with associated hypoplasia or atresia of the straight sinus.4 In another series of 3 members of one family who underwent MRI, all also had this venous anomaly.3 A mesenchymal disturbance has been postulated as primary cause for both the bone and vascular abnormalities.3 Six of the 10 patients in these 2 series also had asymptomatic mesial occipital polymicrogyria. These are the only intracranial abnormalities reported in association with enlarged parietal foramina to date. Although the size of the calvarial defects varies between individuals and decreases with age, there is no indication that there is any relationship between their size and the associated brain anomalies.
Giant parietal foramina have been detected occasionally on antenatal sonography in the mid-trimester.5,6 As in our patient, a single ossification defect involving both parietal bones but without herniation of membranes or brain beyond the confines of the skull is described. There is no previous description of the fetal MRI findings.
Atretic parietal cephaloceles, also associated with midline skull defects, usually present as a subcutaneous midline cyst or nodule and are associated with abnormality of the overlying scalp. In parietal foramina, there is no mass and the overlying scalp is always normal. Abnormalities of venous drainage very similar to those seen with giant parietal foramina are recognized in association with atretic cephaloceles/meningoceles.7–10 The constellation of an absent or rudimentary straight sinus with an alternative venous drainage between the hemispheres that joins the sagittal sinus in a high position is believed to be due to interruption of the normal development of the venous drainage systems. The alternative venous drainage is variably believed to either represent a falcine sinus9 or the straight sinus in an embryonic position.8,10 Although the exact embryologic origin of atretic cephaloceles is uncertain,11 they probably arise from failure of closure of the neuropore during the third to fourth week of gestation. The parietal bones start to ossify around week 7–8. The straight sinus only develops from the primitive venous plexuses by week 10.9,12 Abnormal development in the parietal midline before this therefore may prevent the normal progress of venous sinus formation.
Parietal foramina associated with an atretic cephalocele4 and symmetrical parietal meningoceles12 have been documented. In both cases the abnormal venous anatomy was present.
In summary, to the best of our knowledge intracranial MRI findings in patients with giant parietal foramina have been reported in only a few children and adults and have not been described previously in the fetus and neonate. The abnormal venous drainage with persistence of a falcine sinus and atresia or hypoplasia of the straight sinus, which is present in most, can be recognized on fetal MRI. Similar venous anomalies are seen in both this condition and atretic parietal cephalocoeles, raising the possibility that enlarged parietal foramina may represent the benign end of the same developmental spectrum. Recognition of the early imaging features of this condition is important because the lesions can appear alarming ante- and perinatally. Awareness of the venous anomaly is imperative before surgical management. Follow-up imaging in childhood to screen for any other associated developmental brain anomaly, in particular occipital cortical dysplasia, may be warranted.
Acknowledgments
We thank Dr Amanda Sampson, from the Department of Obstetric Sonography at the Royal Women’s Hospital in Melbourne, for the antenatal sonography image.
References
- Received May 11, 2005.
- Accepted after revision August 2, 2005.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}