
Article Figures & Data
Figures
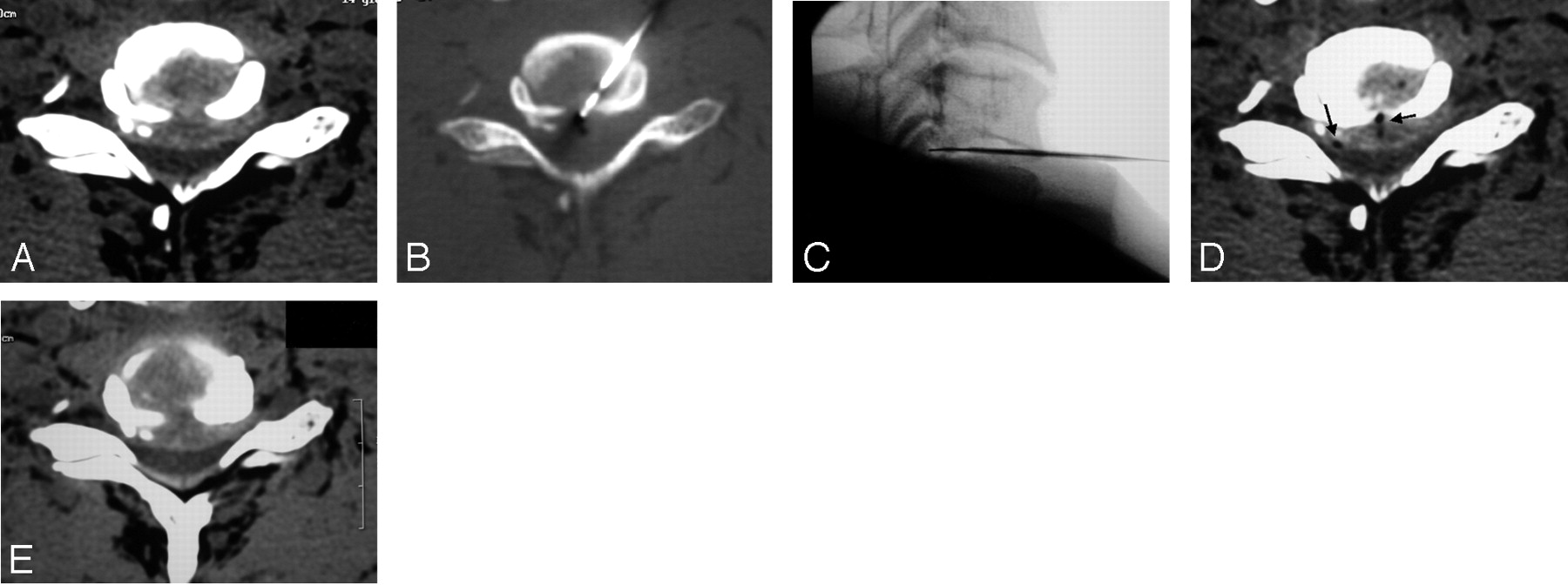
- Fig 1.
A, The 19-gauge cannula with an internal mandrel is positioned against the anterior surface of the annulus fibrosus. The cannula is held by a surgical forceps to minimize x-ray exposure of the surgeon’s hand.
B, Cannula placement as observed under fluoroscopy.
C and D, The cannula is advanced into the disk, and the SpineWand device (D, arrow) is introduced into the nucleus pulposus via the cannula.
E, The device is activated and then rotated 360°(E) to create a spheric void by means of the loop-shaped active electrode (arrow). Between 2 and 4 voids are ablated in a linear direction to create a channel.
F, After the first channel into the disk is completed, the device is repositioned to a different part of the nucleus, with the placement depending on the topography of the herniation. For left-sided herniations, the first channel is made in an oblique direction, from the right anterolateral entry point toward the left posterolateral herniation; the other channel is made on the midline and directed toward the posterior profile of the disk. For a right-sided lesion, the first channel is directed obliquely toward the center of the disk; the second channel is directed toward the right paramedian, along the medial surface of the uncal process to reach the herniation in the posterior aspect of the disk.
G, A schematic drawing shows the entry route, with the clinician’s fingers pushing the trachea across the midline while protecting the neurovascular bundle.
- Fig 2.
A, MR imaging at baseline for a 34-year-old woman who underwent percutaneous plasma radio-frequency–based diskectomy for a disk (C6–7) herniation compressing the spinal cord and causing clinical signs of myelopathy.
B, A 7-week MR imaging follow-up shows regression of both herniation and cord compression; the patient is almost asymptomatic.
C, An MR image at 9-month follow-up shows almost complete regression of the disk herniation; the patient is completely asymptomatic.
- Fig 3.
A, Bilateral disk herniation at C6–7 encroaching the spinal canal. The SpineWand device was placed into position by using CT-guidance and switching to direct fluoroscopy for the disk ablation procedure. This allowed activation of the plasma-field energy directly inside the herniation.
B and C, The loop-shaped active electrode was inserted beyond the posterior limit of the vertebral body into the spinal canal.
D, At the end of the procedure, the gas generated from the tissue excision is evident inside the disk.
E, The 5-month follow-up image shows only minimal or questionable reduction of disk size; despite this, the patient reports good clinical improvement (Macnab 3) (see text for discussion).
- Fig 4.
A, Lateral disk herniation compressing the nerve root.
B, The cannula and SpineWand device are positioned under CT guidance and then safely and precisely directed toward the herniation.
C, Note gas from tissue excision diffusing inside the herniation itself.
D, A 4-month CT follow-up shows partial regression of the lesion; the patient reports a definite clinical improvement (Macnab 3).
- Fig 5.
A and B, The C6–7 disk before undergoing the ablation procedure because of a mostly lateral left intraforaminal herniation (A) with the associated mild central protrusion shown in a sagittal MR image (B).
C and D, MR imaging follow-up at 2 months shows hypo-T1, hyper-T2 modifications of the adjacent vertebral bodies and evidence of an inflammatory condition.
E, Partial reduction of the herniation is observed at the 2-month follow-up. The patient is completely asymptomatic despite only partial reduction of the disk herniation (see text for discussion).





Tables
Grade Definition Excellent Complete resolution of all symptoms and free of pain; no restriction of mobility; able to return to normal work and activities Good Marked reduction of pain with the patient generally satisfied, returning to work or usual daytime activities, and taking analgesics seldom or not at all Fair Some improved functional capacity; still handicapped and/or unemployed Poor Continued objective symptoms of root involvement; additional operative intervention needed at index level, irrespective of repeated operations or length of postoperative follow-up Worse Clinical symptoms considered worse than before receiving procedure Excellent Good Fair or Poor Total Macnab Grade: 2 Months 25 (45%) 19 (35%) 11 (20%) 55 (100%) Macnab Grade: 6 Months Excellent 22 4 0 26 (47%) Good 3 11 4 18 (33%) Fair or Poor 0 3 5 8 (15%) Not yet available 0 1 2 3 (5%) - Table 3:
Regression of disk herniation findings in patients who underwent postoperative MR imaging (n = 15)
Postoperative Clinical Outcome (Macnab Grade) Regression of Disk Herniation Good or Excellent Poor Yes (n = 6) 5 1 No (n = 8) 5 3 Diskitis complication (n = 1) 1 All (n = 55) Excellent (n = 25) Excellent or Good (n = 44) Fair or Poor (n = 11) P-value* Male 55% 52% (13)† 57% (25) 45% (5) .574 >45 years old 31% 24% (6) 27% (12) 45% (5) .995 Herniation direction Central 27% 24% (6) 27% (12) 27% (3) .981 Right 42% 40% (10) 41% (18) 45% (5) .993 Left 35% 36% (9) 32% (14) 27% (3) .865 >1 Disk treated 38% 24% (6) 34% (15) 55% (6) .838 Related pathology 24% 28% (7) 23% (10)‡ 27% (3)§ .803 Note:—Significance of variables determined using forward-entry binary logistic regression.
† (No. of patients).
‡ Including: multiple sclerosis (good), osteophyte and partially calcified herniation (good), osteophytes (1 case excellent, 1 case good), carpal tunnel syndrome (2 cases, excellent), C5–C6 calcified disk herniation (excellent), celiac disease and anorexia (excellent), Scleroderma-Hashimoto thyroiditis (excellent), pulmonary embolism (excellent).
§ Including: osteophytes with retrolisthesis C5–C6 (1 case), L5–S1 disk herniation already operated on 3 times (1 case), L4–L5 disk herniation (1 case).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}