
Article Figures & Data
Figures
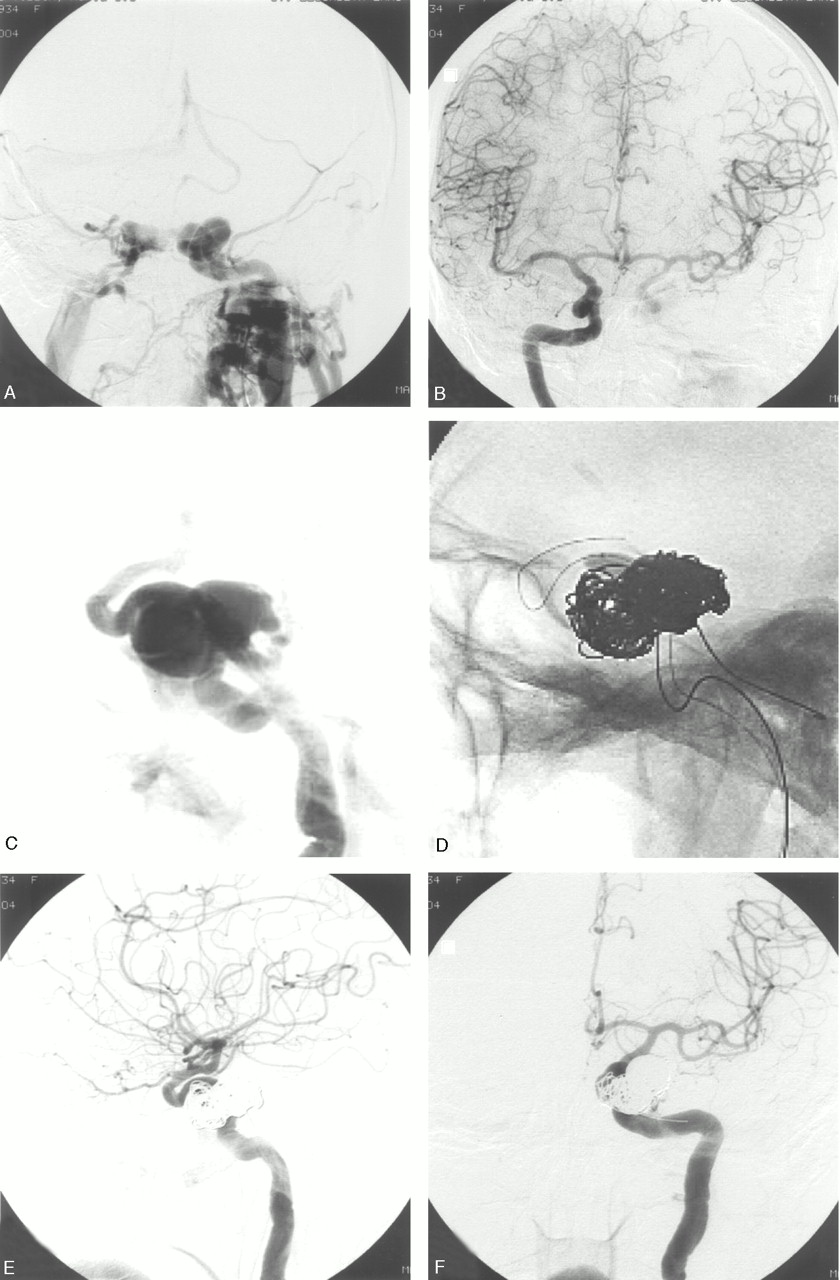
- Fig 1.
Patient 6. Ruptured left cavernous sinus aneurysm in a 70-year-old woman with bilateral exophthalmus, ophthalmoplegia, and decreased vision.
A, Frontal view of left internal carotid artery angiogram. High-flow CCF with venous drainage to both cavernous sinuses, superior ophthalmic veins, and inferior petrosal sinuses. There is some cortical venous drainage, but no filling of intracranial vessels.
B, Right carotid angiogram demonstrates overflow to the left side and some contribution to the CCF.
C, Early arterial phase shows the aneurysm.
D, Coiling with balloon protection of the carotid artery.
E and F, Closure of the CCF with patency of the internal carotid artery.
- Fig 2.
Patient 9. Ruptured right cavernous sinus aneurysm in a 74-year-old woman with bilateral exophthalmus, ophthalmoplegia, and decreased vision.
A and B, Frontal (A) and lateral (B) view of right internal carotid artery angiogram. Principal venous drainage to both cavernous sinuses and superior ophthalmic veins. There is some cortical venous drainage.
C and D, Arterial (C) and venous (D) phase of left internal carotid angiogram during test occlusion of the right internal carotid artery. Synchronous opacification of cortical veins in both hemispheres indicates tolerance to permanent occlusion.5
E, Occlusion of the ruptured aneurysm, including the internal carotid artery, with coils.
- Fig 3.
Patient 4. CCF in a 61-year-old woman with bilateral exophthalmus, ophthalmoplegia, and decreased vision.
A, Lateral view of left internal carotid angiogram shows CCF with principal venous drainage to both cavernous sinuses and superior ophthalmic veins. There is some cortical venous drainage.
B, Early arterial phase shows small cavernous aneurysm.
C and D, Selective occlusion of the aneurysm with a detachable balloon.
E and F, Follow-up angiogram after 4 months shows reopening and enlargement of the aneurysm, subsequently occluded with coils.



Tables
Clinical presentation, treatment and outcome in 11 patients with ruptured cavernous sinus aneurysms causing CCF
Patient No./ Gender/Age (y) Presentation Diagnosis Principal Venous Drainage Test Occlusion Treatment Outcome; Duration of Follow-up in Months 1/F/77 Bilateral exophthalmus and ophthalmoplegia, vision 0.1 bilateral, pulsatile bruit High-flow left CCF Bilateral superior ophthalmic vein, minor cortical venous drainage − Coiling aneurysm with balloon protection, carotid artery patent Complete recovery; 9 mo 2/F/75 Left exophthalmus and ophthalmoplegia, pulsatile bruit, decreased vision Intermediate-flow left CCF Left superior ophthalmic vein, no cortical venous drainage − Coiling aneurysm ×2 Complete recovery; 72 mo 3/F/60 Left hemiplegia and aphasia, bilateral exophthalmus and ophthalmoplegia, decreased vision, pulsatile bruit High-flow right CCF Bilateral superior ophthalmic vein, major cortical venous drainage + Coiling aneurysm with balloon protection, carotid artery patent Complete recovery; 6 mo 4/F/61 Bilateral exophthalmus and ophthalmoplegia, decreased vision, pulsatile bruit Intermediate-flow left CCF Bilateral superior ophthalmic vein, minor cortical venous drainage + Balloon occlusion aneurysm, later coiling pseudo-aneurysm Complete recovery; 18 mo 5/M/27 Left abducens palsy, decreased vision, pulsatile bruit Low-flow left CCF Left superior ophthalmic vein, left petrosal sinus, no cortical venous drainage Not done Spontaneous closure, coiling aneurysm ×2 Complete recovery; 24 mo 6/F/70 Bilateral exophthalmus and ophthalmoplegia, decreased vision, pulsatile bruit High-flow left CCF Bilateral superior ophthalmic vein, minor cortical venous drainage + Coiling aneurysm with balloon protection, carotid artery patent Complete recovery; 34 mo 7/F/51 Right exophthalmus and ophthalmoplegia, pulsatile bruit High-flow right CCF Right superior ophthalmic vein, no cortical venous drainage + Coiling aneurysm with balloon protection, carotid artery patent Complete recovery; 28 mo 8/M/58 Left exophthalmus, left abducens palsy, pulsatile bruit Low-flow left CCF Left superior ophthalmic vein, no cortical venous drainage + Spontaneous closure CCF, carotid occlusion Remaining VI palsy; 4 mo 9/F/74 Bilateral exophthalmus and ophthalmoplegia, decreased vision, pulsatile bruit Intermediate-flow right CCF Bilateral superior ophthalmic vein, minor cortical venous drainage + Coiling aneurysm + carotid artery Remaining right VI palsy; 7 mo 10/M/65 Left exophthalmus and ophthalmoplegia, vision 0 left, pulsatile bruit High-flow left CCF Left superior ophthalmic vein + Coiling aneurysm + carotid artery Enucleation left eye; 38 mo 11/F/59 Pulsatile bruit, left temporal hemorrhage ×2 High-flow right CCF Major cortical venous drainage Not done None Death Note:—+ indicates tolerance; −, nontolerance.





{kind=link}
{kind=link}
{kind=link}