
Article Figures & Data
Figures
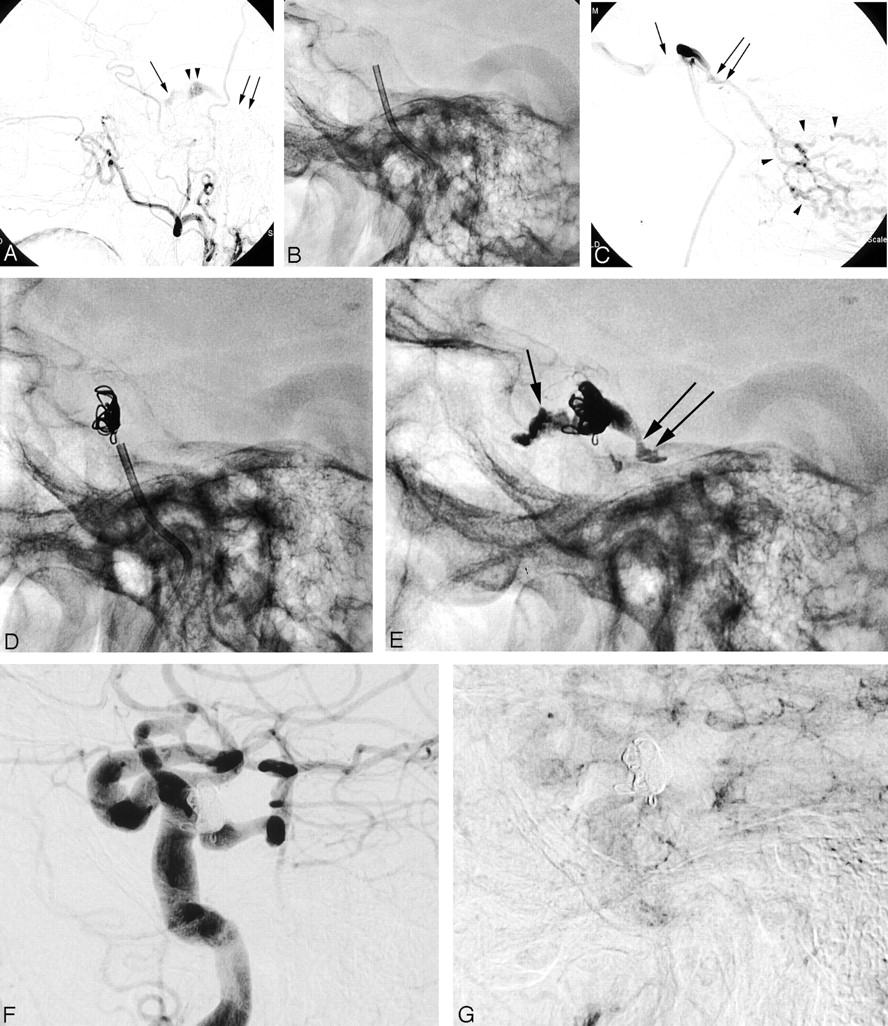
- Fig 1.
Ninety-one-year-old woman (case 10 [Table 1]), 2 months after radiation therapy for nasopharyngeal carcinoma develops a slowly progressive right orbital swelling, chemosis, proptosis, and ophthalmoplegia. Angiogram shows a CCF with mixed dural artery supply via both ECA (type C, ref. 2). There is a retrograde venous drainage via the right ophthalmic vein and right cerebellar cortical veins. A transvenous n-BCA embolization combined with coils was carried out with successful dural CCF obliteration and complete clinical recovery.
A, Right lateral ECA angiogram shows incomplete filling of the CS (arrowheads) and SOV (straight arrow). Discrete retrograde filling of the congested anterior cerebellar vein is noted (double arrows). Note there is no filling of the IPS.
B, Placement of a 5F guide catheter over a wire through the obliterated IPS into the posterior-lateral segment of the CS.
C, Right lateral CS venogram shows a proximal stenosis of the congested SOV (arrow) as source for the clinical symptoms and filling of cerebellar cortical veins (arrowheads) via proximal superior petrosal vein (double arrow). Note the guide catheter is occlusive within the IPS.
D, Lateral radiograph shows several coils placed in the CS for flow reduction and to protect acrylate spillage into SOV and anterior cerebellar veins.
E, Lateral radiograph shows coils and n-BCA-Ethiodol cast of the entire CS segment depicted in panels A and C, proximal SOV (arrow), and the superior petrosal vein (double arrow).
F and G, Early- and late-phase right lateral CCA angiograms show CCF obliteration.
- Fig 2.
Eighty-seven-year-old woman (case 4, Table 1) presented with progressive ophthalmoplegia, decreased visual acuity, and chemosis. Angiogram shows a CCF with bilateral mixed dural artery supply both via the external and internal carotid arteries (type D, ref. 2), congestion of both cavernous segments with retrograde flow in both SOV. A transvenous embolization was carried out by using n-BCA with complete CCF obliteration and cure of symptoms.
A–D, Early- and late-phase right lateral and frontal ICA angiograms show slow contrast filling (A, thin double arrow) through dural branches of the ICA (A, arrow) including capsular arteries of McConnell at the floor of sella turcica. Retrograde filling of the SOV (arrowhead) with origin stenosis (B and C, double arrows). Note delayed contrast washout (B–D, arrows) of the CS bilaterally.
E and F, Frontal and lateral radiographs show the microcatheter in the left cavernous segment (arrow) before n-BCA infusion. Microcatheter was navigated through the SOV (double arrow) and the anterior intercavernous connection (arrowhead).
G and H, Frontal and lateral radiograph show the n-BCA-Ethiodol cast within the CS bilaterally. Some embolic material spillage is seen in the right proximal SOV through the stenotic segment (arrow). Note the radiolucent structures within the glue cast represent the internal carotid arteries.
I–L, Left lateral early and late phase ICA angiograms (I and J) and right and left frontal angiogram show CCF obliteration. Note artifacts related to the embolic material (arrows).
- Fig 3.
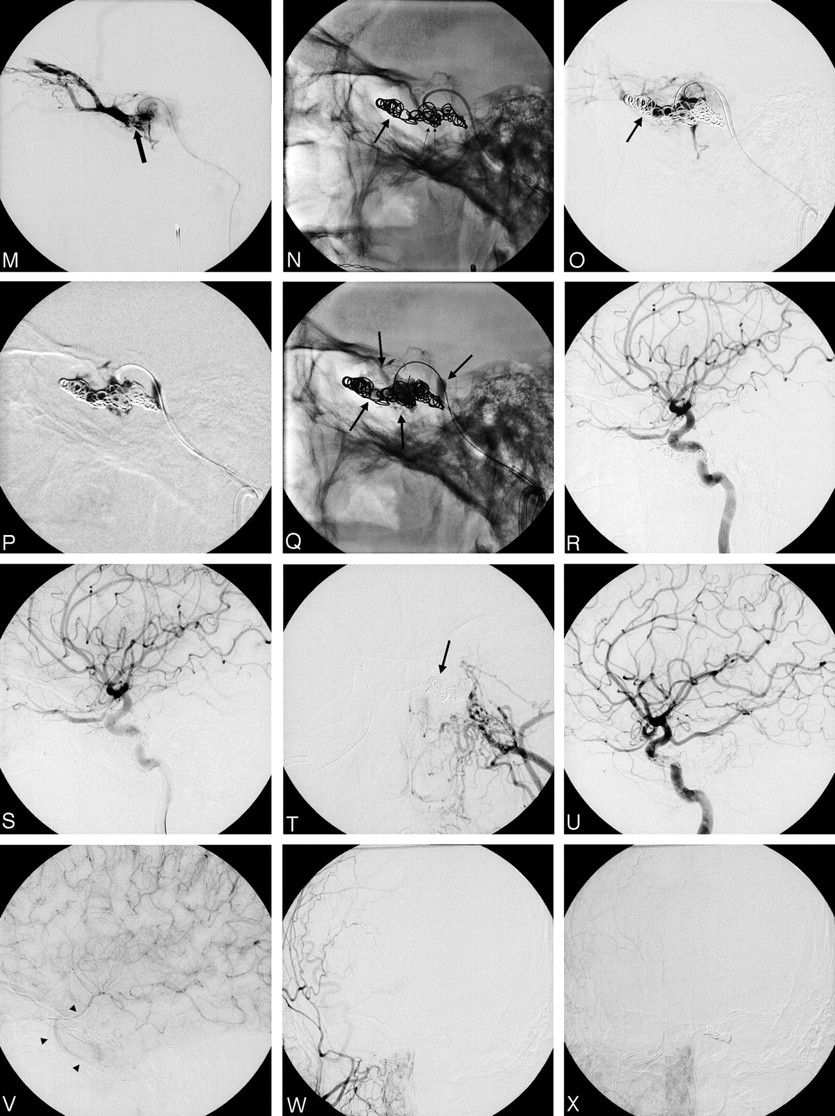
Forty-four-year-old man (case 14 [Table 1]) develops a slowly progressive bilateral chemosis and proptosis. A transvenous n-BCA embolization combined with platinum coils was carried out with successful CCF obliteration and clinical recovery.
A–J, Early and late right ICA lateral (A and B), right ECA frontal (C and D), left ICA frontal and lateral (E–I), and left ECA frontal (J) angiograms show a CCF with mixed bilateral (left > right) dural artery supply via both ECA and ICA (A, B, E, F, G, arrows, Type D-2, ref. 2). There is an early venous drainage via both IPS (D, arrows; I, double arrow), both SOVs (right > left; I, small arrowheads), and the right sphenoparietal vein (F, H, I, arrowheads). Marked dilation of the right CS segment as compared with the left (F and H, small arrows) with prominent “radiolucent” ICA boundaries (F and J).
K and L, Superselective catheterization of the left CS segment through the right IPS and microcatheter tip placement into the anterior-medial segment (arrow). The microcatheter injection shows retrograde filling of both congested SOVs (small arrowhead and small arrows) and the right sphenoparietal vein (arrowheads).
(Continued)M, The microcatheter tip is placed further into the left common ophthalmic vein (arrow).
N, Placement of platinum coils into the common ophthalmic vein (arrow) and cavernous sinus to reduce flow in CS and protect acrylate spillage.
O, Microcatheter control angiography shows filling of the cavernous sinus and the common ophthalmic vein (arrow), but sparse filling of SOV.
P and Q, Acrylate infusion under plain roadmap with casting of the cavernous sinus. Note n-BCA is contained within the coil mass, no spillage into SOV (arrows).
R–X, Bilateral ICA and ECA early and late control angiography shows CCF obliteration with antegrade filling of the sphenoparietal vein and slow outflow (V, arrowheads).
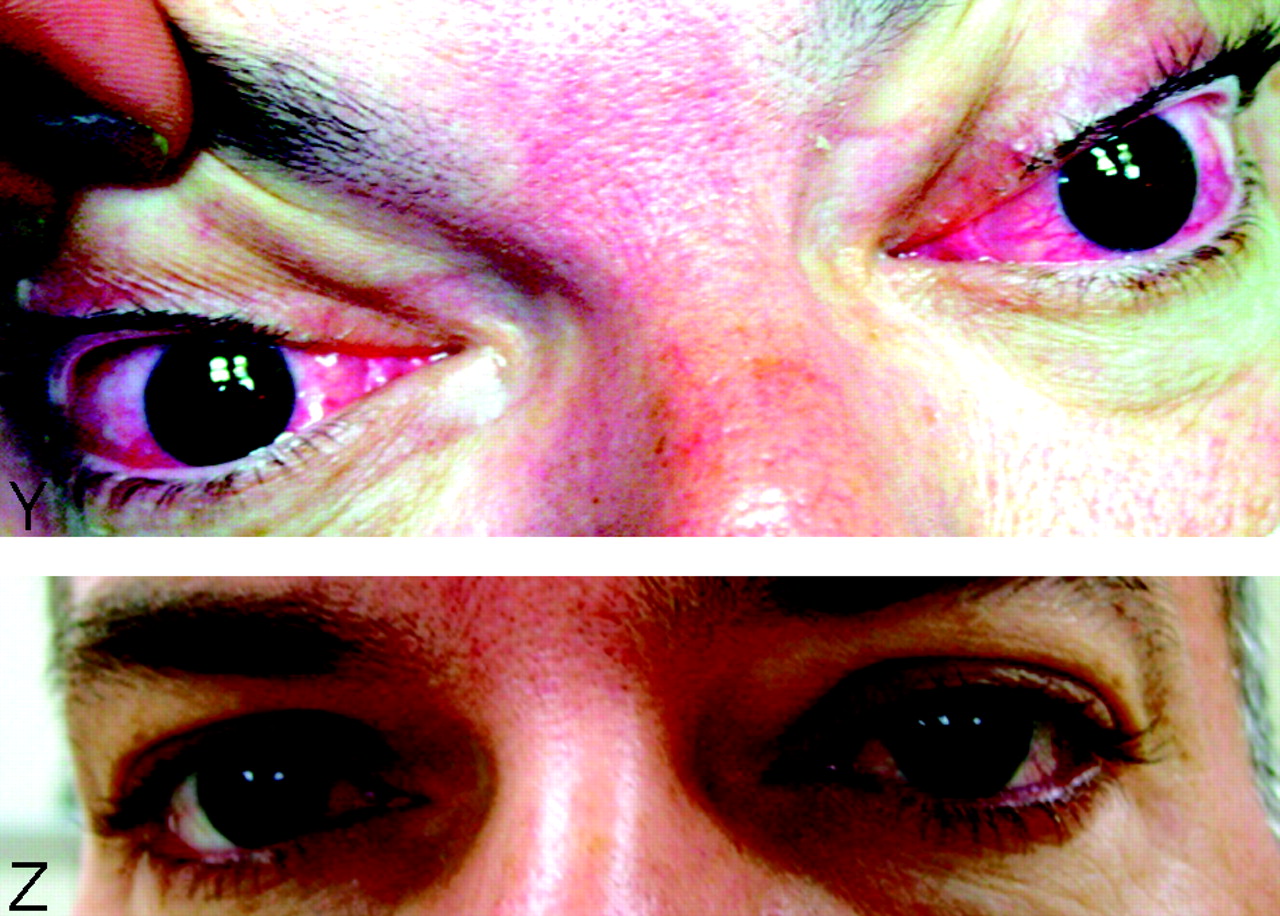
(Continued) Y and Z, Chemosis and conjunctivitis before treatment. Near-complete resolution 2 weeks after CCF obliteration.





Tables
Patients with dural carotid cavernous fistulas: clinical data and endovascular techniques
Patient No./Age (y)/Sex Clinical Presentation Type* Approach Embolic Material Angiography Obliteration† Clinical Outcome Complications 1/41/F Chemosis, proptosis D SOV percutaneous/IPS/IMAX n-BCA (TV), PVA (IMAX) Yes Cure n-BCA droplet escaped via the fistula into MCA, no branch occlusion; no clinical sequelae 2/70/M Chemosis, decreased visual acuity B SOV percutaneous n-BCA (TV) Yes Cure No 3/56/M Chemosis, ophthalmoplegia D-2 IPS transfemoral n-BCA (TV) Yes Cure Initial worsening of cranial nerve VI palsy, but progressive improvement 4/87/F Chemosis, decreased visual acuity, ophthalmoplegia D-2 SOV transfemoral n-BCA (TV) Yes Cure n-BCA spillage into SOV without clinical sequelae 5/45/M Chemosis, proptosis, decreased visual acuity D-2 SOV transfemoral IMAX Coils/n-BCA (TV), n-BCA (TA) Yes Cure Microcatheter perforation of IPS, no sequelae 6/93/F Chemosis, pain B IPS transfemoral Coils/n-BCA (TV) Yes Cure No 7/82/M Chemosis B IPS transfemoral n-BCA (TV) Yes Cure No 8/35/F Chemosis, ophthalmoplegia C IPS transfemoral IMAX Coils/n-BCA (TV), n-BCA (IMAX) Yes Cure No 9/54/M Chemosis, proptosis B IPS transfemoral n-BCA (TV) Yes Cure No 10/91/F Chemosis, proptosis, ophthalmoplegia C-2 IPS transfemoral Coils n-BCA (TV) Yes Cure No 11/60/F Chemosis, proptosis, ophthalmoplegia D-2 IPS transfemoral Coils in SOV n-BCA (TV) Yes Cure No 12/65/F Chemosis, proptosis, ophthalmoplegia D IPS transfemoral Coils in SOV n-BCA (TV) Yes Cure No 13/60/F Chemosis, proptosis D IPS transfemoral n-BCA (TV) Yes Cure No 14/44/M Chemosis, proptosis D IPS transfemoral Coils/balloon-assisted n-BCA (TV) Yes Cure No Note.—C-2 indicates bilateral; D-2, bilateral; IPS, inferior petrosal sinus; n-BCA, n-butyl-cyanoacrylate; SOV, superior ophthalmic vein; TA, transarterial; TV, transvenous; IMAX, internal maxillary artery.
* From Barrow et al (2).
† Patient no. 3 had a follow-up angiography because of an initial worsening of symptoms, but demonstrated obliteration. Patients nos. 6 and 9 had tiny residual filling of the dCCF as seen on immediate posttreatment angiograms, but showed obliteration at 6-month follow-up study.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Mid- and long-term outcomes of carotid-cavernous fistula endovascular management with Onyx and n-BCA: experience of a single tertiary center
- Intracranial Dural Arteriovenous Fistulae: Clinical Presentation and Management Strategies
- Surgical access on the superior ophthalmic vein to the cavernous sinus dural fistula for embolization
- Use of Onyx for Transarterial Balloon-Assisted Embolization of Traumatic Carotid Cavernous Fistulas: A Report of 23 Cases
- Onyx 18 embolisation of dural arteriovenous fistula via arterial and venous pathways: preliminary experience and evaluation of the short-term outcomes
- Brain Aneurysms and Arteriovenous Malformations: Advancements and Emerging Treatments in Endovascular Embolization