
Abstract
Summary: We report a case of a ruptured aneurysm of the anomalous cerebellar artery originating from internal carotid artery presenting with a carotid cavernous fistula (CCF). An initial angiogram showed the typical appearance of a CCF with a direct fistulous tract with focal aneurysmal dilation from the ascending cavernous segment of the right internal carotid artery. A postembolization angiogram of the right internal carotid disclosed the anomalous cerebellar artery originating from the fistula point of the internal carotid artery.
Anomalous cerebellar arteries originating from the internal carotid artery are very rare and are considered persistent trigeminal artery variants. Persistent trigeminal artery is the most frequently encountered persistent carotid-vertebrobasilar anastomosis, usually anstomosing between the internal carotid artery and the basilar artery. The persistent trigeminal artery variant rarely represents as an anomalous origin of the cerebellar artery from the internal carotid artery and seems to occur as the result of the persistence of a primitive trigeminal artery associated with an incomplete fusion of the longitudinal neural arteries (1). Spontaneous or traumatic fistula from the persistent trigeminal artery to the cavernous sinus and its endovascular treatment has rarely been reported (2–7). To the best of our knowledge, however, carotid cavernous sinus fistula (CCF) caused by a ruptured aneurysm of the cerebellar artery at its anomalous origin has not been reported.
We present a case in which the initial carotid angiogram showed the typical appearance of a CCF without opacification of any variant artery and postembolization carotid angiogram revealed complete disappearance of the fistula with opacifiation of an anomalous cerebellar artery from the fistula point of the internal carotid artery, which supplied the inferior hemisphere of right cerebellum.
Case Report
A 40-year-old previously healthy man without any medical history presented with a sudden onset of a severe headache and a pulsatile bruit in his right ear. Right 6th cranial nerve palsy developed 2 days later. The patient denied any history of minor trauma. Brain MR imaging revealed only ventriculomegaly. Towne’s view of right internal carotid artery angiogram showed the typical appearance of a CCF with its main venous drainage through the intercavernous sinus and both inferior petrosal sinuses (Fig 1A). A lateral and an oblique magnified view of the right internal carotid angiogram with carotid artery compression revealed a small fistulous tract originating from the ascending cavernous segment of right internal carotid artery. The fistulous tract revealed focal aneurysmal dilation in close association with the inferior portion of the right cavernous sinus (Fig 1B, -C).

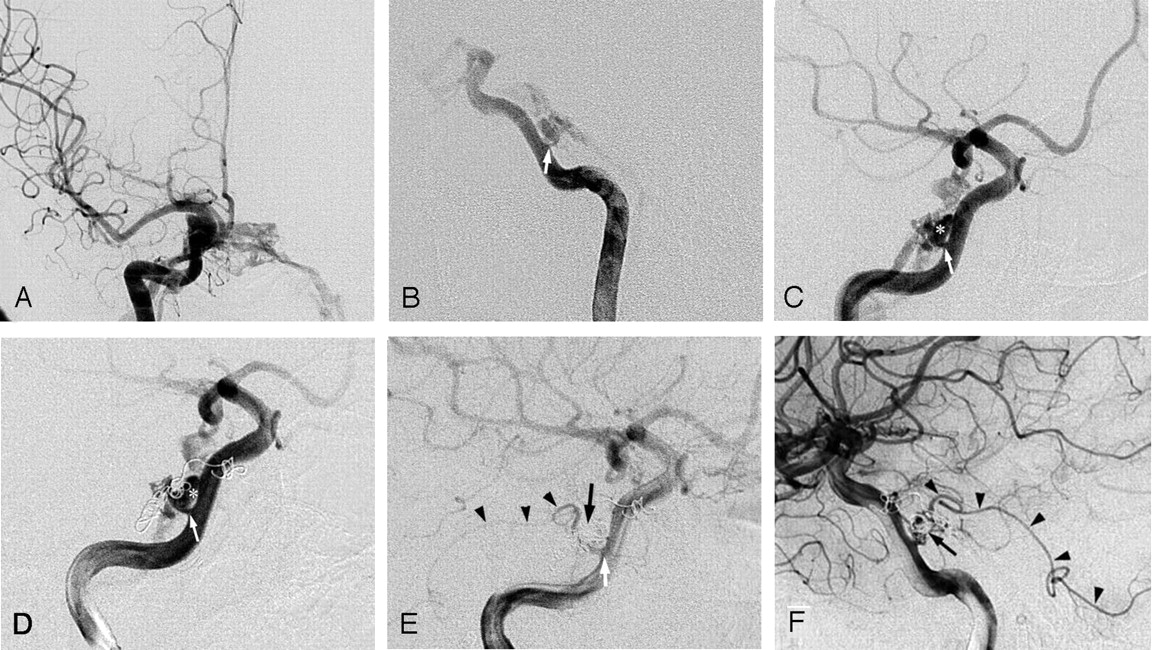
A, Initial Towne’s anteroposterior view of right internal carotid angiogram showing the typical appearance of a CCF with main venous drainage through intercavernous sinus and both inferior petrous sinuses.
B and C, Lateral and magnified oblique view revealing a single fistulous tract (white arrow) between right internal carotid artery and cavernous sinus. The aneurismal dilatation (asterisk) of the fistula, which was first opacified at an early arterial phase, was closely associated with the inferior aspect of right cavernous sinus.
D, The flow of the CCF never decreased after embolization of the pouch of right cavernous sinus near the fistulous tract by using three coils by venous approach.
E and F, After coil embolization of the aneurysmal dilatation of the fistula (black arrow) by arterial approach with the same setting, immediate postembolization oblique and lateral angiograms showed complete occlusion of the CCF and disclosed the anomalous cerebellar artery originating from the fistula point of right internal carotid artery (arrowheads), which supplied the inferior hemisphere of right cerebellum.
Endovascular treatment was performed 2 days later. First, endovascular coil embolization was attempted through the venous approach. After embolization of the right cavernous sinus pocket near the fistulous tract by using one detachable coil and two fibered platinum coils (Boston Scientific, Watertown, MA), there was no decrease in the flow through the fistulous tract (Fig 1D), so embolization by venous approach was abandoned and an arterial approach was attempted to directly select the fistulous tract through the right internal carotid artery. By right femoral arterial access with the same setting, a 6F guiding catheter (Envoy; Cordis, Miami, FL) was positioned to the cervical segment of the right internal carotid artery. The fistulous tract was selected by using a microcatheter (Renegade; Boston Scientific) and a 0.014-inch guidewire (Transcend; Boston Scientific) by using the coaxial technique, although it was impossible to advance the microcatheter into the cavernous sinus beyond the aneurysmal dilation of the fistulous tract. The aneurysmal dilation of the fistulous tract was embolized with Guglielmi detachable coils (Boston Scientific). A postembolization right internal carotid angiogram showed complete occlusion of the CCF and disclosed an anomalous cerebellar artery, which was not opacified at the initial angiogram, originating from the fistulous point of the right internal carotid artery and supplying the inferior hemisphere of the right cerebellum (Fig 1E, -F). The patient recovered completely from the symptoms of headache, fulsatile tinnitus, and right 6th nerve palsy soon after the treatment. The clinical course was uneventful until discharge and further clinical follow-up at 6 months.
Discussion
Direct CCFs are included among type A fistulas according to Barrow’s classification. Etiologically, most dissecting CCFs are traumatic, but less commonly they may be spontaneous. Spontaneous direct CCFs are usually caused by rupture of an intracavernous carotid aneurysm, and aneurysmal CCFs account for about 20% of direct CCFs (8).
Spontaneous or traumatic CCF from the persistent trigeminal artery to the cavernous sinus and its endovascular treatment has rarely been reported (2–7). To the best of our knowledge, however, CCF caused by a ruptured aneurysm of the anomalous cerebellar artery has not been reported.
The cerebellar artery originating from the internal carotid artery was first reported by Teal et al (9). The level of the internal carotid artery from which these vessels took origin led to the conclusion that they were persistent trigeminal artery variants (1, 11). Unlike the usual persistent trigeminal artery that has a direct communication with the basilar artery, the persistent trigeminal artery variant with direct communication between the internal carotid artery and the cerebellar artery without interposition of the basilar artery has rarely been reported (1, 11).
The persistent trigeminal artery is the most common fistulous connection among the persistent embryonic vascular anastomosis connecting the developing carotid arteries and the longitudinal neural arteries. It connects the cavernous segment of the internal carotid artery with the basilar artery. The persistent trigeminal artery originates from the internal carotid artery at the point where this vessel leaves the carotid canal and penetrates the cavernous sinus. From this point, the artery takes a posterior course, sometimes inclining rostrally slightly, through the cavernous sinus. Therefore, if an aneurysm located at the junction of the persistent trigeminal artery-internal carotid artery ruptures, or if spontaneous or traumatic rupture of the persistent trigeminal artery occurs near its anomalous origin, CCF may result. This hypothesis is supported by several previous reports that the persistent trigeminal artery was associated with a CCF (2–7).
Rupture of the cerebellar artery near its anomalous origin may be a possible explanation in our case; however, the spontaneous development of the patient’s symptoms, initial opacification of the aneurysmal segment of the fistula, and the opacification of the anomalous cerebellar artery after embolization of the aneurysmal segment of the fistula suggest that an aneurysm of the cerebellar artery might have existed previously.
Conclusion
This may be the first case of a ruptured aneurysm of the anomalous cerebellar artery originating from the internal carotid artery, a so-called persistent trigeminal artery variant, presenting with a typical appearance of CCF, diagnosed after successful endovascular treatment. If a patient presents with a sudden onset, spontaneous CCF without any history of trauma and selective angiogram reveals a small fistulous connection between internal carotid artery and cavernous sinus at the ascending cavernous segment, one should consider the possibility of ruptured aneurysm of the anomalous cerebellar artery originating from the internal carotid artery.
References
- Received May 25, 2004.
- Accepted after revision July 17, 2004.
- Copyright © American Society of Neuroradiology





{kind=link}