
Abstract
Summary: We present a case report of a patient presenting with persistent aphasia for 1 week and cerebral hypoperfusion documented by single-photon emission tomography, both of which resolved completely after successful angioplasty of the symptomatic artery. This case represents a rare clinical example of “limping brain syndrome.”
Cerebral hypoperfusion that causes neurologic deficits lasting >24 hours is invariably associated with infarction on brain imaging. We present the case of a patient with persistent aphasia that fluctuated over 1 week, left middle cerebral artery (MCA) stenosis, and hypoperfusion of the left MCA territory documented by single-photon emission tomography (SPECT). The patient underwent angioplasty of the left MCA, and his aphasia resolved. Repeat SPECT showed resolution of left MCA territory hypoperfusion, and follow-up MR imaging brain showed no infarct. We present this case as a rare clinical example of “limping brain syndrome.”
Case Reports
A 77-year-old right-handed man from Florida was transferred to Emory University Hospital with episodes of speech disturbance. These episodes had been occurring almost daily for the past month and consisted of difficulty finding words and slurring of speech lasting <30 minutes.
Past medical history included hypertension, congestive heart disease, and coronary artery bypass surgery. He had a 15-pack year smoking history but had quit smoking 30 years ago. Medications included Enalapril, Atenolol, Lasix, and Digoxin.
His neurologic examination revealed occasional word-finding difficulty and mild short-term memory loss, but was normal otherwise. Review of an outside angiogram showed high-grade left MCA stenosis. Intravenous heparin and warfarin were initiated.
Five days later, when the International Normalized Ratio (INR) was 2.2, the patient developed aphasia consisting of word-finding problems, paraphasic errors, and difficulty writing and spelling. Intravenous heparin was reinitiated, and the patient was transferred to the intensive care unit, where he was kept in a supine position and a mean arterial pressure of 120 mmHg was targeted.
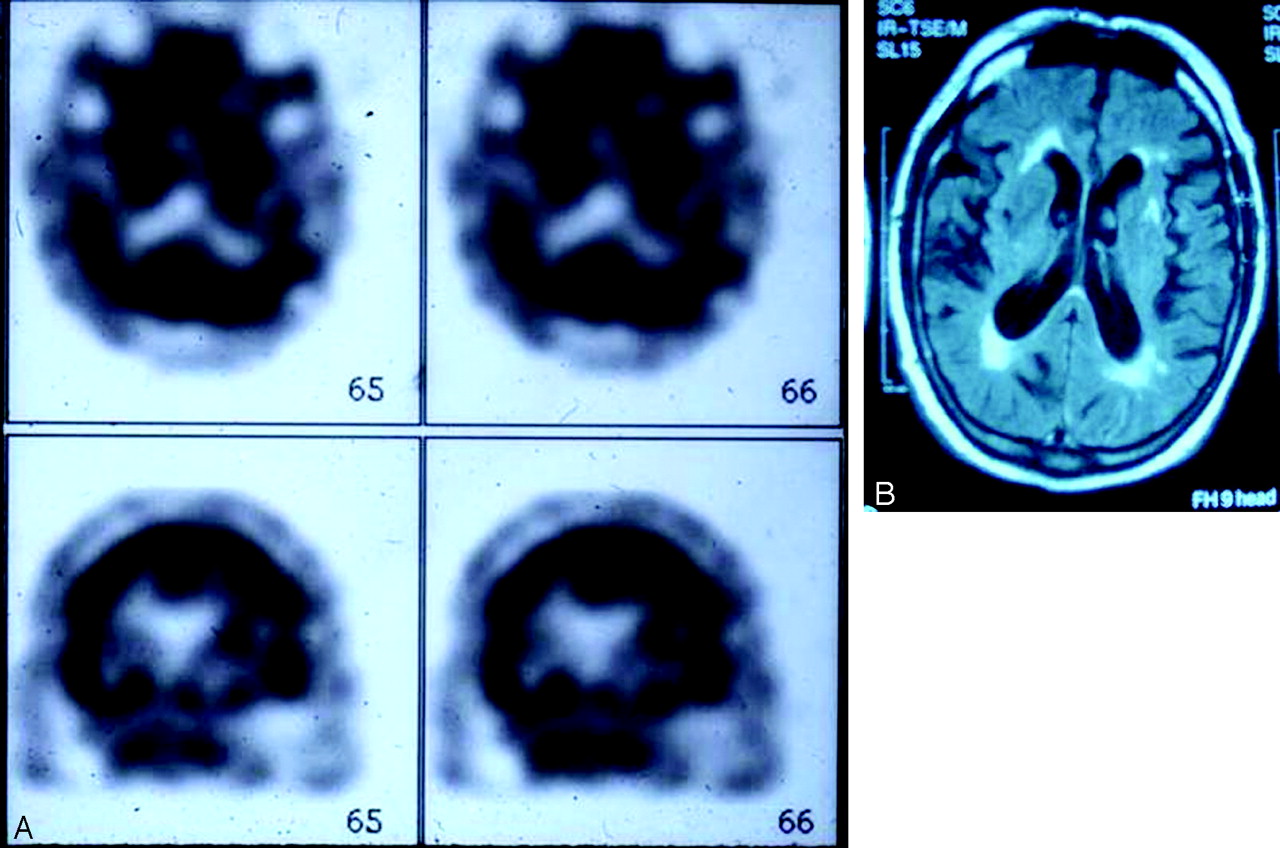
Despite these measures, the patient’s aphasia persisted, although it fluctuated in severity, over the next week. During this period, a SPECT scan showed decreased perfusion in the left MCA territory (Fig 1A), and an MR image showed moderate periventricular white matter changes but no infarct in the left MCA territory (Fig 1B). At the time, diffusion-weighted imaging was not available.

A SPECT scan (A) shows decreased perfusion in the left MCA territory and MR image (B) shows moderate periventricular white matter changes but no infarct in the left MCA territory.
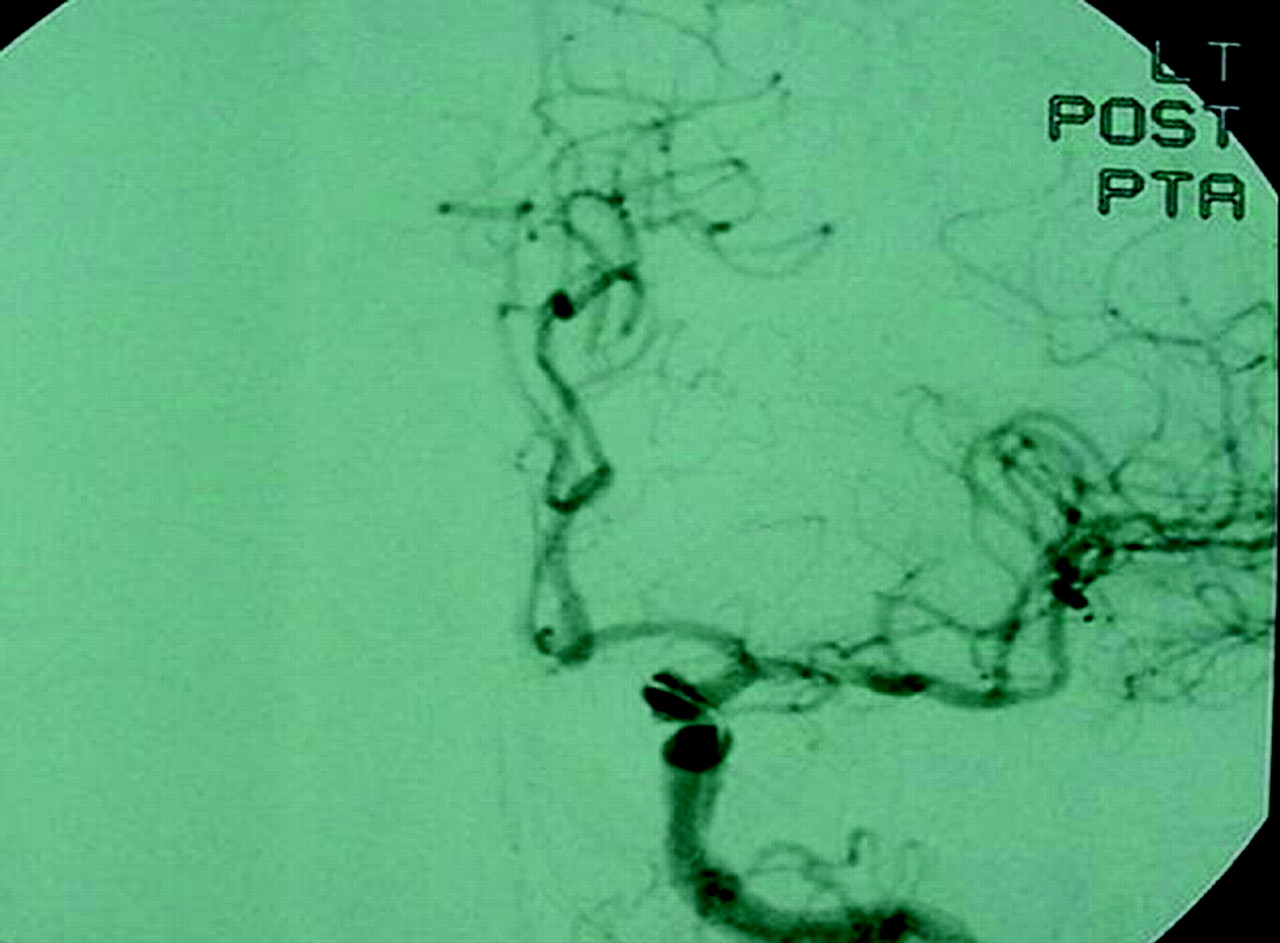
Because of persistent aphasia, angioplasty of the left MCA was planned. The preangioplasty angiogram showed severe stenosis of the M1 segment of the left MCA (Fig 2A) with delay in filling of the left MCA branches compared with the left anterior cerebral artery (ACA) branches (Fig 2B, C). In addition, there was poor collateralization between the pial branches of the left ACA and left MCA (Fig 2C, D). Left MCA angioplasty was performed, which resulted in moderate improvement in the severity of stenosis and marked improvement in flow in the MCA territory (Fig 3). Immediately after the procedure, the patient was mute, but 2 hours later the severity of aphasia was similar to the preprocedure level. The following day, the patient’s aphasia had resolved, a repeat SPECT scan showed normal perfusion in the left MCA territory (Fig 4A), and MR imaging showed no infarct in the left MCA territory (Fig 4B). The patient was discharged on warfarin, returned to Florida, and did not return for follow-up.

Preangioplasty angiogram (A) shows severe stenosis of the M1 segment of the left MCA. Angiograms (B and C) show a delay in filling of the left MCA compared with those of the left ACA; angiograms (C and D) also show poor pial collateralization between left ACA and left MCA branches.

Postangioplasty angiogram shows moderate improvement of left MCA stenosis.

Postangioplasty SPECT scan (A) shows normal perfusion in MCA territory and MR image (B) shows no MCA infarct.
Discussion
Cerebral blood flow (CBF) in man is approximately 50 mL/100 g brain tissue/min (1). Reduction of CBF to 18 mL/100 g brain tissue/min causes slowing of electroencephalographic waveforms (2). Further reduction of CBF to 15 mL/100 g brain tissue/min suppresses somatosensory-evoked responses (3). Thus, the threshold of electrical failure is quantified at 15–18 mL/100 g brain tissue/min.
Recent studies have shown reduced cerebral blood flow further to 10–12 mL/100 g brain tissue/min leads to release of glutamate and rapid depletion of ATP. This results in failure of the Na/K ATPase pump (4), an influx of sodium, calcium, and chloride (5) into neurons, and an increase in extracellular potassium concentration (6, 7). In addition to this ionic failure of the neurons, there is a rise in intracellular lactic acid concentration due to anaerobic metabolic state (8).
Between these two thresholds of electrical and ionic failure, there exists a small range of CBF at which neuronal membrane structure and homeostasis are maintained despite functional loss (9). For want of a better description, we refer to this state as the “limping brain.” When this state exists on the periphery of infarcted brain tissue, the periphery is usually referred to as the “ischemic penumbra,” which has the potential for recovery (10).
We present our patient as a rare clinical example of “limping brain” syndrome. He experienced aphasia lasting a week in association with hypoperfusion on SPECT, both of which resolved after left MCA angioplasty. The absence of an infarct on MR imaging after this prolonged episode of aphasia and the fluctuating course argue strongly against the possibility that the aphasic episode was the result of a stroke in the left MCA territory, from which he recovered in a week. Epilepsy partialis continua that was induced by hypoperfusion is another consideration, but the fluctuating course over 1 week and involvement of language rather than the motor system would be atypical for that condition. Rather, the evidence in this case suggests that the functional loss of neurons in the left MCA territory (i.e., the aphasia) was a result of a fall in focal CBF to a level that was between the two thresholds of electrical and ionic failure. Once focal CBF normalized after left MCA angioplasty, the aphasia resolved, which suggests that there had not been any permanent insult to the structural integrity and homeostatic function of the ischemic neurons.
A limitation of this case report is our reliance on SPECT for qualitative CBF measurements. Our conclusion would have been better supported if quantitative measurements of CBF and tissue oxygen metabolism using positron-emission tomography had been performed.
References
- Received May 25, 2004.
- Accepted after revision August 17, 2004.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.