
Abstract
Summary: The radiologist needs to be aware of a potential pitfall that can influence the imaging appearance of thyroid goiter. Whether the patient is imaged with the arms overhead or by the side may affect the apparent mediastinal excursion of a goiter. CT scans obtained with the patient’s arms by the side are more accurate for determining substernal extent of goiter than when the arms are overhead, a position usually used in chest CT. Ultimately, this difference in imaging technique may have a profound effect on the adjacent structures impacted by the goiter and may influence the planned surgical approach.
Radiologic evaluation plays a critical role in the preoperative assessment of large goiters and other thyroid masses, and the radiologist must be aware of the information the surgeon seeks to provide useful guidance for surgical planning. We have noted that whether a patient is imaged with the arms overhead or by the side may affect the apparent mediastinal excursion of a goiter. This difference in excursion and the resulting apparent localization can alter the planned surgical approach with regard to whether a sternotomy or thoracotomy is necessary.
Description of Technique
CT scans of 15 patients who had both neck and chest CT and a preexisting or subsequent diagnosis of goiter were retrospectively reviewed by two board-certified radiologists. There were 13 women and 2 men, ranging in age from 37 to 84 years. Thirteen of the 15 were studied specifically for thyroid dysfunction, and symptoms included dysphagia and neck mass. Two of the 15 had neck and chest CT scans for indications unrelated to thyroid gland. All patients had both dedicated neck and chest CT at the same time. Neck CT technique was performed by using section thickness of 2.5 mm, kv 140, maS 190, and 100 mL of nonionic IV contrast at 2 mL/s with a 40-second delay. Chest CT was performed either by using section thickness of 0.625 mm (for high-resolution reconstructions to evaluate interstitial lung disease) or 1.25 mm, kv 140, maS 190, and 100–150 mL of nonionic intravenous contrast. Dedicated chest CT imaging was performed with the patient’s arms overhead in an attempt to avoid beam-hardening artifact from the shoulders. Dedicated neck CT imaging was performed with the arms by the side. Images were retrospectively evaluated by two board-certified radiologists who assessed goiter size, heterogeneity, and effect on local soft tissue and vascular structures. The clavicular heads were used as an easy and reproducible objective landmark for measuring the lowest extent of goiter within the mediastinum and serving as a point for comparison.
Results
Seven patients demonstrated a 1–1.5-cm discrepancy between the two techniques, with the apparent retrosternal extent of the goiter lower when the arms were overhead. Four had a 1.5–3.2-cm discrepancy, with the enlarged thyroid glands extending further substernally on the dedicated chest imaging. One demonstrated a 3.3-cm discrepancy between the two techniques (Fig 1). Three scans showed <5-mm difference in substernal excursion of the goiters. In three patients, the goiter extended substernally on the chest technique but not on the neck technique.

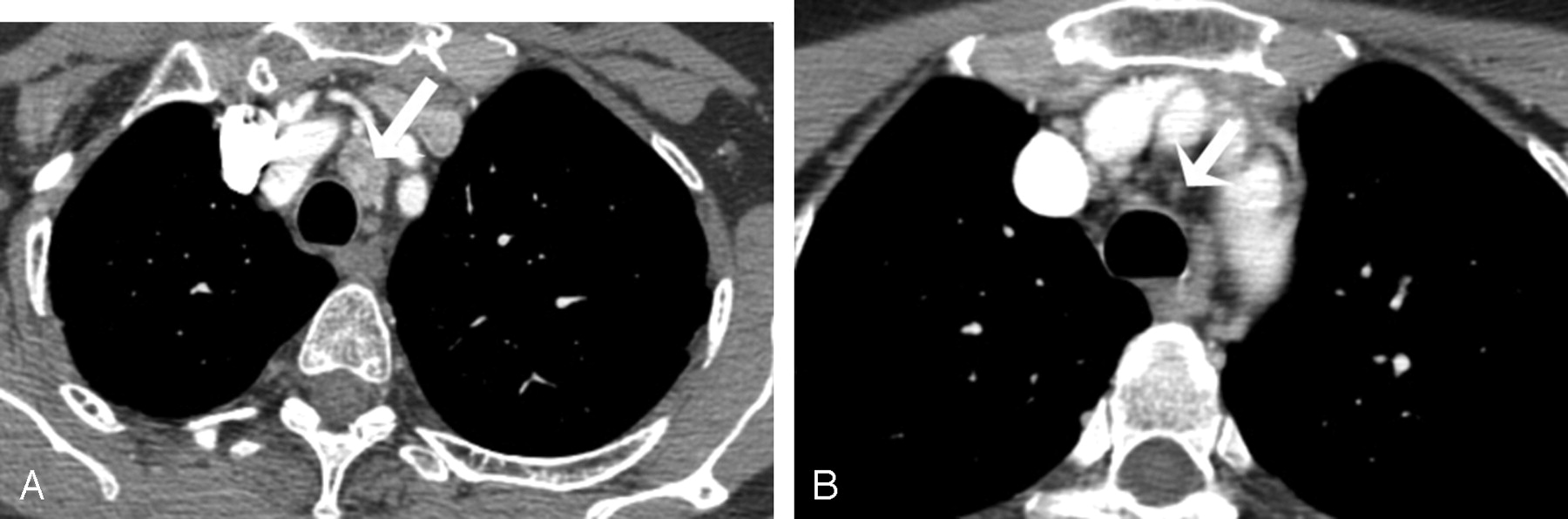
Use of the chest technique with arms above the head (A) demonstrates clear substernal extension of goiter (arrow). By contrast, use of the neck technique with arms by the sides (B) demonstrates no substernal extension of goiter (arrow).
Discussion
Surgical intervention is generally regarded as the treatment of choice for most substernal goiters. Patients may present for cosmetic reasons, or symptoms such as mild dyspnea, dysphagia, or hoarseness. Serious life-threatening complications, such as airway obstruction and neurovascular compression, can arise suddenly, usually secondary to intrathyroid bleeding from trauma or infection (1). In addition, substernal goiters have a relatively high malignancy rate (7–17%), and fine-needle aspiration can be difficult to accomplish on a substernal mass (2). Fine-needle aspiration is also subject to sampling error that can lead to a false-negative result. Most substernal goiters descend to one side of the trachea or the other and are found in the anterior mediastinum. The airway can become trapped between the sternum and upper thoracic spine in a centrally located mass. More posterior-oriented substernal goiters can displace the normal path of the recurrent laryngeal nerve, particularly on the left as it traverses the posterior aspect of the aortic arch. Severe mass effect on vascular structures can lead to findings of superior vena cava syndrome. Finally, goiters can also demonstrate more cephalad extension with exertion of mass effect on cervical vascular and airway structures.
Most anterior substernal thyroid goiters are accessed via a transcervical approach. On the basis of imaging findings, the surgeon will decide whether to perform a total thyroidectomy, subtotal thyroidectomy, or thyroid lobectomy with or without isthmusectomy (3). A 3–4-inch incision is made in the low collar area of the neck above the clavicles and sternum. The strap muscles are divided in the midline and retracted to expose the cervical aspect of the thyroid gland. The gland is explored manually with blunt digital dissection, carefully exposing the substernal portions of the goiter. Fragmentation of the goiter is avoided and attention is given to not violating the course of the recurrent laryngeal nerve resulting in postsurgical vocal cord paralysis (4). For goiters that cannot be removed via neck dissection, such as those goiters with complicated anatomic extensions or posterior mediastinal involvement, the surgeon may need to incorporate a partial upper sternotomy and clavicular head resection or minithoracotomy for adequate exposure.
Surgeons have long been familiar with the impact when a patient with a large thyroid goiter simultaneously raises both arms overhead. Pemberton sign or “thyroid cork” describes the physical manifestation of marked facial plethora resulting from jugular vein compression when the thoracic inlet rises so that it is temporarily filled by a large substernal goiter (5). Although elevating the patient’s arms and shoulders above the head is desirable to eliminate the beam-hardening artifact from the shoulders, it may also have the adverse consequence of temporarily increasing the apparent descent of a substernal goiter.
The clavicular heads can serve as a useful landmark for comparison of the pertinent anatomy on the dedicated neck and chest CT imaging (Fig 2). Another useful method for comparison entails by using patient specific findings such as calcification in a vessel or a lymph node for comparison. A surgeon who follows a radiologic interpretation of a substernal thyroid goiter given from a dedicated chest CT technique might perform a sternotomy instead of a simple low-collar incision for resection of a substernal goiter. Therefore, patients with substernal thyroid goiters should be evaluated by using dedicated neck CT technique with the patient’s arms by the sides. Ultimately, recognizing this potential pitfall can improve both the quality and value of the radiologist’s contribution to patient care while also clarifying appropriate operative approaches.

A, At the level of the clavicular heads on chest technique images goiter with at least 180° of extension around the trachea (arrow). B, At the same level on neck technique does not image goiter (arrow).
Conclusion
The role of the radiologist in evaluation of substernal thyroid goiters is to provide the surgeon with an anatomic roadmap to guide surgical intervention. The radiologist provides an accurate account of the substernal extent of the mass and describes its impact on the trachea, esophagus, and vascular structures. Imaging the patient with the arms overheard can result in misleading substernal localization of the goiter. Substernal thyroid goiters should be imaged with the patient’s arms by the sides, because this is the position the patient will be in during surgery, and this position most accurately reflects the true anatomic location of the gland.
Footnotes
This technical note was presented as an educational exhibit at the 38th annual meeting of the American Society of Head and Neck Radiology, Philadelphia, September 29–October 3, 2004.
- Received November 8, 2004.
- Accepted after revision January 10, 2005.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.