
Abstract
Summary: We describe herein the use of MR fluoroscopic guidance in the drainage of abscess cavities. We percutaneously drained 12 brain abscesses in 11 patients. A 0.3T open MR imaging system was used. Sixteen drainages were performed in 12 abscesses. Repeat drainage was needed in three recurrences and one residual lesion. No serious complications were seen. MR fluoroscopy–guided percutaneous brain abscess drainage in an open MR imaging system is feasible.
Conservative treatment, craniotomy and abscess evacuation, stereotactic puncture, endoscopy, sonography, and CT-guided evacuation of abscesses have been described for treating intracerebral abscesses in the literature (1–3). The advent of open MR imaging systems, fluoroscopy software, and MR-compatible tools has contributed to minimally invasive procedures in a similar way, adding high temporal resolution and fast imaging techniques (4–7). We report our experience with the safety and efficacy of aspiration of the brain abscesses by using a freehand technique within an open MR imaging system.
Technique
Between April 2001 and January 2004, 12 brain abscesses were diagnosed in 11 patients (age range, 2–70 years; six male and five female) with CT or MR imaging. Presenting symptoms included headache, vertigo, seizures, hemiparesis, and signs of infection. Six patients were in poor condition. Two of them had meningitis. Surgery for a glial tumor had been performed in one patient, and another had surgery for a brain abscess concurrent with otitis media. The abscesses were located in the frontal lobe (four cases), occipital lobe (one case), parietal lobe (one case), temporal lobe (three cases), basal ganglia (one case), and subdural empyema (two cases). The abscesses were 1–8 cm in diameter (mean, 3.8 cm).
For real-time MR-guided interventions, an open-configuration 0.3T permanent magnet was used. Patients were in a supine position. Contrast-enhanced T1-weighted spin-echo images offered good visualization with a ring enhancement after injection of 0.2 mL/kg gadolinium (Dotarem, Guerbet, France).
Following the plan of entry point and appropriate trajectory by using two orthogonal laser beams and fish-oil capsules, the patient was moved from the MR imaging machine. A burr-hole craniotomy and incision of the dura were carried out using conventional drills, and surface vessels were electrocauterized in the operating room by a neurosurgeon (N.K.). In the cases of two patients, the holes had been already opened. Local anesthesia was used in five patients, and general anesthesia without endotracheal intubation was used in six patients. The patients were brought back into the magnetic field in the same position. The side of the head in which a lesion existed was placed in a standard ring-shaped surface coil, which allowed easy access. The coil was covered in a sterile fashion with a hole for imaging. The MR fluoroscopy sequence (spoiled gradient-echo, TR/TE, 15–20/4; acquisition, 1; FOV, 250 mm; flip angle, 30°; matrix, 92 × 256; section thickness, 5 mm; imaging time, 1 second; reconstruction time, 1 second) was started. An MR-compatible, 18-gauge, titanium Chiba fine needle (Cook, Bloomington, IN) was used. After the trajectory was verified by using the needle and the finger of radiologist (Ö.Ü.) (Fig 1), the needle was inserted and advanced along the planned pathway to the abscess capsule. The MR fluoroscopy images showed the tip of the needle, after reaching the capsule, it was gently perforated. The obturator inside the needle was retracted, and the needle was connected to a syringe. When the most suitable part of the lesion was reached, the drainage was accomplished under continuous image control and continued by the time outflow of purulent material ceased. The needle was withdrawn after the evacuation procedure. In a period of 3–5 minutes, the pus was evacuated (Figs 2, 3).

Trajectory of the finger helped to apply the angle of the needle during MR fluoroscopically guided intervention.

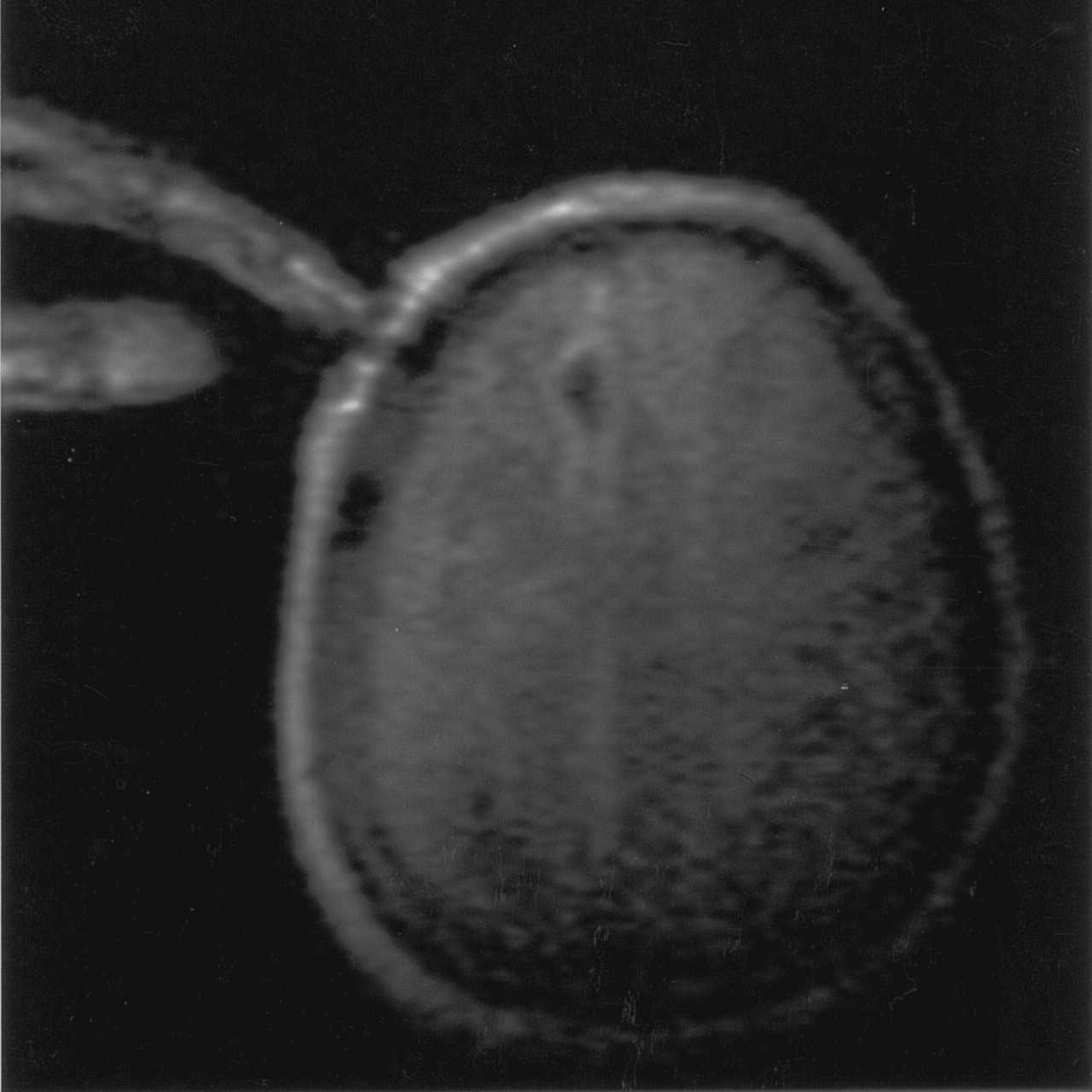
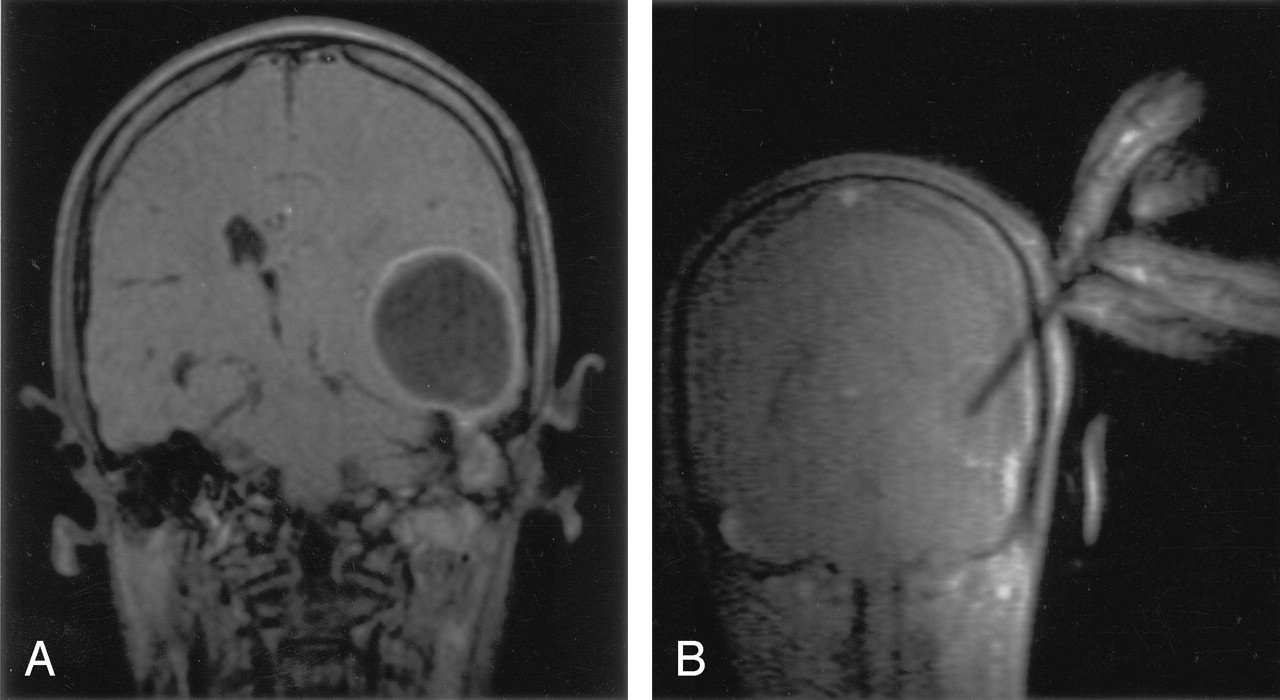
Contrast-enhanced coronal T1-weighted image shows a left temporal abscess and infection of the temporal bone (A). Image of the drainage seen during MR fluoroscopy image (B).

Contrast-enhanced coronal image demonstrates a subdural empyema in occipital localization (A). The needle has ruptured the capsule and is seen in the abscess cavity (B). The interhemispheric fissure is seen very close to tip of the needle, but it is intact. After the drainage, no pus is seen in the abscess localization (C).
While one radiologist (Ö.Ü.) was carrying out the intervention and watching the process on a television monitor placed at the entrance of the room, the other (M.E.S.) was checking the needle from the standard MR imaging monitor. The distance between the 20-inch television monitor and radiologist was nearly 2.5 m. The aspirate was sent to the laboratory for microbiological analysis and antibacterial sensitivity tests. The procedures took 40–80 minutes (average, 60 minutes). After the drainage, T1-weighted spin-echo images were obtained to determine the presence of hemorrhage, the alteration in the size of the lesion, or other changes. All cases were in-patients, and they were followed up with CT studies because abscesses can be detected easily and follow-up is available immediately.
The needle was identified clearly as a linear signal void with its actual diameter (4 mm). It was safely navigated intracranially to the target lesion. All abscesses were reached on the first attempt, except one, which was reached on the second attempt because the bore hole could not be placed at a suitable place. The needle was guided to reach the center of the ring-enhanced lesion, and the abscesses were slowly aspirated under continuous imaging monitoring to observe the progressive collapse of the abscess walls. The presence or absence of hemorrhage, the accuracy of aspiration site, and changes associated with decompression of brain parenchyma and ventricular system were clearly seen.
Altogether, 16 drainages were performed in 12 abscesses in 11 patients. Single aspiration was carried out in seven patients, and re-aspiration was performed in four patients because of recurrence or insufficient aspiration. Eight patients (73%) were treated using an MR guidance procedure. One patient died of meningoencephalitis after total drainage. One patient, with an 8 × 5 cm abscess, was referred for surgery after the second drainage. In another case, because the abscess material was too viscous even for an 18-gauge needle, the patient (a baby with meningitis) was also referred to the surgery department (Table).
Eleven patients who underwent MR-guided drainage
From 2 to 150 mL of pus material were drained from abscesses. Pus culture was sterile in eight patients and grew Staphylococcus aureus in two patients. The pathologist thought amibiasis in one case. Minimal hemorrhage (1), minimal subdural effusion (2), air in the cavity (3), and minimal leakage of CSF in the access hole (1) were shown in this study.
Discussion
Bacterial brain abscesses can be diagnosed and treated with percutaneous aspiration under imaging modalities. Drainage of brain abscesses are carried out in most centers with contrast-enhanced CT. When the lesion cannot be demonstrated well with CT, MR imaging is used. They have provided promising results in the management of this disease. One major advantage of modern imaging techniques is the use of stereotaxy. Sharp fixation of a frame to the skull, however, is quite uncomfortable for the patient, and any dislocation of the frame disrupts the relationship of the reference system to the chosen target (4). In addition, MR-compatible tools of stereotaxy are expensive. Stereotactic drainage of abscesses can be carried out for the lesions located in cerebral hemisphere, cerebellum, pons, or brain stem (1, 2). These procedures are planned on the basis of preoperative images and therefore do not provide formation on the pathologic changes occurring during the procedure. These changes include brain shift and shifting of target structures and are seen usually in brain abscesses. Most abscess walls are soft and easily punctured, but a subpopulation of abscesses appears to have a solid wall, a characteristic that could lead to mistargeting when conventional stereotaxy is used (5). Because a thin needle (18 gauge) was used in this study, we did not encounter such a problem in any patient.
The needle artifact was 4 mm wide for an 18-gauge needle in our study. There are several key imaging factors that alter the appearance of needle artifact during biopsy, including the dependence of this artifact on the direction of frequency encoding in the image and the bandwidth of the imaging sequence. The carbon fiber-based biopsy needle is more promising material than titanium for the design and construction of MR-compatible instruments (8). The size of susceptibility artifact in spin-echo is less than gradient-echo sequence, and low field strength is superior for visualization of the needle (9). Titanium instruments, gradient-echo sequences, and a low-field-strength (0.3T) magnet were used in this study, and the needle artifact was not difficult to visualize in the abscess cavity when the needle was approximately perpendicular to the main magnetic field.
Ultrasonography and CT are alternative image-guidance systems (1–3). Because of the poor image quality and inability to penetrate the skull bone, use of ultrasonography alone is limited. Radiation, beam-hardening artifacts related to metallic devices and lack of 3D data are disadvantages of CT. In addition, multiplanar capabilities, high spatial resolution and excellent soft tissue contrast, and the absence of ionizing radiation makes MR guidance for brain interventions an attractive alternative. The ability to monitor the drainage by using near-real-time imaging information is exceptional with MR imaging (6). In this study, a freehand technique was used. During evacuation of pus material, the freehand technique with MR fluoroscopy provided information about the amount of abscess drainage, making it easier to evacuate an abscess completely with no risk. Repositioning of the needle tip could be possible, and monitoring prevented overevacuation of the abscesses.
MR-guided drainage was performed without special requirements such as an in-room monitor or special biopsy coil in this study. A flexible transmit-receive coil is usually used in an interventional MR imaging department (6). We used only an MR-compatible needle as an extra instrument for MR-guided intervention. The surface ring coil for cervical examination that was used is 6 cm wide and is not flexible. Sometimes we encountered sterilization problems due to the fact that the sterile cloth was not able to cover the whole skin area of the head. The targeting, however, was not seen in any patients. If there is an MR-compatible needle, drainage of brain abscess under MR-guidance can be managed even if an MR-compatible in-room LED screen monitor and specific biopsy coil were absent.
Kollias and Bernays (6) drained eight brain abscesses in seven patients by using MR-guidance frameless stereotaxy in an open-configuration 0.5T superconducting system. Tronnier et al (4) drained six abscesses by using a 0.3T open system.
In management of brain abscesses, more than one aspiration may be needed, and repeat aspiration are often necessary for cure (10). A second aspiration was needed in four (36%) patients. Recurrence was reported 21% in Kondziolka et al’s study (11), 14% in Kollias et al’s study (7), and 8% in Boviatsis et al’s study (12). Surgical excision was performed in one patient because the abscess was very large and could not be entirely aspirated after the second attempt. Large and multiloculated abscesses may need excision if simple aspiration proves inadequate (10, 11), as in the second patient (Table). The procedure was not successful in the case of one patient (9%), a child, because of the viscosity of the abscess material. Strowitzki et al (3) also reported insufficient aspiration in 8% of patients. Needles as large as 16 gauge were needed for the drainage. We determined that a variety of needles, especially 16–18 gauge, must be present in the interventional neuroradiology suite. Moreover, the viscosity of subdural empyema was less than that of the parenchymal abscesses; the former were evacuated easily. We conclude that use of a 16-gauge needle for a viscous abscess and closed external drainage for a large lesion can increase the success of this method.
The uniform, ringlike enhancement of abscess capsule may provide definition of the lesion. Although a double dose of contrast agent can be used to optimize visualization of the target lesion (6), we used a standard dose of contrast agent and capsules of the lesions were visualized clearly in all cases.
On average, the intervention took 60 minutes, plus 15 minutes for targeting, in our study. With experience, the procedure time was reduced. According to Kollias and Bernays (6), procedure time was 1.7 hours.
Conclusion
Drainage of cerebral abscesses by use of MR fluoroscopic drainage is a safe and reliable procedure, but it usually requires expensive instruments such as an MR-compatible monitor, needle, respirator, stereotactic device, biopsy coil, neurobiopsy needle probe, and sterile procedure room. This study shows that if an MR-compatible fine needle is available, drainage of brain abscess can be accomplished in a standard open MR configuration system.
Acknowledgments
We sincerely thank Dr. Emin Oguz for his extensive help in the writing of this article.
References
- Received May 21, 2004.
- Accepted after revision November 4, 2004.
- American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.