
Abstract
Summary: An 11-year-old girl presenting with neck pain was diagnosed as having an aneurysmal bone cyst involving the posterior arch of C1. Minimally invasive treatment was performed with percutaneous injections of calcitonin and methylprednisolone. Two injections separated in time by 2 months were performed with complete sclerosis and ossification of the cyst over a period of 6 months. Such percutaneous sclerosis offers an important primary therapeutic option or an adjunct to surgery of these otherwise vascular cystic masses and should be contemplated as the initial step in the treatment of these benign tumors, especially those in the spine where surgical treatment can involve complex resection and fixation procedures.
Aneurysmal bone cysts are expansile lytic bone lesions. The radiographic appearance of these lesions has been well documented on conventional radiographs, CT scans, and MR images. Numerous cases of pediatric aneurysm bone cysts affecting the spine have been reported (1–3). Treatment of these lesions typically involves resection and curettage (4–6). Other strategies have included radiation therapy (7) and sclerotherapy (8). Angiographic findings of these lesions and preoperative embolization have been reported (9, 10).
The following is a case report discussing the presentation, imaging, and treatment of an 11-year-old girl with an aneurysmal bone cyst at the posterior arch of C1.
Case History
An 11-year-old girl presented with a 4-year history of increasing neck pain and headaches. Her neurologic examination in the clinic was normal. MR imaging showed an expansile lytic mass in the posterior arch of C1 with a predominantly fluid signal intensity and one or two small fluid-fluid levels. A thin-section CT revealed an expanded C1 lamina with thin eggshell cortical margin and small internal septation (Fig 1). The thin bony margin was causing some narrowing of the spinal canal. Radiographic diagnosis of aneurysmal bone cyst was entertained, with other possibilities such as osteoblastoma considered less likely.

Thin-section axial images show the expansile lytic lesion at the posterior arch of C1
Because there was no neurologic compromise and no cervical spine instability, surgical excision and associated spine fixation was deemed unnecessary. The more traditional interventional radiology procedure of particle embolization was also excluded because of the additional risks in the upper cervical region of vertebrobasilar and spinal arterial embolization. An initial attempt at percutaneous ablation of the cyst was considered a reasonable minimally invasive alternative.
The percutaneous procedure was performed under general endotracheal anesthesia. Under CT guidance, a coaxial biopsy needle was passed through the expanded outer cortex into the cystic mass (Fig 2). Four milliliters of blood were easily aspirated. A core specimen of the deeper wall of the cyst was obtained without discernable osseous tissue. The easy return of blood reinforced the diagnosis of an aneurysmal bone cyst. A mixture of 200 IU of calcitonin and 125 mg of methylpredisone was gently injected into the aneurysmal bone cyst. Finally, DBX bone putty (Dentsply Friadent Ceramed, Lakewood, CO) was injected on the outer aspect of the puncture site in the cortex.

Axial CT images document the coaxial needle placement within the aneurysmal bone cyst.
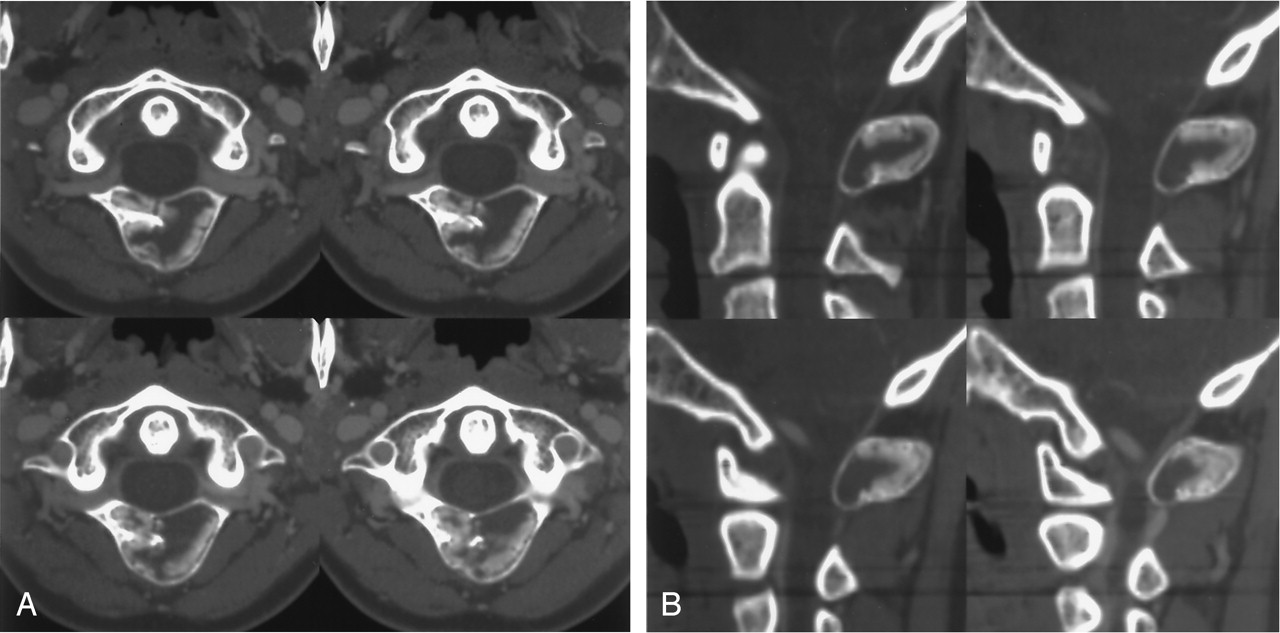
The patient had significant symptomatic relief after the injection, lasting for about 2 months with some return in pain after that. A second similar intralesional injection was performed. A CT scan at that time showed increased sclerosis within the cyst, which indicated response to treatment (Fig 3). The patient had continued improvement of her neck pain with a 6-month follow-up CT scan showing complete ossification of the aneurysmal bone cyst (Fig 4). She did have recurrence of some of her pain, especially in the occipital region, and her occipital neuralgia was presumed to be secondary to mass effect and compression against upper cervical nerve roots by the now ossified cyst. Laminectomy and excision of the aneurysmal bone cyst was performed. Final pathologic diagnosis was consistent with aneurysmal bone cyst wall. Over the next month or so, her neck pain and upper cervical radiculopathy resolved.

Axial (A) and sagittal (B) reformatted images 2 months after the first intralesional injection show sclerosis developing along the margins of the aneurysmal bone cyst.

Thin-section axial images about 6 months after the first injection show near-complete sclerosis.
Discussion
Surgical treatment of spinal aneurysmal bone cysts, which can be very vascular, is technically challenging involving resection and curettage and spine fixation. These procedures carry the risk of significant blood loss, postoperative spinal deformity and the possibility of recurrence (1). Percutaneous intralesional injections offer the least invasive initial therapeutic option with more invasive surgical or endovascular strategies (3, 10, 11) reserved for resistant lesions. In this case, since the aneurysmal bone cyst involved the posterior arch of C1, the vascular supply would have likely been from either or both of the verterbral arteries with possibly some feeders from the external carotid system. Embolization of any feeders arising from the vertebral arteries carry the risk of inadvertent intracranial and spinal artery embolization with potentially devastating complications. In this case, because of the patient’s young age, the location of the lesion, the complex spine surgery involved and the risks of preoperative embolization, it was decided to start with the least invasive and complex procedure (percuatneous ablation) with embolization and surgery as an alternative if the initial treatment failed. Placement of a biopsy needle under CT guidance is relatively safe as long as the cortical margin toward the spinal canal is not breached. Needle insertion should be planned in such a way that any potential bleeding should not compromise the spinal canal. Calcitonin inhibitis osteoclastic activity and promotes trabecular bone formation. Methylprednisolone has an antiangiogenesis effect. The procedure we chose has been previously described (12, 13). In our case there was fairly rapid sclerosis and stabilization of the lesion. Surgery performed for persistence radicular symptoms was relatively straight forward with partial laminectomy without the need for occipitocervical fixation and with minimal blood loss.
Conclusion
Image guided percutaneous sclerosis of spinal aneurysmal bone cysts offers a relatively safe, simple and minimally invasive option either as primary treatment or as an adjunct to surgery.
References
- Received April 27, 2004.
- Accepted after revision May 6, 2004.
- Copyright © American Society of Neuroradiology
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.