
Abstract
Summary: CT findings of the base of the neck are often degraded by beam-hardening artifact from the shoulder girdle. This artifact can be reduced by placing the patient in a “swimmer’s” position, a supine position in which the patient has one arm fully abducted and the other arm lowered. We selectively employed swimmer’s CT in patients between January 1999 and December 2002 when standard (arms-down) CT failed to depict suspected disease. In nine of 10 patients, swimmer’s CT improved CT quality or accuracy or both over that obtained when the standard CT position was used.
The difficulties in radiography of the cervico-thoracic junction are well known, because of the frequency of trauma and the importance of excluding injury to the cervical spine. The swimmer’s technique was first described in the 1980s as a means to depict this area (1, 2). CT scanning has also long been employed to clarify lingering questions in this area (3). CT has been successful in imaging the complex vascular syndromes that can occur from compression of the subclavian artery and vein in the thoracic outlet syndrome (4). Nonetheless, CT artifacts (eg, beam hardening) also occur in this area because of high soft tissue and bone attenuation.
Technique and Results
Ten patients with suspected disease at the base of the neck who underwent routine neck and cervical spine CT and were imaged in the conventional, arms-down position were found to have nondiagnostic scans. Repeat CT was performed in the swimmer’s position (Fig 1). All patients were imaged supine, with one imaged prone because of discomfort while supine. All other parameters were kept constant in each standard and swimmer’s CT scan. In three patients, scanner auto select of mAs produced less than 10% variation in this parameter. Scan parameters included a 15–25-cm field of view, 120 KvP, 170–300 mAs, 1.5- or 3-mm scan thickness, pitch of 1 to 1.6, and 0.8-second gantry rotation. The indications for examinations included suspected soft-tissue mass or vascular malformation in three (thyroid enlargement, level V lymph node, vascular malformation), postmyelography in three, radiculopathy in two, suspected abscess, and suspected C7–T1 traumatic instability. The two image sets were compared for lesion conspicuity and presence of beam-hardening artifact. The Human Use Committee at Tripler Army Medical Center approved the study protocol. Investigators adhered to the policies for protection of human subjects as prescribed in 45 CFR 46.

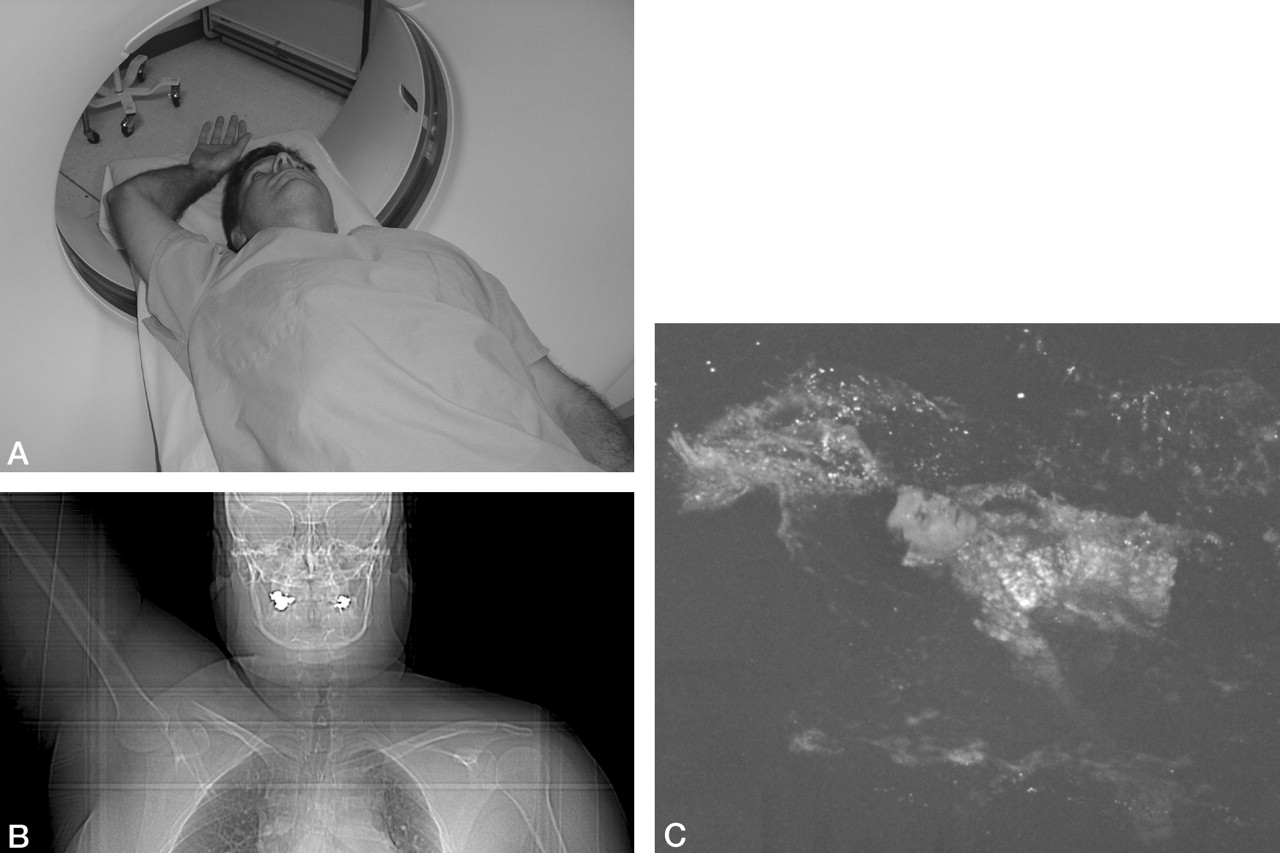
A, Volunteer in swimmer’s position, with one arm raised above head, the other with shoulder depressed, while supine within CT scanner. B, CT scout in swimmer’s position. Note the right humoral head and clavicle are no longer in the same axial plane as the left. C, Backstroke while swimming, from which the swimmer’s position is named.
In nine of 10 patients, beam hardening present on the initial scan was eliminated on the swimmer’s CT scan. In two patients, lesions not visible on the initial scan were made apparent on the swimmer’s CT scan (Fig 2). These included a Delphian node and a symptomatic cervical lateral foraminal C6–C7 disk on CT myelography. The foraminal disk was proved surgically and removed with relief of symptoms. The depiction of anatomy and soft-tissue contrast was judged to be better in eight of 10 scans (Figs 3–5).

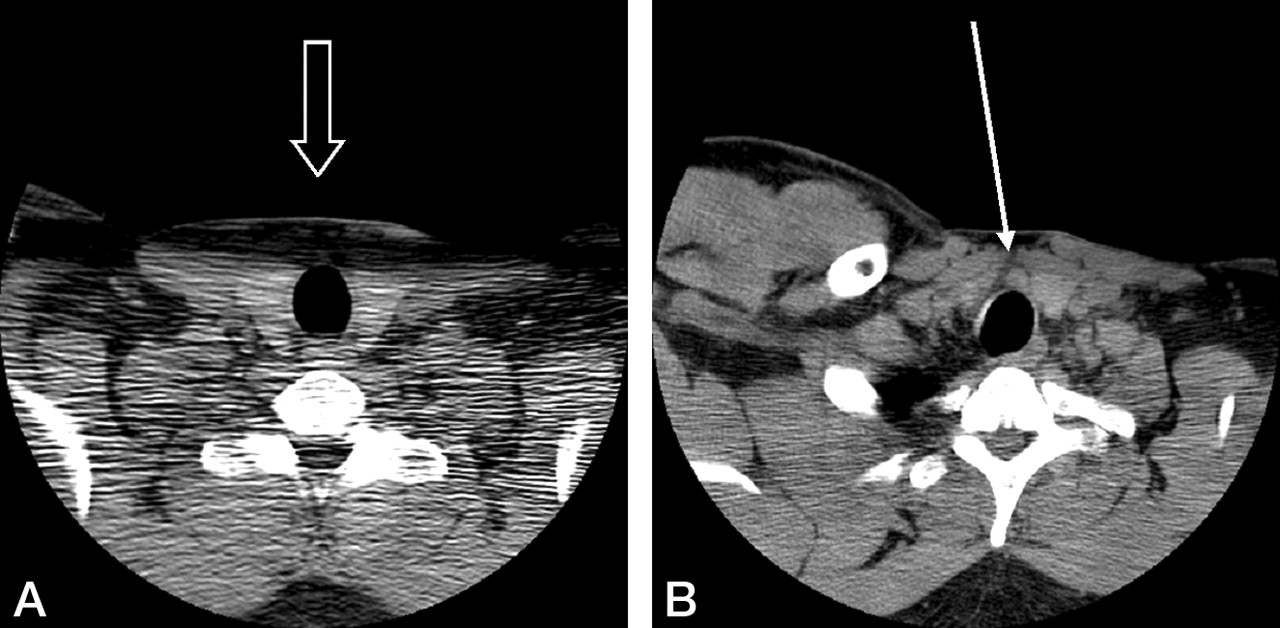
A, In normal position, beam hardening completely obscures pretracheal soft tissues (open arrow). B, With swimmer’s positioning, the arrow depicts a pretracheal lymph node just above the thyroid isthmus, and just beneath the larynx. This node has been referred to as the Delphian node and is not visible in the left image because of artifact. Notice the asymmetry of the clavicle and scapular position and musculature in the swimmer’s position (B), making normal anatomy more difficult to assess. This later point constitutes cause for reservation of the swimmer’s position until after normal anatomy has been initially assessed with conventional (symmetric) positioning.

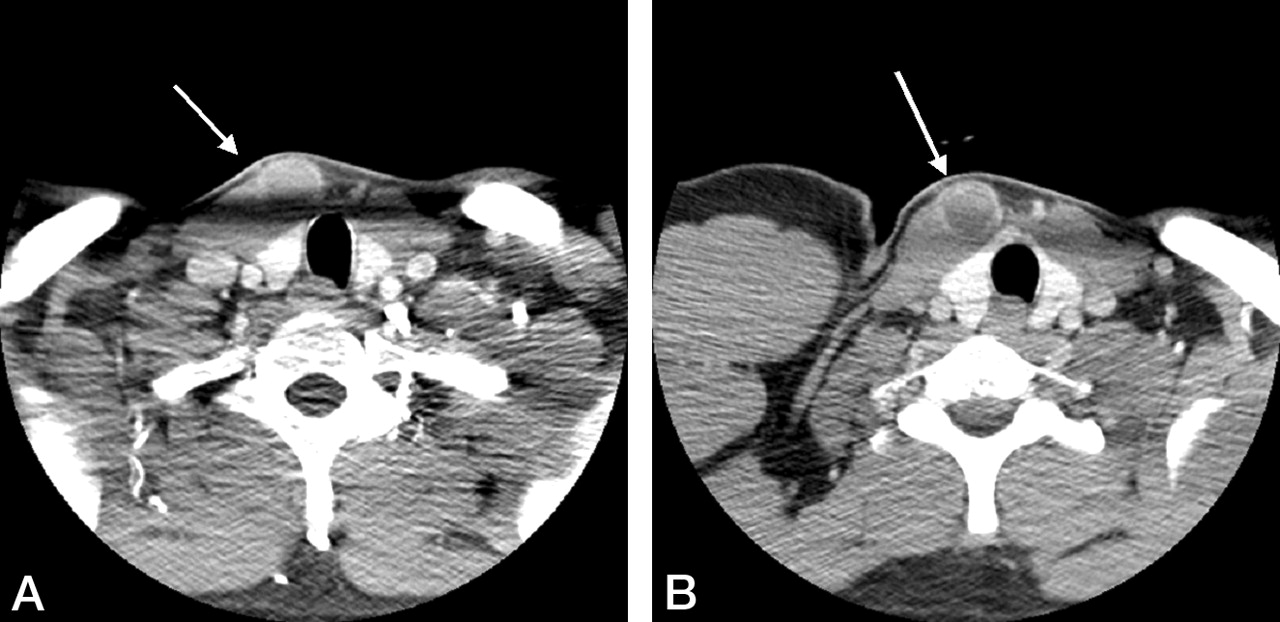
A, Beam hardening at the level of the thyroid isthmus results in decreased soft-tissue contrast and obscures the vascular malformation (arrow) anterior to the right sternocledomastoid muscle, which is better seen in panel B, with the swimmer’s position (open arrow). This lesion had been present and stable for many years and may actually represent a type II or III branchial cleft cyst, as it lies anterior to the lowermost aspect of the sternocleidomastoid muscle. No tract was visible; thus, venous or lymphatic malformation was the favored diagnosis.
Discussion
This retrospective series indicates the swimmer’s position can be useful when attempting to depict or detect abnormalities on CT. The swimmer’s CT position has some limitations, such as the loss of symmetry of scapular and chest wall musculature (Fig 2).
Although for 20 years the utility of the swimmer’s maneuver has been well established in conventional radiology, it is not without its limitations and alternatives as well (5, 6). It is unclear exactly when the swimmer’s view was first employed in the evaluation of lower cervical trauma, but it is clear that it was not conceived of or at least was certainly not widely known because of the lack of reference to it in articles on the subject published in the 1970s (7). Now, however, it is perhaps the most common adjunctive maneuver done on a daily basis in most radiology departments because of the frequency of conventional radiographic evaluation of cervical spine trauma and deceleration injury from motor vehicle accidents (8). With regard to its use in CT, the desire to identify a lesion must be weighed against the need to maintain symmetry of chest wall structures such as the subscapularis and rhomboid musculature, as well as the shoulder girdle itself (Fig 2).
Thus, to minimize radiation, patients should typically be imaged by the standard CT scan position first to benefit from symmetry in attempting diagnosis in this complex anatomic region. In some cases, MR imaging may be the study of choice rather than a repeated attempt with swimmer’s CT position. This is true in patients with large body habitus, in whom CT of the thoracic inlet and base of neck is deemed inadequate because of artifact or because of the need for superior soft-tissue contrast achievable with MR imaging. Nonetheless, clinically relevant disease that affects patient care and outcome can be demonstrated by the swimmer’s CT position. For instance, the Delphian lymph node, a pretracheal node seen in Figure 2, is significant in that, when present on imaging, it often harbors metastasis in patients with cancer of the larynx. The Delphian node, which harbors malignant cells in the setting of laryngeal cancer, has been shown to indicate a 64% chance of 5-year recurrence, whereas those patients without malignant pretracheal lymph nodes only have a 12% recurrence rate (9). Similarly, the features of lesions are better depicted, allowing a more specific lesion characterization (Fig 3), more precise lesion depiction (Fig 4), or more confident confirmation of the presence of disease (Fig 5).

Seat-belt deceleration vertical fracture of anterior aspect of second thoracic (T2) vertebral body. Multidetector CT in standard (A and C) and swimmer’s (B and D) position obtained by reformatted 0.6-mm-thick axial images then sagittally reconstructed. The superior mediastinum and soft tissues are more distinct in panel B than in panel A, whereas swimmer’s sagittal reconstruction (D) more sharply demarcates the fracture boundary and endplate defects (arrow). E, Proton density-weighted sagittal MR confirms the lower T2 endplate defect (arrow). F, Fat-suppressed T2-weighted sagittal MR confirms acuity of fracture on the basis of marrow edema (arrow).

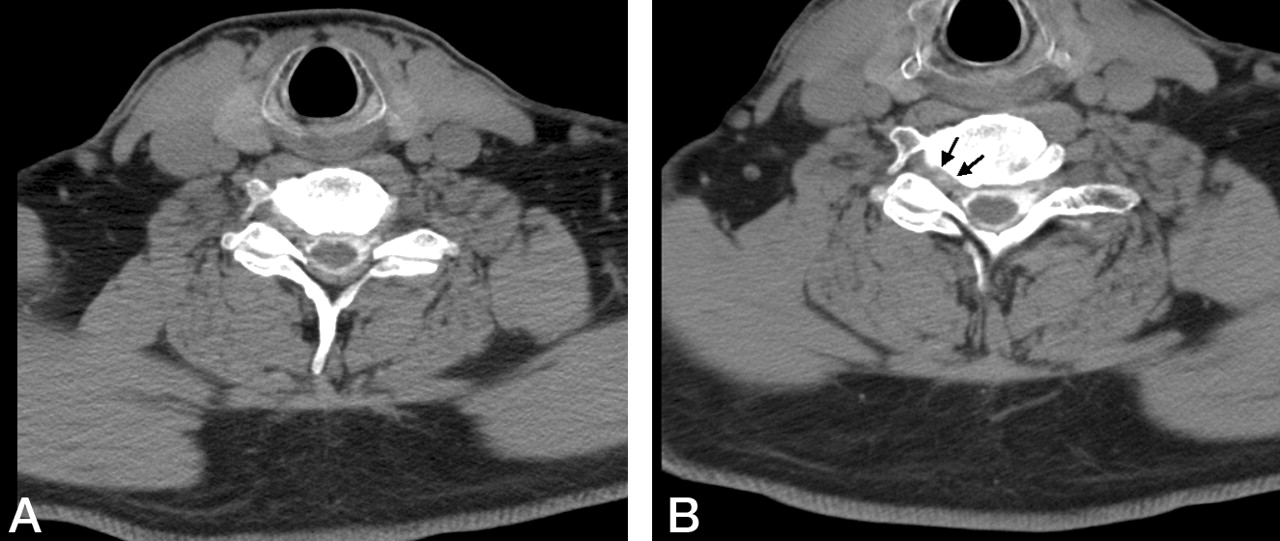
Right C7 radiculopathy evaluated with cervical postmyelography CT axial images at 1.5-mm thickness at same level in standard (A) and swimmer’s (B) position. A, Beam hardening produces linear areas of decreased attenuation in the right foramen, contrast-opacified CSF and spinal cord, and linear variable attenuation in the left foramen and soft tissues compared with swimmer’s CT (B) B, Swimmer’s CT demonstrates distinct uniform soft-tissue attenuation representing formamenal disk herniation (surgically confirmed) in the right foramen (arrows) while also better demonstrating normal uniform fat attenuation surrounding the nerve root sleeve in the normal left foramen.
The issues of beam-hardening at the base of neck remains an issue with multidetector CT, though less so. Despite rapid sub-millimeter imaging, Figure 4 demonstrates improvements obtainable when imaging with an 8-channel multidetector CT scanner.
Beam-hardening artifact and excess attenuation sometimes can obscure significant disease at the base of the neck. The swimmer’s CT position is a useful maneuver to be considered on an as-needed basis during CT for suspected disease at the base of neck and thoracic inlet.
Footnotes
Presented at the 41st annual meeting of the American Society of Neuroradiology, Washington, D.C., April 16–May 2, 2003.
The views expressed herein are those of the authors and do not reflect the official policy or position of the Department of the Army, Department of Defense, or the U.S. government.
References
- Received August 20, 2003.
- Accepted after revision January 5, 2003.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}