
Abstract
Summary: A 70-year old man with a 15-year-history of chronic daily Valsalva maneuvers for left ear congestion presented with worsening vertigo and calvarial (occipitoparietal) and upper cervical hyperpneumatization. With continued frequent Valsalva maneuvers, subsequent studies demonstrated increased pneumatization with extension of air into the epidural space, causing mass effect on the left parietal lobe. Four months after discontinuing the habitual Valsalva maneuvers, CT demonstrated resorption of the epidural air and partial regression of the calvarial pneumatization.
Calvarial hyperpneumatization is a rare disorder. To the best of our knowledge, only six other cases have been reported in the literature (1–6). Acquired hyperpneumatization associated with a long history of habitual Valsalva maneuver, the striking progression over a relatively short period of time, the development of epidural air, and the response to conservative treatment are reported.
Case Report
A 70-year old man with a 15-year history of habitual Valsalva maneuver for left ear congestion presented with worsening vertigo and a “gurgling sensation” in his left ear and skull. Ten years before presentation at this institution, he perforated his left tympanic membrane after minor trauma. Head CT at that time revealed some pneumatization of his occiput, but there were no fractures. Because of worsening symptoms, CT was performed elsewhere 3 years before presentation and revealed extensive pneumatization of the left occipital and parietal calvaria (Fig 1A). The patient continued to perform Valsalva maneuvers multiple times every day. Subsequent CT performed elsewhere 8 months before presentation revealed an increase in pneumatization, which extended into the epidural space, causing mass effect on the left parietal lobe (Fig 1B and C). Pneumatization at that time had also progressed to involve the right skull base, right lateral mass of C1, and the left petrous apex (Fig 2). The patient was instructed to and stopped habitual Valsalva maneuver 4 months before presentation. CT at presentation demonstrated resorption of the epidural air with resolution of mass effect. The pneumatization was less prominent, and the air was mostly replaced by fluid (Fig 1D). CT cisternography was performed and excluded CSF leak before consideration of pressure equalization tube placement. Conservative therapy with a nasal steroid inhaler to improve eustachian tube function and instructions to stop Valsalva maneuvers alleviated his symptoms altogether, precluding the need for surgical intervention.

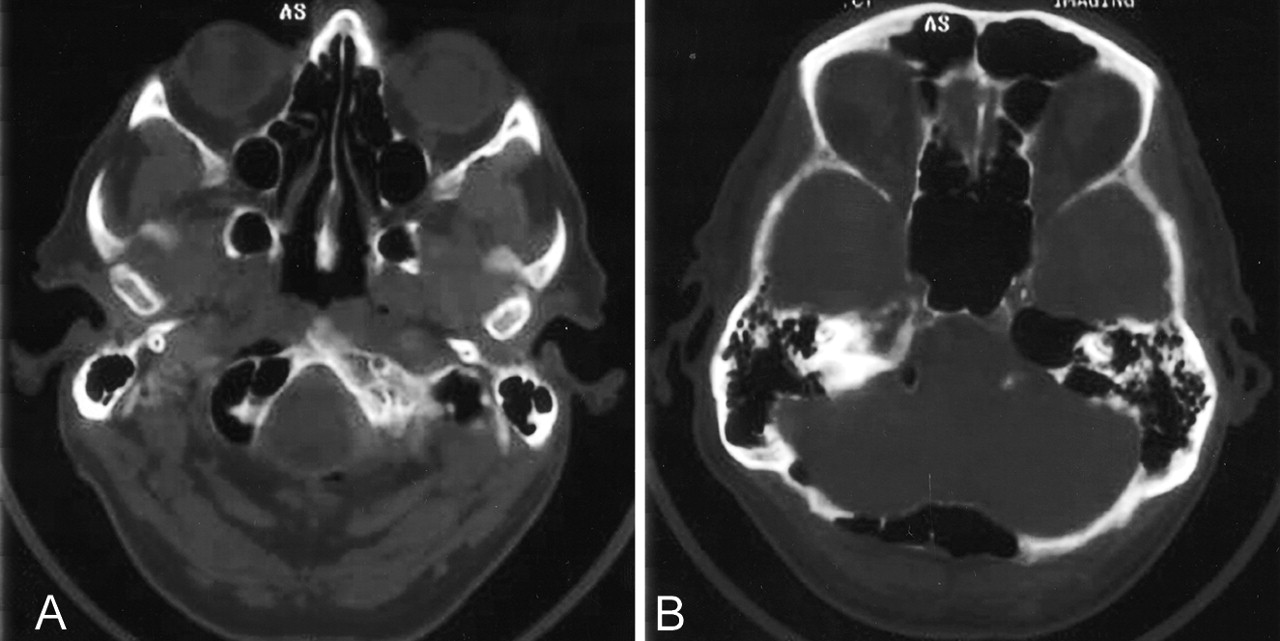
Sequential axial CT head images. Selected images (A) from CT head performed 3 years before presentation demonstrate pneumatization of the diploic space of the occipital and posterior parietal bones extending to the level of the vertex with marked thinning of the inner table. After this patient continued to perform daily Valsalva maneuvers, subsequent CT examination performed elsewhere 8 months before presentation with soft tissue windows (B) revealed an increase in pneumatization, which extended into the epidural space causing mass effect on the left parietal lobe. Bone windows (C) from this examination demonstrate complete dehiscence of the inner table. The patient discontinued habitual Valsalva maneuvers and CT scan performed at presentation (D) demonstrated resorption of the epidural air with resolution of mass effect. The pneumatization was less prominent and the air was mostly replaced by fluid.

Additional axial CT head images (A and B) performed 8 months before presentation. CT images demonstrate extension of air into the left petrous apex as well as involvement of the skull base with pneumatization of the right occipital condyle and extension into the anterior soft tissues.
Discussion
Embryologically, temporal bone air cells originate from an out-pouching from the lateral nasopharynx that courses up the eustachian tube, through the middle ear and aditus ad antrum, into the mastoid antrum. Middle ear and perilabyrinthine air cell development is fairly consistent. Pneumatization of the mastoid and petrous bones can vary greatly, and in cases of well-pneumatized temporal bones, accessory occipital air cells may occur that communicate with the mastoid air cells and middle ear. Other accessory sites of air cell pneumatization include zygomatic, squamous, and styloid (7). The mastoid antrum may be visible in the neonate and is usually visible by 2 or 3 months of age. Mastoid pneumatization occurs throughout childhood with air cells becoming visible by about 6 months of age and increase in size and number throughout childhood until maturity, when air cell development ceases (8, 9).
To the best of our knowledge, only six other cases of calvarial hyperpneumatization have been reported in the literature (1–6). In two of these cases, the condition was associated with frequent Valsalva maneuver and, like this case, regressed or resolved after the habit was stopped (1, 2). This case reinforces the concept that hyperpneumatization is associated with habitual Valsalva maneuver. Barometric pressure within the temporal bone should approximate ambient barometric pressure. Normally, the eustachian tube temporarily opens with each swallow to permit pressure equalization (7). Calvarial hyperpneumatization is thought to result from a dysfunctional eustachian tube acting as a ball valve, causing increased middle ear pressure and air entering the calvaria through the mastoid sinus (Fig 3) (1, 3). Because pneumatization normally ceases at maturity, it is interesting to note the pronounced progression of pneumatization that occurred over a 28-month period despite the advanced age of this patient and the chronicity of his symptoms, which had persisted for more than 10 years. Although the exact etiology of this patient’s vertigo is unclear, there was a direct relationship between increasing calvarial pneumatization and intracranial air and worsening vertigo. This patient also experienced improvement in his symptomatology with resolution of the epidural air, suggesting a possible causative effect.

Illustration demonstrating the relationship between eustachian tube, middle ear, and mastoid air cells. Normally, the eustachian tube temporarily opens with each swallow to permit pressure equalization (7). A dysfunctional eustachian tube, acting as a ball valve, could lead to increased middle ear pressures and air entering the calvaria through the mastoid antrum (1, 3) (arrow).
This case also demonstrates that extensive pneumatization can lead to epidural air with resulting mass effect. This phenomenon has previously been reported in a single case in which surgery was performed to obliterate the calvarial air cells and relieve mass effect (3). This is the only case demonstrating that both the calvarial pneumatization as well as the epidural air can be reversed rather quickly with elimination of chronic Valsalva maneuver.
- Received April 24, 2003.
- Accepted after revision June 4, 2003.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}