
Abstract
Summary: Infarction of the choroid plexus may result from ischemia in the distribution of the medial posterior choroidal artery. Diffusion-weighted imaging may depict this unusual stroke syndrome. The clinical and radiologic aspects of this rare condition are discussed taking into consideration the anatomy and pathophysiology of the choroid plexus.
The choroid plexus plays a pivotal role in the regulation of CSF, determining permeability of the blood-CSF barrier, containing various types of receptors, and secreting numerous growth and trophic factors (1). Despite the elaborate function of the choroid plexus, pathologic derangements of this structure are of rare clinical significance. Diffusion-weighted (DW) imaging may reveal clinically silent lesions of the choroid plexus. We describe an unusual case of infarction of the choroid plexus due to medial posterior choroidal artery stroke.
Case Report
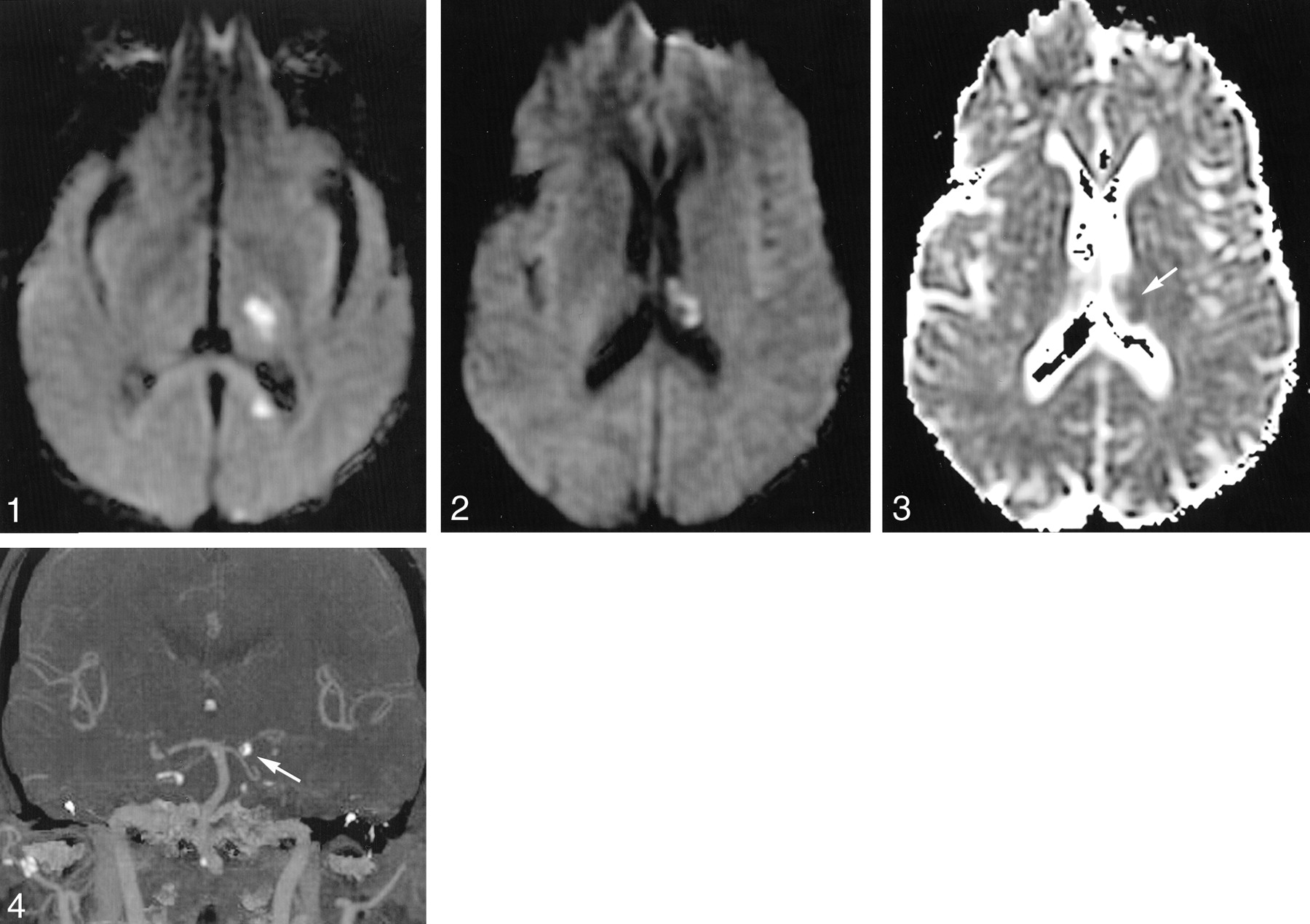
A 54-year-old man with hyperparathyroidism presented with acute-onset right hemisensory loss and hemiparesis without visual impairment. After 30 minutes, these symptoms resolved with the exception of minimal right face and hand numbness. Two days later, he had abrupt-onset, complete right hemisensory loss. On hospital admission, noncontrast CT revealed a hypoattenuated lesion consistent with a subacute left thalamocapsular lacunar stroke. Fluctuations in the severity of his hemisensory deficits correlated with blood pressure readings over a period of several days, without associated neurologic deficits. DW imaging performed 5 days after the initial onset of symptoms illustrated thalamocapsular lacunar infarction due to thalamogeniculate ischemia, a splenial lesion due to pericallosal involvement, and limited infarction of the occipital cortex due to distal posterior cerebral artery involvement (Fig 1). Infarction of the choroid plexus in the left lateral ventricle was also demonstrated on DW images (Fig 2). Apparent diffusion coefficient (ADC) maps confirmed restricted diffusion in all involved regions, with only minimal reduction of ADC values in the choroid plexus lesion (Fig 3). MR angiography demonstrated a segmental occlusion of the left posterior cerebral artery that was corroborated with conventional angiography. The presence of prominent vascular calcifications and mobile aortic arch atheromata prompted further investigation with CT angiography (CTA). CTA demonstrated in situ calcification of the posterior cerebral artery (Fig 4). After several days of antiplatelet therapy and vigorous hydration, his clinical symptoms subsided with only mild right hemisensory loss.

DW image reveals scattered hyperintensities in the vascular distribution of distal branches of the left posterior cerebral artery, including the superficial cortical branches, thalamogeniculate, and pericallosal arteries.

DW image reveals infarction of the choroid plexus in the left lateral ventricle.

ADC map shows only minimal reduction in coefficient values within the choroid plexus lesion (arrow).

CT angiogram reveals in situ calcification of the left posterior cerebral artery (arrow).
Discussion
To the best of our knowledge, infarction of the choroid plexus has not been described previously. This unusual pattern of ischemia likely resulted from involvement of a medial posterior choroidal artery, emanating from the posterior cerebral artery in close proximity to the thalamogeniculate perforators that caused the thalamocapsular lacune (2, 3). The scattered infarcts in the distribution of various distal branches of the posterior cerebral artery, including the medial posterior choroidal, may have developed insidiously in association with progressive stenosis of the parent vessel. Variability in the degree of the ADC decrements may be due to differing ages of the ischemic lesions, although interpretation of DW abnormalities of the choroid plexus may be limited by inherent differences with respect to brain parenchyma. The differential diagnosis of DW abnormalities in the intraventricular space includes lesions of the choroid plexus, such as cysts and xanthogranulomata, intraventicular hemorrhage, and pyogenic ventriculitis. DW abnormalities of the choroid plexus may be caused by a variety of choroid plexus cysts and xanthogranulomata, although conventional MR imaging may help differentiate these lesions on the basis of appearance and location. The DW abnormality visualized in this case is located in an unusual location for a cystic lesion, and xanthogranuloma typically has bilateral involvement. Intraventricular hemorrhage and pyogenic ventriculitis may produce DW abnormalities, although extension into adjacent ventricular structures in dependent fashion and corresponding signal intensity abnormalities at conventional MR imaging may be expected. Such neuroimaging features were not observed in this case, because the DW abnormality was restricted to a focal region of the choroid plexus. The simultaneous depiction of multifocal DW abnormalities in the distribution of sibling tributaries of the posterior cerebral artery supports the diagnosis of choroidal infarction.
Medial posterior choroidal infarcts are rare, with neurologic findings that may be difficult to discern from adjacent lesions (4). Because most posterior cerebral artery infarcts are embolic and associated with more proximal ischemia, involvement of the medial posterior choroidal artery may go unrecognized.
Anastomoses of the anterior and posterior choroidal arteries are believed to protect the highly vascular choroid plexus from ischemia. Despite the presumed luxuriant collateral circulation of the choroid plexus, recent investigations of focal cerebral ischemia and hypoxic-ischemic injury have demonstrated the relative vulnerability of this structure (5, 6). Apoptotic and necrotic cell loss in the choroid plexus may result from either hypoxic-ischemic injury or secondary involvement due to parenchymal ischemia (7). The choroid plexus of the lateral ventricle appears to be more vulnerable to ischemia compared with the portion of this structure residing in the fourth ventricle (8). Collateral blood flow to the choroid plexus likely also varies by the specific anatomic segment of this structure.
Localized infarction of the choroid plexus probably has a negligible effect on CSF regulation without any clinical manifestations. Alteration of the permeability of the blood-CSF barrier may theoretically exacerbate cerebral edema following stroke; however, stabilization of brain fluid balance may be rapidly restored by the choroid plexus (9). Although infarction of the choroid plexus may be clinically silent, recognition of this entity may expand the differential diagnosis of intraventricular lesions with characteristic features that may exclude clinically portentous diagnoses.
Conclusion
Increasingly routine use of DW image for stroke will likely reveal various clinically silent infarct patterns that may invoke an underlying stroke or vascular mechanism. Unusual stroke syndromes such as medial posterior choroidal artery infarction may be readily apparent on DW images, leading the clinician to search for relatively subtle aspects of stroke origin. Choroidal infarction as demonstrated by DW imaging may have limited clinical significance yet may provide further insight into the pathophysiology of this complex structure.
References
- Received April 16, 2003.
- Accepted after revision May 20, 2003.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.