
Abstract
BACKGROUND AND PURPOSE: Three-dimensional time-of-flight (TOF) MR angiography has been evaluated in the follow-up of intracranial aneurysms treated with Guglielmi detachable coils (GDCs) with good results. Some of the studies used contrast material in addition to the 3D TOF MR technique and others did not. We assessed the usefulness of contrast material with 3D TOF MR angiography by comparing this sequence before and after contrast material injection.
METHODS: Fifty-eight patients harboring a total of 71 cerebral aneurysms previously treated with GDCs were included in the prospective study. MR angiography (at 1.5 T) was performed with a 3D TOF sequence before and after injection of gadolinium-based contrast material. Features evaluated were presence and size of a neck remnant, parent and adjacent vessel patency, and venous overlap. Digital subtraction angiography was the standard of reference.
RESULTS: Comparison of the techniques showed a good agreement in the detection of residual flow. Six cases of small residual neck were not detected with either the 3D TOF or the contrast-enhanced 3D TOF sequence. In one case of giant aneurysm, the extent of recanalization was more evident after contrast material administration. The use of contrast material did not help to show the parent and adjacent arteries. Venous overlap on contrast-enhanced 3D TOF angiograms did not affect image interpretation.
CONCLUSION: In this series, the use of intravenous contrast material did not improve the ability of 3D TOF MR angiography to depict the presence of residual or recurrent aneurysms previously treated with endovascular coiling. In one giant aneurysm, use of intravenous contrast material did result in improved visualization of a residual aneurysm.
Selective endovascular treatment with Guglielmi detachable coils (GDCs; Boston Scientific/Target Therapeutics, Boston, MA) is increasingly being used in the management of intracranial aneurysms. The goal of this technique is to exclude the aneurysm from the circulation by filling it with platinum microcoils. The long-term occlusion rates of completely packed aneurysms have not yet been established. In some patients, the aneurysm may recur because of either coil compaction or regrowth of a residual aneurysm neck. Moreover, some aneurysms cannot be completely packed with coils, and residual filling within the interstices of the coil mass or a residual aneurysm neck is left after treatment. Subarachnoid hemorrhage has been observed in patients after subtotal GDC treatment (1). Patients treated with GDC therapy are routinely studied after therapy with conventional digital subtraction angiography (DSA) to assess the durability of the initial treatment and to determine the need for further therapy. If residual aneurysm or aneurysm regrowth is identified, retreatment is often considered. Arteriography is the most accurate means of assessing the need for further therapy.
However, DSA is expensive, invasive, and carries some risk to the patient. Few studies have attempted to evaluate the potential place of MR angiography in this follow-up (2–8). They indicate that a noninvasive technique such as 3D time-of-flight (TOF) MR angiography could be an important adjunct in this follow-up and could partly replace DSA. Some of these studies have used contrast material in combination with 3D TOF MR angiography to increase signal intensity in residual pouches, whereas others did not use contrast material. The objective of our study was to compare prospectively 3D TOF MR angiography, gadolinium-enhanced 3D TOF MR angiography, and DSA to determine the usefulness of contrast material in addition to 3D TOF MR angiography in the follow-up of intracranial aneurysms treated with GDCs.
Methods
Patient Population
Fifty-eight patients (11 men and 47 women; mean age, 52 years) harboring a total of 71 cerebral aneurysms previously treated with GDCs were prospectively entered into the study. In two cases (one aneurysm arising from the top of the basilar artery and one carotid-ophthalmic aneurysm), wide-neck aneurysms were treated with assistance from a neck-bridge device (GDC TriSpan coil; Target Therapeutics/Boston Scientific, Fremont, CA). Forty-nine patients had subarachnoid hemorrhage. In the remaining patients, the aneurysms were discovered incidentally or because of symptoms caused by their mass effect.
The locations of the aneurysms were as follows: anterior communicating artery in 23 cases (32%), internal carotid artery and communicating posterior artery in 29 cases (41%), and middle cerebral artery in five cases (7%). Fourteen aneurysms (20%) were located in the posterior circulation: basilar artery, posterior cerebral artery, and superior cerebellar artery in seven cases (10%); posterior inferior cerebellar artery and vertebral artery in seven cases (10%). The size of the aneurysm was 3 mm or smaller in 21 cases (30%), 4–7 mm in 28 cases (39%), 8–14 mm in 12 cases (17%), 15–20 mm in six cases (9%), and larger than 20 mm in four cases (6%).
Follow-up MR angiography was performed within 1 week before DSA. The interval between treatment and DSA follow-up studies ranged from 3 months to 4 years, with a median follow-up period of 12 months.
MR Imaging Techniques
MR examinations were performed with a 1.5-T unit (Signa; GE Medical Systems, Milwaukee, WI). In the standardized study performed with the head coil, sagittal T1-weighted gradient-echo and axial T2-weighted fast spin-echo sequences were performed. Imaging parameters for the T1-weighted gradient-echo sequence were 275/6 (TR/TE), flip angle 90°, 224 × 512 matrix, 22-cm field of view, 5-mm-thick sections. Parameters for the T2-weighed fast spin-echo sequence were 4400/120, 256 × 320 matrix, 22-cm field of view, 5-mm-thick sections with a 0.5-mm intersection gap. For the selected 3D TOF MR angiographic sequence, the imaging parameters were as follows: spoiled gradient-echo sequence, 38/6.9, flip angle 30°, 224 × 512 pixel matrix, 22-cm field of view, 46 partitions, 1.2-mm section thickness, magnetization transfer, one acquisition, and an acquisition time of 4 minutes 57 seconds. A second 3D TOF MR angiographic examination was performed immediately after manual injection of 0.2 mL of gadotenique acid (Dotarem; Guerbet, Villepinte, France) per kilogram of body weight with use of the same parameters.
DSA Technique
DSA was performed with an Advantx unit (GE Medical Systems) with a matrix of 1024 × 1024. Selective catheterization of the vessel harboring the aneurysm was performed by using a 4F or 5F catheter with the femoral approach. Eight to ten milliliters of nonionic contrast material (iobitridol, Xenetix; Guerbet, Roissy, France) was injected into the internal carotid or vertebral artery with a power injector at 4–5 mL/s. DSA before treatment included multiple views. Only the best views that showed the aneurysm during initial DSA were acquired at DSA follow-up.
Image Interpretation
All MR angiograms were postprocessed off-line on a workstation (Advantage Windows 3.1; GE Medical Systems). MR angiographic source images and standard and targeted maximum intensity projection (MIP) reconstructions were interpreted in a blinded fashion by two trained radiologists (J.P.C., A.B.C.) without knowledge of the contemporary DSA findings. Cases leading to a disagreement between the observers were reviewed by both readers to reach a consensus. Another author (D.H.) performed the DSA examinations and assessed the resultant images. DSA was regarded as the standard of reference. The findings at each examination were assessed by using the following classification: complete occlusion or remnant size (height of the remnant evaluated by means of direct measures on the MR angiograms and of comparison with the diameter of the internal carotid artery or the basilar artery at DSA) 3 mm or smaller, 4–5 mm, or larger than 5 mm. The study also evaluated for parent and adjacent artery patency and venous overlap. Patency of the parent artery and adjacent arteries was assessed by using both axial 3D TOF source images and MIP reconstructions. The artery was graded as normal in cases of regular outlines or abnormal in cases of stenosis or occlusion involving the artery in whole or in part. Venous overlaps were judged as minor when they did not prevent the interpretation of images and major when they degraded the image quality.
Results
MR Angiographic Quality
In only one of the 58 patients for whom MR angiography was recommended were 3D TOF and contrast-enhanced 3D TOF MR angiograms not informative. The patient had a recurrent vertebral aneurysm after surgical clipping. Artifacts were responsible for the poor quality of the MR angiograms, which did not enable evaluation of the aneurysm secondarily treated with coils.
Assessment of the quality of the aneurysm occlusion on MR angiograms was judged possible in all other patients. Venous overlaps were present on all contrast-enhanced MR angiograms (especially at the cavernous sinus) and on none of the nonenhanced images. Nevertheless, venous overlaps were considered as minor because venous enhancement did not prevent the interpretation of the arterial images (Fig 1).

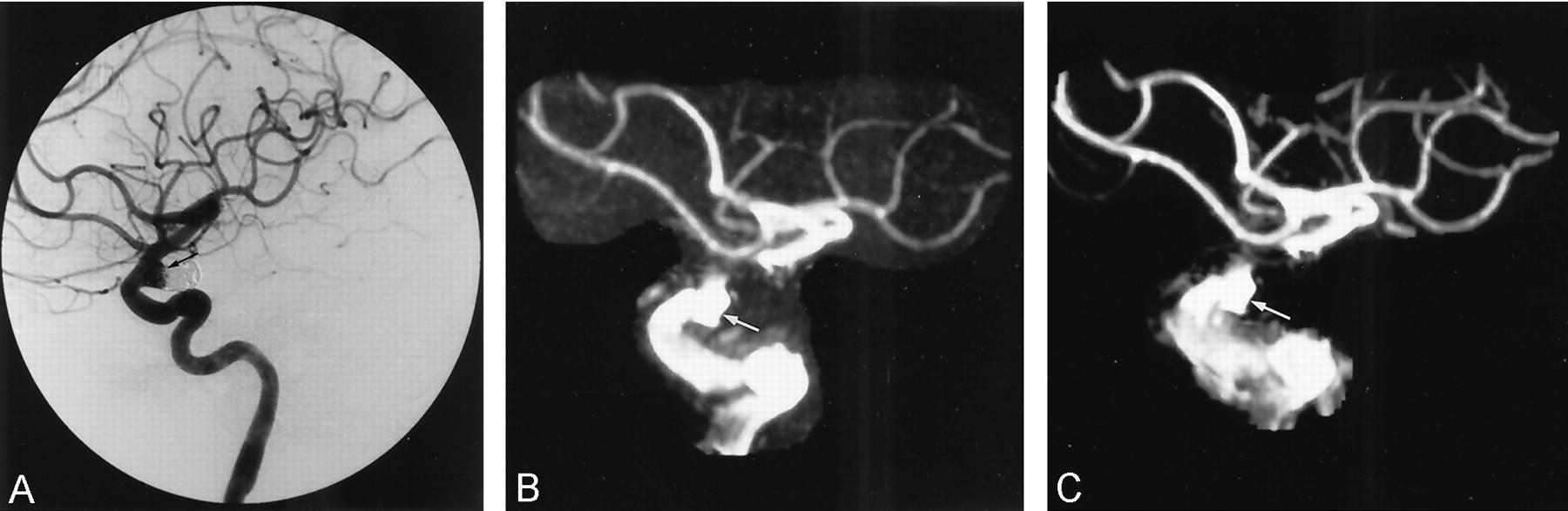
Recurrent communicating posterior aneurysm partially treated initially with a surgical clip and secondarily with coils.
A, DSA lateral projection image obtained 1 year after GDC treatment shows an aneurysm remnant (arrow).
B and C, Three-dimensional TOF (B) and contrast-enhanced 3D-TOF (C) images obtained with MIP reconstruction depict the same remnant cavity (arrow). On both MR angiograms, loss of signal intensity is noted at the internal carotid artery level above the aneurysm due to an artifact from the surgical clip. On the contrast-enhanced 3D TOF image, there is a enhancement of the cavernous sinus that does not preclude aneurysm analysis.
Comparison of MR Angiographic and DSA Findings
The frequency and size of residual flow in 70 coiled aneurysms are summarized in the Table. Aneurysm remnants were revealed in 36 DSA studies (51%). The addition of contrast material at 3D TOF MR angiography did not improve the ability of MR angiography in depicting a residual neck. Six minor remnant necks (≤ 3 mm) were not detected with either 3D TOF MR angiography or contrast-enhanced 3D TOF MR angiography (Fig 2), whereas all aneurysm remnants detected with MR angiography were seen with DSA. Thus, the sensitivity of MR angiography compared with DSA was 83%, specificity 100%, positive predictive value 100%, and the negative predictive value 85% for depicting an aneurysm remnant. In two cases, both 3D TOF MR angiography and contrast-enhanced 3D TOF MR angiography depicted residual flow in the aneurysms, but underestimated the remnant size in comparison with findings at DSA. However, even if contrast material injection did not modify our classification of residual intraaneurysmal flow on MR studies, in one case of large recanalization in a giant aneurysm (25 mm diameter) contrast-enhanced images allowed for better evaluation of the remnant size (Fig 3). In this case, the two examiners concluded that the two MR angiographic examinations provided the same result according to our classification (recanalization size 5 mm).

Discrepancy between DSA and MR angiography.
A, DSA oblique projection image of the right internal carotid artery obtained 3 months after treatment of a aneurysm in the anterior communicating artery shows a 2-mm remnant in the aneurysm neck (arrow).
B and C, Three-dimensional TOF (B) and contrast-enhanced 3D TOF (C) images with MIP reconstruction in the frontal view do not depict the aneurysm remnant.

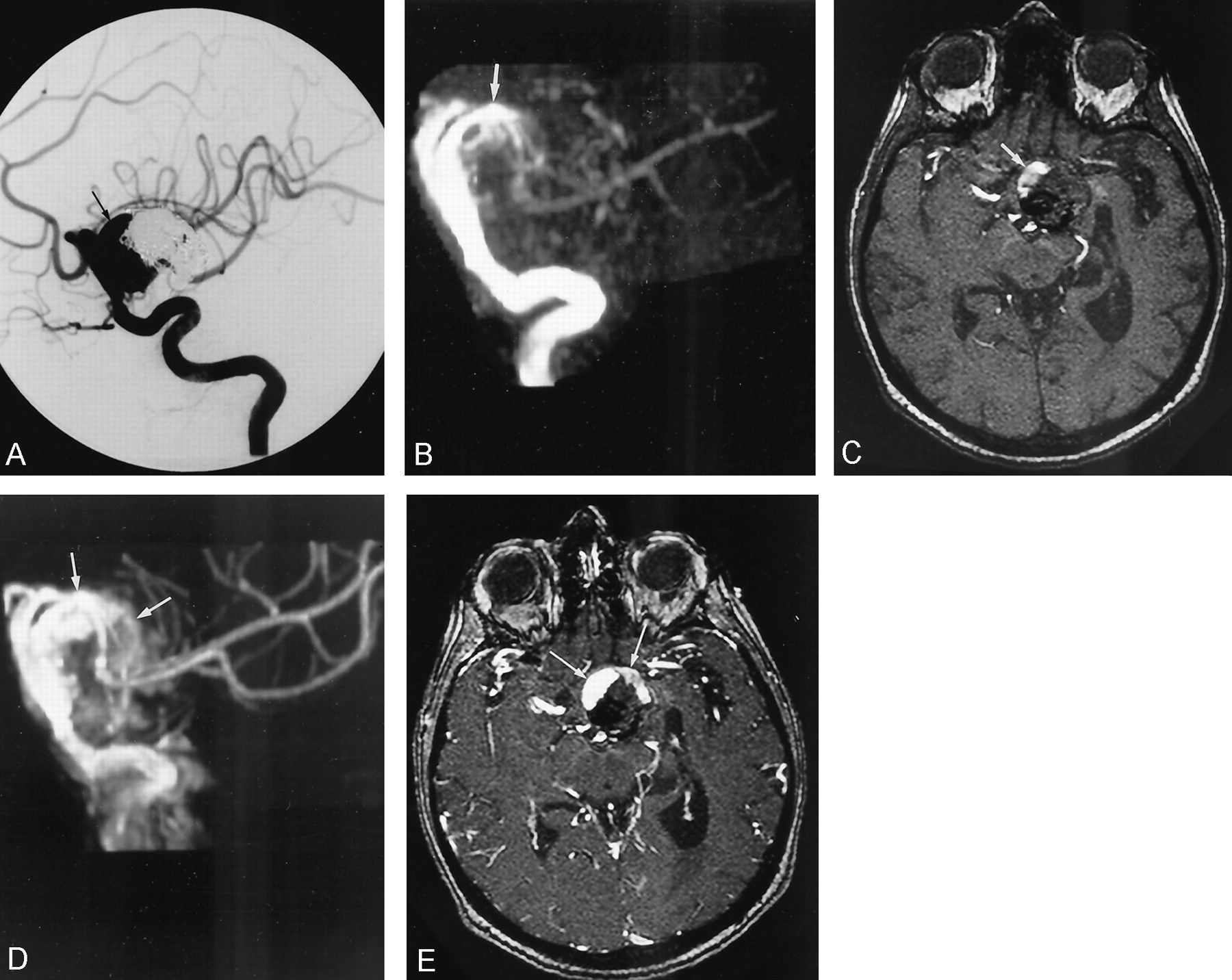
Ruptured giant internal carotid artery aneurysm partially treated with endovascular placement.
A, DSA image, lateral projection, after left internal carotid injection obtained 3 months after treatment shows the partially packed aneurysm (arrow).
B and C, Lateral MIP reconstruction (B) and axial 3D TOF source MR angiogram (C) underestimate the size of the aneurysm remnant (arrow).
D and E, Contrast-enhanced lateral MIP reconstruction (D) and axial 3D TOF source MR angiogram (E). Contrast material administration allows a better delineation and identification of the aneurysm remnant (arrows).
MR angiographic performance in the detection of a residual flow after GDC treatment in 70 aneurysms
In six cases (9%), both 3D TOF MR angiography and contrast-enhanced 3D-TOF MR angiography depicted abnormalities in the parent vessel (encroachment or loss of signal intensity) visible on DSA images; but in 18 cases (26%) 3D TOF MR angiography and contrast-enhanced 3D TOF MR angiography showed anomalies not seen at DSA. In the two cases of wide-neck aneurysms treated with the aid of a GDC TriSpan coil (neck-bridge device), susceptibility artifact was very important, causing loss of signal intensity in parent and adjacent arteries (Fig 4). The sensitivity and specificity of 3D TOF MR angiography and contrast-enhanced 3D TOF MR angiography were, therefore, 72% and 100%, respectively, for assessment of patency of the parent artery and adjacent arteries.

Wide-neck basilar tip aneurysm treated with assistance from a neck-bridge device.
A, DSA image (Towne projection) after right vertebral artery injection shows the aneurysm before embolization.
B and C, DSA images (Towne projection) obtained 1 year after embolization show subtotal occlusion of the aneurysm. There is only a 2-mm remnant neck (arrow in C), with patency of the left posterior artery.
D, Nonsubstracted DSA image after left vertebral artery injection. The arrow points to the stem marker of the neck-bridge device used during treatment.
E and F, Both 3D TOF (E) and contrast-enhanced 3D TOF (F) images obtained with MIP reconstruction depict the small remnant neck (arrow). Loss of signal intensity is noted at the origin of the posterior cerebral and superior cerebellar arteries surrounding the Trispan coil stem. The addition of contrast material does not improve the quality of the images.
Discussion
All patients with aneurysms treated with GDCs are followed up angiographically to assess the long-term stability of aneurysm exclusion or to diagnose recurrence of the aneurysm sac, which can require a new treatment. Usually, this follow-up is conducted by performing DSA at 3 months, 1 year, and 3 years after treatment (9). In fact, the most useful duration of follow-up is unknown since coiling is a relatively new technique and it is difficult to determine the clinical importance of an aneurysm remnant or a small recurrence. DSA has a risk of neurologic complications, which are estimated to occur in 0.5–1.7% of cases (10, 11). This rate of morbidity and mortality is similar to or greater than the rate of rebleeding (1–3%) reported in large series treated with GDCs (1, 12, 13).
Unlike DSA, MR angiography provides noninvasive intracranial vascular imaging (14). Preliminary studies have shown the potential of 3D TOF MR angiography for depicting an aneurysm remnant. Published studies (2–6, 7) have shown that the sensitivity of 3D TOF MR angiography without contrast material in revealing residual flow within the aneurysm ranged from 71% to 91% and the specificity in ruling out residual flow ranged from 89% to 100%. False-negative examinations were explained by the presence of slow flow in the aneurysm (2) with a saturation phenomenon, turbulence creating intravoxel dephasing (5), or magnetic susceptibility artifact of the coil mass (14). False-positive examinations were related to the presence of artifacts or intra- or extraluminal blood clot interpreted as flow at MR angiography (2).
Some authors have suggested the use of a short TE to minimize the intravoxel spin-dephasing artifacts (2, 3). Thus, Gönner et al (3) have shown that use of an ultrashort TE, 3D TOF sequence may reduce the GDC-induced signal intensity dropout and improve the ability of MR angiography to assess vessels adjacent to an aneurysm. However, for detectability of residual aneurysm flow, which is the main interest of MR angiography, the reduction in TE had no advantage over conventional 3D TOF MR angiographic sequences. To reduce saturation effects, a few authors have proposed the use of contrast material in addition to 3D TOF MR angiography. The goal is to increase signal intensity in residual pouches where flow can be slow (7). Anzalone et al (6) used contrast material, but in that study only a few patients were evaluated both before and after administration of contrast material. They noted that contrast material administration was useful only for giant aneurysms in which the extent of recanalization was more evident on contrast-enhanced images. In the largest study of follow-up of intracranial aneurysms treated with GDCs, Boulin and Pierot (7) evaluated gadolinium-enhanced 3D TOF MR angiography versus DSA, with a good correlation between the two modalities (sensitivity 72%, specificity 98%). Nevertheless, the value of contrast material administration was not demonstrated in that study, since none of the MR angiograms were obtained without contrast material. Gadolinium-based contrast material has also been used with other MR angiographic sequences, such as dynamic 3D contrast-enhanced T1-weighted MR angiography, in preliminary reports (15, 16). This technique allowed the use of a large imaging volume with a short acquisition time; high signal intensity in the vascular structures resulted from major shortening of the T1 in blood because of gadolinium-based contrast agent. Images were more similar to those obtained at DSA; on theses images, the signal intensity in the vascular lumen depended on the vascular concentration of the gadolinium-based contrast agent at the time of image acquisition. The combination of a very short TE with a high concentration of contrast agent at the first pass made these arterial images less prone to signal intensity losses to turbulence or flow saturation effects. In the study of Leclerc et al (16), coils artifacts seemed less apparent on contrast-enhanced MR angiograms compared with those on TOF MR angiograms, and this difference was probably due to the shorter TE, which decreases magnetic susceptibility artifacts. The number of patients in that study was limited, however, and only aneurysms of the anterior communicating artery previously treated with endovascular coiling were assessed.
In our study, we did not find any difference between 3D TOF MR angiography before and after contrast material injection in its ability to depict aneurysm recanalization. Among 70 studies, both MR techniques missed six small remnant necks (≤ 3 mm), whereas all residual sacs detected with MR angiography were seen at DSA. Both 3D TOF MR angiographic examinations had a sensitivity and specificity of 83% and 100%, respectively. Hartman et al (14) showed that the coils produced magnetic susceptibility artifacts, with obscuration of approximately 2 or 3 mm around the coil mass. This source of a false-negative examination is probably not modified by the adjunct of a contrast agent at the 3D TOF sequence. In one case of large recanalization of a giant aneurysm, the contrast-enhanced sequence provided better evaluation of the remnant sac size. The addition of contrast material, which shortens T1 and reduces saturation, could help to identify regions of slow flow, providing better definition of the residual sac (6, 17). However, in this case, the two examiners concluded that the two MR angiographic techniques provided the same result according to our classification (recanalization size 5 mm), leading to a repeat DSA with retreatment. On this subject, one limitation of our study is the small number of large or giant aneurysms (only 10 aneurysms 15 mm in diameter), but our findings agree with those of Anzalone et al (6) on treated giant aneurysms and with the results of a previous study concerning untreated giants aneurysms (17).
We also failed to find a difference between 3D TOF MR angiography before and after contrast material injection for analyzing patency of parent and adjacent arteries in the vicinity of the aneurysm. In the two cases of wide-neck aneurysm treated with an adjunctive neck-bridge device (GDC TriSpan coil), we observed a significant loss of signal intensity around the coils. This neck-bridge device is made of three nitinol loops partly covered by platinum coils (18). The loops are fixed together at their struts, and the stem coil may project into the parent artery. The nitinol may be responsible for important magnetic susceptibility artifacts.
In our study, venous overlaps were considered minor, and they did not impair vessel delineation. Nevertheless, the use of contrast-enhanced conventional sequences is not recommended for cavernous internal carotid artery aneurysms or for aneurysms located near the base of the skull because enhancement of veins would interfere with evaluation of adjacent arterial vessels (6).
Conclusion
Contrast material is not useful in addition to 3D TOF MR angiography in the follow-up of intracranial aneurysms treated with GDCs, except for giant aneurysms in which contrast material may provide better evaluation of a residual sac.
However, in preliminary reports, gadolinium-based contrast material has been used with other MR angiographic sequences such as dynamic 3D contrast-enhanced T1-weighted MR angiography (15, 16). The combination of a high concentration of contrast agent at the first pass with a very short TE demonstrated a relative insensibility to artifacts, and thus it could become a promising technique in the follow-up of patients treated with GDCs.
References
- Received December 6, 2002.
- Accepted after revision April 13, 2003.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- MRA versus DSA for the follow-up imaging of intracranial aneurysms treated using endovascular techniques: a meta-analysis
- MRA Versus DSA for Follow-Up of Coiled Intracranial Aneurysms: A Meta-Analysis
- Outcomes of Endovascular Treatments of Aneurysms: Observer Variability and Implications for Interpreting Case Series and Planning Randomized Trials
- Residual Flow After Cerebral Aneurysm Coil Occlusion: Diagnostic Accuracy of MR Angiography
- Long-Term Prospective Follow-Up of Intracranial Aneurysms Treated with Endovascular Coiling Using Contrast-Enhanced MR Angiography
- MR Angiography Follow-Up of Aneurysms Treated with Coils: Is There a Need for the Use of Gadolinium?
- MR Angiographic Follow-Up of Intracranial Aneurysms Treated with Detachable Coils: Evaluation of a Blood-Pool Contrast Medium
- Intracranial Aneurysms Treated With Endovascular Coils: Detection of Recurrences Using Unenhanced and Contrast-Enhanced Transcranial Color-Coded Duplex Sonography