
Abstract
Summary: We present a case of an 85-year-old woman with a 40-year history of progressive bilateral sensorineural hearing loss. Imaging studies demonstrated bilateral pseudoaneurysms of the petrous portion of the internal carotid arteries eroding into both cochleas. To our knowledge, this is the first case report of such lesions.
Pseudoaneurysms of the petrous internal carotid artery (ICA), although uncommon, have been described in the literature (1, 2). Presenting symptoms of these pseudoaneurysms are varied, depending on the adjacent structures and vessels involved. We report a case of bilateral petrous ICA pseudoaneurysms eroding into both cochleas presenting with bilateral sensorineural hearing loss, which to our knowledge has not been previously reported.
Case Report
An 85-year-old woman presented to the otolaryngology clinic at our institution for evaluation of progressive bilateral hearing loss. Although she had a 40-year history of bilateral hearing loss, audiograms documented a deterioration of hearing in the right ear within the past year. She denied tinnitus, vertigo, or recent ear infections. She denied any significant head injuries in the past. Medical history was significant for an untreated growth hormone-secreting pituitary adenoma. On examination, she had significant acromegalic features, bilateral hearing loss, and bitemporal hemianopsia.
Audiography showed severe to profound sensorineural hearing loss in the right ear with a mild, sloping to severe sensorineural loss on the left. High-resolution (1.25-mm section thickness) coronal and axial CT examinations of the temporal bones were obtained, which revealed erosive lesions involving the petrous bone bilaterally, along the posteromedial wall of the horizontal carotid canals. Lucency was also seen extending from the petrous carotid canal to the cochlea with erosion of the basal and apical turns of the cochlea bilaterally (Figs 1 and 2). The right-side lesion was larger than the left, with more significant erosion of the cochlea. The vestibule, semicircular canals, and internal auditory canals were normal. There was no enlargement of the vestibular aqueduct. MR imaging was performed, revealing questionable flow-related enhancement in these lesions. A diagnostic cerebral angiogram was obtained, which revealed bilateral 5–6-mm aneurysms in the petrous carotid arteries corresponding in location to the CT abnormalities. Subtle changes in diameter were seen in the cervical internal carotid arteries bilaterally, suggesting that these findings represented sequela of remote dissections. An incidental 3-mm right middle meningeal artery aneurysm was also noted.

Axial (A) and coronal (B) CT images acquired through the temporal bone demonstrate an erosive lesion involving the right petrous carotid canal posteromedially with erosion into the cochlea (black arrowhead). The horizontal petrous carotid canal is indicated by the white arrow. Similar changes were seen on the left.

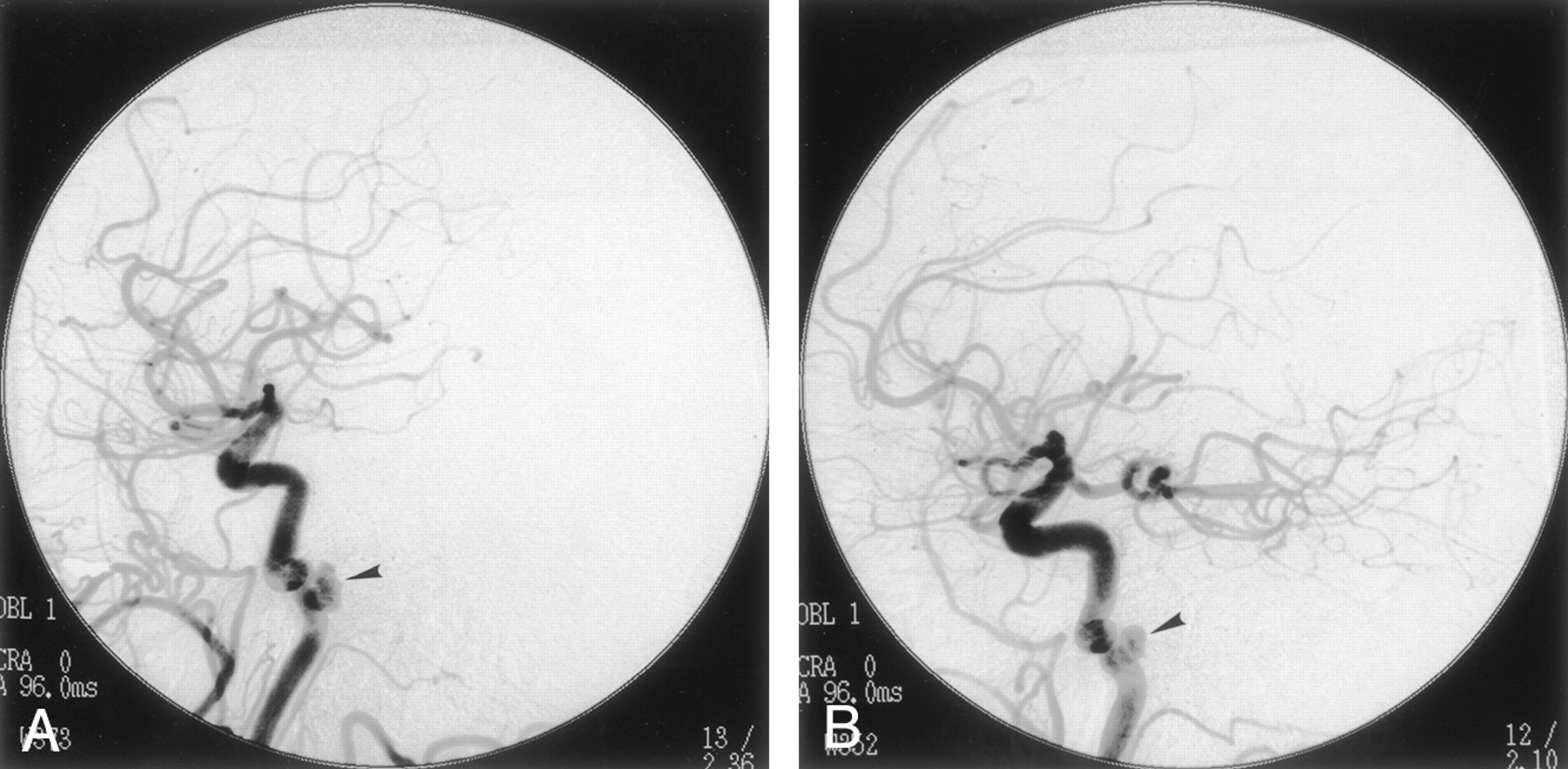
Images from right (A) and left (B) common carotid artery injections demonstrate bilateral aneurysms of the horizontal petrous carotid arteries (black arrowhead).
Because of the patient’s age and the presence of bilateral ICA pseudoaneurysms, conservative management was chosen.
Discussion
Vascular lesions involving the petrous segment of the extradural ICA are uncommon. In large part, the rarity of lesions involving the petrous ICA results from the well-protected course of the vessel within the carotid canal, the absence of branches from this portion of the vessel, and the uncommon involvement of the petrous ICA by atheromatous changes. Nevertheless, the anatomic arrangement of the cervico-petrous junction of the ICA may predispose to injury from blunt trauma. As the relatively mobile cervical portion of the ICA enters the carotid canal, the vessel is fixed to the skull base, an arrangement that permits stretching forces to be transmitted to the vessel wall by excessive head movement around the atlanto-occipital joint. Although most often resulting in dissection of the cervical ICA, such forces may also damage the petrous ICA with traumatic pseudoaneurysm formation, the most common cause of petrous aneurysm in most series (3).
A pseudoaneurysm, or false aneurysm, develops when a fibrous tissue capsule forms in response to injury to all layers of an arterial wall (eg, after trauma, surgery, infection, or vasculitis). Such injury may result from a number of mechanisms, including blunt or penetrating trauma, infections, or inflammatory conditions. Although most often resulting from blunt trauma, pseudoaneurysms involving the petrous ICA have been described as rare sequelae of vessel injury from pituitary and sinus surgery as well as from gunshot wounds (1, 4). Mycotic aneurysms of the petrous ICA have also been reported from bacterial and fungal infections (2, 5). The lack of structural integrity of the wall of a pseudoaneurysm often permits rapid expansion and may suggest the cause.
Several reports of rapidly enlarging petrous aneurysms in children have documented involvement of other arterial structures or associated anomalies. Such cases may suggest congenital disorders, including neurofibromatosis (6, 7). Connective tissue disorders such as Marfan syndrome and fibromuscular dysplasia may also be associated with the development of pseudoaneurysms, although involvement of the petrous ICA has not been documented (8).
The presence of a pseudoaneurysm may be demonstrated on CT or MR images. In the case of our patient, the pseudoaneurysm presented as an erosive petrous bone mass on CT images. The differential diagnosis of petrous lesions includes cholesterol granuloma, cholesteatoma, mucocele, chondrosarcoma, granulation tissue, and pseudoaneurysms. The MR imaging appearance of pseudoaneurysm may mimic cholesterol granuloma or mucocele (9). Conventional angiography remains the reference standard for diagnosing vascular lesions such as pseudoaneurysms.
The presenting symptoms of pseudoaneuryms vary depending on the vessels involved and adjacent structures. Symptoms associated with petrous ICA pseudoaneurysms include headache, nasal congestion, and midface pressure and pain (2). A ruptured petrous ICA aneurysm may occur with otorrhagia, epistaxis, and neurologic deficit (10). Sudden sensorineural hearing loss has also been associated with aneurysms (11). Other vascular causes of sensorineural hearing loss are microvascular insufficiency, arteriovenous malformations, vertebrobasilar artery dolichoectasia, thrombosis, and vascular loops (12). The sensorineural hearing loss in these cases is postulated to be a result of cranial nerve VIII compression and dysfunction. Conductive hearing loss in association with a petrous ICA aneurysm has also been reported (13, 14).
Although cranial nerve VIII dysfunction may play a role in our patient’s sensorineural hearing loss, we suspect that it resulted from erosion of the pseudoaneurysm into the cochlea, as seen on CT and MR imaging. Our patient’s sensorineural hearing loss was progressive, reflecting the slow erosion of the cochlea from the pseudoaneurysms. In contrast, the sensorineural hearing loss described in other case reports was usually sudden and associated with recent trauma. In our patient, there is no known history of head trauma; however, in light of the changes in the diameter of cervical internal carotid arteries and an additional aneurysm in the right middle meningeal artery, we suspect that these pseudoaneuryms are the result of remote dissection.
The management of petrous aneurysms is challenging. The primary goals of treatment for petrous aneurysms are to provide symptomatic relief and to minimize the risks of hemodynamic compromise to the cerebrovascular circulation, thromboembolism, and hemorrhage. Treatment of petrous aneurysms was originally limited to rare instances amenable to surgical clip placement or vessel sacrifice versus conservative management (15). More recently, endovascular treatment has become the most often used technique, with sacrifice of the vessel following balloon occlusion testing or endovascular stent placement to preserve the vessel (14, 16, 17). The safety of treatment depends on the anatomy of the aneurysm and segment involved as well as the presence of collateral flow to the brain and the age of the patient. In this case, treatment options were discussed and conservative management was chosen, because there were bilateral ICA aneurysms and the patient was elderly.
Conclusion
Petrous ICA pseudoaneurysms are rare, with only a few case reports in the literature. To our knowledge, this is the first case of bilateral petrous ICA pseudoaneurysms eroding into the cochlea presenting as progressive bilateral sensorineural hearing loss. Thus, in cases of progressive sensorineural hearing loss, a vascular cause such as a pseudoaneurysm should be considered in the differential diagnosis. Imaging studies are integral in evaluating this association.
References
- Received July 24, 2002.
- Accepted after revision October 18, 2002.
- Accepted after revision October 18, 2002.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.