
Abstract
Summary: Infiltrating spinal epidural angiolipoma is an uncommon benign tumor composed of mature adipose elements admixed with abnormal blood vessel, which tends to invade the surrounding soft tissue and may potentially be mistaken for an aggressive tumor. In this report, we present the MR imaging findings of a pathologically proved infiltrating spinal epidural angiolipoma that appeared largely hypointense on T1-weighted images and enhanced strongly with IV injection of contrast medium, features that suggested a malignant tumor.
Spinal extradural angiolipoma is a rare pathologic entity and usually is benign and noninfiltrating. The noninfiltrating spinal angiolipomas occur mostly in the posterior spinal epidural space and have no tendency to involve the surrounding tissues. Previous reports have shown the tumor to be hyperintense on T1-weighted images and usually inhomogeneous in signal intensity (1–4). For infiltrating type spinal epidural angiolipomas, surgical findings and histopathologic features have been reported but MR imaging features have not been described. We herein present the MR imaging findings and pathologic features of an infiltrating spinal epidural angiolipoma with extra-spinal extension in the thoracic area. The tumor appeared heterogeneous in signal intensity on T1-weighted images and locally invasive into the surrounding soft tissue, suggesting a malignant tumor.
Case Report
An 81-year-old man presented with unstable gait and weakness of the lower limbs that had been progressive for 2 weeks. The patient had no history of trauma or urinary incontinence. No evidence of fever or chills had been noted recently. A neurologic examination revealed moderate symmetrical weakness in the lower limbs. Sensory impairment was noted below the T7 level. Deep tendon reflexes were hyperactive, and Babinski responses were negative. MR imaging of the thoracic spine showed an intraspinal extradural mass located in the posterior epidural space at the level of T3 through T5, extending further to the right paraspinal space via the right neural foramen. The T4−T5 neural foramina bilaterally were expanded, with focal bony destruction of the right T4 pedicle observed near the demifacet region by the tumor. The mass caused near total obstruction of the spinal canal with severe compression of the cord at the T4 level. The signal intensity of the mass was inhomogeneous in hypointensity on T1-weighted images (517/21/2 [TR/TE/number of excitations]) (Fig 1A) and strongly enhanced with IV injection of contrast medium on fat-saturated T1-weighted images (649/19/2 [Fig 1B–D]). On fat-saturated T2-weighted images (4680/122/2), the tumor showed high signal intensity with internal linear hypointense foci (Fig 1E). According to the location and the MR imaging features of the tumor, our initial diagnosis preoperatively was epidural metastasis from tumor elsewhere in the body, with lymphoma and neurogenic tumor being in the differential diagnosis list.


Signal intensity of mass was inhomogeneous in hypointensity on T1-weighted images and strongly enhanced with IV injection of contrast medium on fat-saturated T1-weighted images. On fat-saturated T2-weighted images, tumor showed high signal intensity with internal linear hypointense foci.
A, Unenhanced sagittal view T1-weighted MR image (517/21/2) shows extradural mass located in posterior epidural space at level of T3 extending to T5 (arrows). Mass displays inhomogeneous predominately low signal intensity mixed with intermediate signal intensity content.
B, Contrast-enhanced sagittal view T1-weighted MR image (649/19/2) with fat saturation technique shows marked enhancement of mass.
C, Contrast-enhanced coronal view T1-weighted MR image (649/19/2) with fat saturation technique well delineated extent of enhancing tumor along neural foramen bilaterally, more prominent on right side.
D, Contrast-enhanced axial view T1-weighted MR image (649/19/2) with fat saturation technique shows involvement of tumor in right demifacet region of T4 vertebra (arrows).
E, Fat-saturated T2-weighted MR image (4680/122/2) shows tumor to have high signal intensity with internal linear hypointense foci.
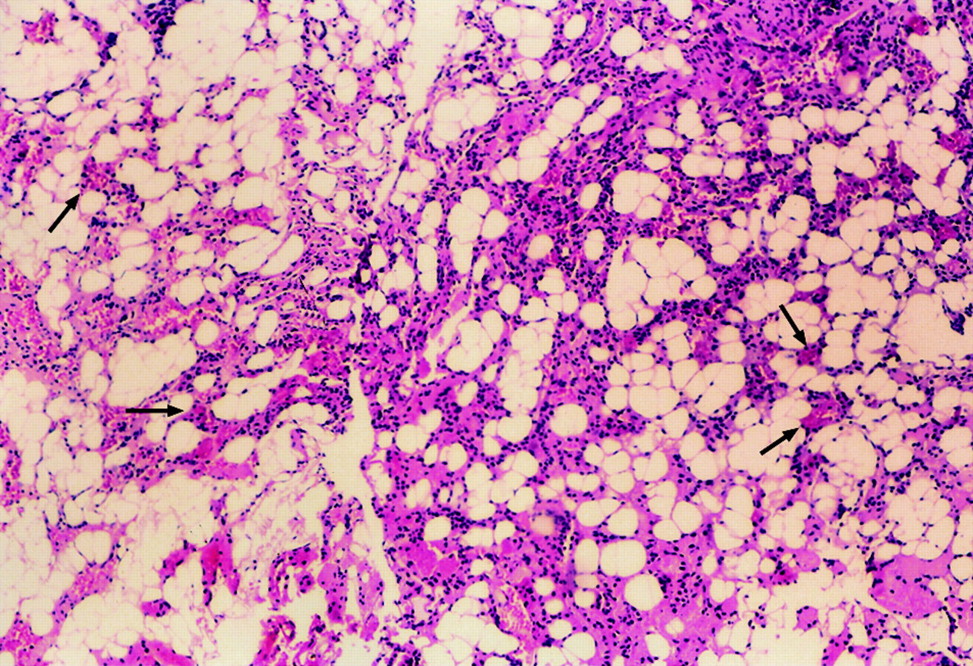
The patient underwent T3−T5 laminectomy. During surgery, the epidural mass was poorly demarcated and easily bled. It appeared hypervascular, with extension to the paraspinal region via neural foramen, and caused destruction of the proximal portion of the right fourth rib and the demifacet of the right T4 vertebra. Invasion of the surrounding soft tissue was also noted. Total removal was impossible because of the infiltrating nature of the mass. However, decompression of the spinal cord was undertaken. The histopathologic examination revealed the tumor to be composed of mature adipose tissue and blood vessels (Fig 2). No evidence of mitosis or malignancy was noted. The diagnosis of angiolipoma was confirmed. At the 2-month follow-up examination, the patient was shown to have improved gradually after surgery.

Histomicrograph of the surgical specimen shows a characteristic angiolipoma composed of mature adipose tissue and blood vessels (arrows) (hematoxylin and eosin; original magnification, ×100).
Discussion
Spinal angiolipoma is a rare benign tumor. Berenbruch first described a case of spinal angiolipoma in 1890. The extensive study of angiolipomas presented by Howard and Helwing (5) in 1960 established angiolipoma as an anatomopathologic entity containing vascular and mature adipose elements. The most common locations of angiolipomas were in the soft tissues of the extremities, trunk, or neck. Spinal angiolipomas are rare benign spinal neoplasms and account for between 0.14% and 1.2% of all spinal tumors, 3% of extradural spinal tumors, and 24% of spinal lipomas (6).
Angiolipomas are classified as a subgroup of lipomas and have been referred to by various terms, including hemangiolipoma, angiomyolipoma, vascular lipoma, and fibromyolipoma (1). The cause of spinal angiolipomas is unknown. They probably originate from the same progenitor tissue as lipomas and hemangiomas and have two features common to both. They may represent an intermediate stage between the two extremes (6).
Angiolipomas can be further categorized into two subtypes: noninfiltrating and infiltrating (7). The former type is more common and is usually well encapsulated. Clinically, the noninfiltrating angiolipoma is seen in young persons and presents as painful, soft, subcutaneous nodules. The infiltrating angiolipomas are rare. They usually involve the extremities and may extensively infiltrate into the surrounding tissues, such as bones, muscles, nerves, and fibrocollagenous tissues. Spinal infiltrating angiolipomas are generally located in the anterior epidural space. In 1990, Kuroda et al (8) reported a case of infiltrating spinal angiolipoma extensively infiltrating into the vertebral body and the epidural space, resembling the behavior of vertebral hemangioma. In our case, the uncommon location of the tumor in the posterior epidural compartment was of interest. The tumor extended to the right paraspinal space via right neural foramen and involving the proximal portion of right fourth rib. Therefore, the infiltrating behavior of spinal angiolipomas may in part be related to the degree of tumor vascularity, as in our case in which there was rich vascularity with strong contrast enhancement.
The spinal extradural angiolipoma generally arises from the posterior epidural space. Intramedullary angiolipomas are extremely rare. Most of spinal angiolipomas are located at the thoracic level and usually extend over three to four vertebral bodies (2). The lesions occur most commonly in women and generally present during the fifth decade. The frequently clinical presentations of spinal epidural angiolipomas are progressive paraparesis, back pain without radiculopathy, lower extremity sensory changes, and hyperreflexia. Often, they occur over a period of a few years. Sometimes, the symptoms onset and exacerbations have been reported during pregnancy, probably because of impaired spinal venous drainage or hormonal changes (1).
MR imaging appearances of noninfiltrating spinal angiolipomas have been reported. These lesions are typically hyperintense on T1-weighted images and often inhomogeneous. The degree of central hypointensity on T1-weighted images is predictive of the degree of vascularity (1, 3, 4). In our case, the presence of the more hypointense foci on T1-weighted images, the behavior of the tumor extension, and the strong enhancement of the tumor with IV injection of contrast medium were indicative of the more vascular and infiltrative nature of the tumor.
Spinal angiolipomas do not typically contain vascular flow voids on MR images because of their low vascular flow characteristics, which can be distinguished from high flow arteriovenous malformations and capillary hemangiomas. On T2-weighted images, the tumors are of variable signal intensity, with hyperintensity being the more common feature. Another important finding is that the tumors usually show intense homogenous enhancement on contrast-enhanced fat-saturated T1-weighted images. Therefore, spinal angiolipomas can be differentiated from epidural lipomatosis, which are homogeneous and would not be enhanced after IV injection of contrast medium. The differential diagnoses should include spinal epidural metastases, neurogenic tumor, meningioma, lymphoma, and, rarely, tuberculoma and chloroma, according to the location and MR imaging characteristics of the tumor (9).
Total surgical removal of the tumors is the first choice for treatment of spinal noninfiltrating angiolipomas. For the infiltrating type of spinal angiolipomas, a total resection of the tumor for relief of substantial symptoms by decompressing the spinal cord can be more difficult. Most patients have a good prognosis because the tumors are usually slow growing and do not undergo malignant transformation.
References
- Received August 8, 2002.
- Accepted after revision September 11, 2002.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.