
Article Figures & Data
Figures
- Fig 1.
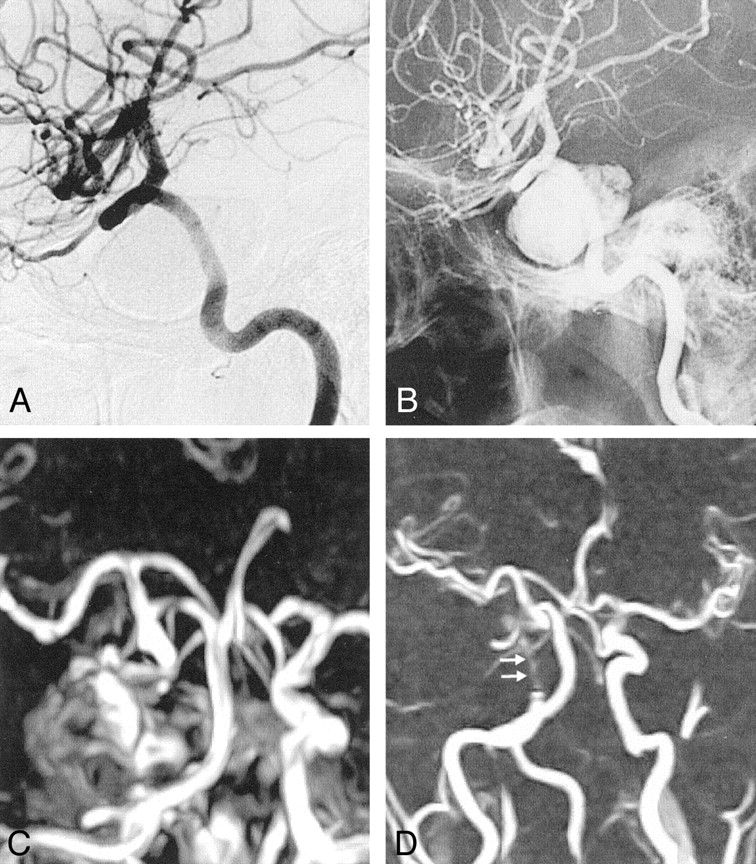
A, Pretreatment angiogram demonstrates partially thrombosed giant right ICA aneurysm.
B, Immediate posttreatment angiogram shows obliteration of the aneurysm sac with minimal filling, if any, at the neck.
C, Follow-up angiogram reveals regrowth at the neck of the aneurysm.
D, Control angiogram after retreatment with the stent and the polymer shows complete obliteration of the aneurysm.
E, Pretreatment contrast-enhanced CT image demonstrates partially thrombosed giant aneurysm with the patent portion of the aneurysm enhancing (arrow). Note the calcification at the aneurysm wall.
F and G, Nonenhanced CT images obtained after initial treatment with parenchyma (F) and bone (G) settings. Attenuating streak artifact hinders the evaluation of the parenchyma. With the bone setting, the attenuating cast of the polymer is seen extending beyond the patent portion; this finding indicates the extension of the material into the thrombus, though it does not completely fill the sac.
H and I, Corresponding T1-weighted images before (H) and after (I) treatment. The images differ in regard to the loss of pulsation artifact (arrows) and the increased hypointensity in the occluded nonthrombosed portion of the aneurysm after treatment.
J–M, Fluid-attenuated inversion recovery images (J, K) and T2-weighted turbo spin-echo images (L, M) demonstrate disappearance of the pulsation artifact (arrows). J and L were obtained before treatment, and K and M, after treatment. The hyperintense interface between the thrombosed portion and the lumen of the patent aneurysm appears thinner, possibly because of the absence of flow and consequent turbulence after treatment. Otherwise, the polymer itself does not create any signal intensity. No change in mass effect and no edema are observed after treatment.
- Fig 2.
A, Lateral left internal carotid angiogram reveals partial recanalization of the giant left ICA aneurysm that had been initially treated with GDC occlusion.
B, Left internal carotid right oblique angiogram after polymer treatment shows that the regrowth at the neck is completely occluded.
C and D, Axial T2-weighted turbo spin-echo MR images before (C) and after (D) polymer treatment. The entire aneurysm sac is hypointense after being filled; this finding includes the hypointense patent regrowth (arrowhead) and the thrombosed portion containing the GDC (arrows). The signal intensity change in the thrombosed portion may suggest penetration of the polymer into the coil mass and thrombus.
- Fig 3.
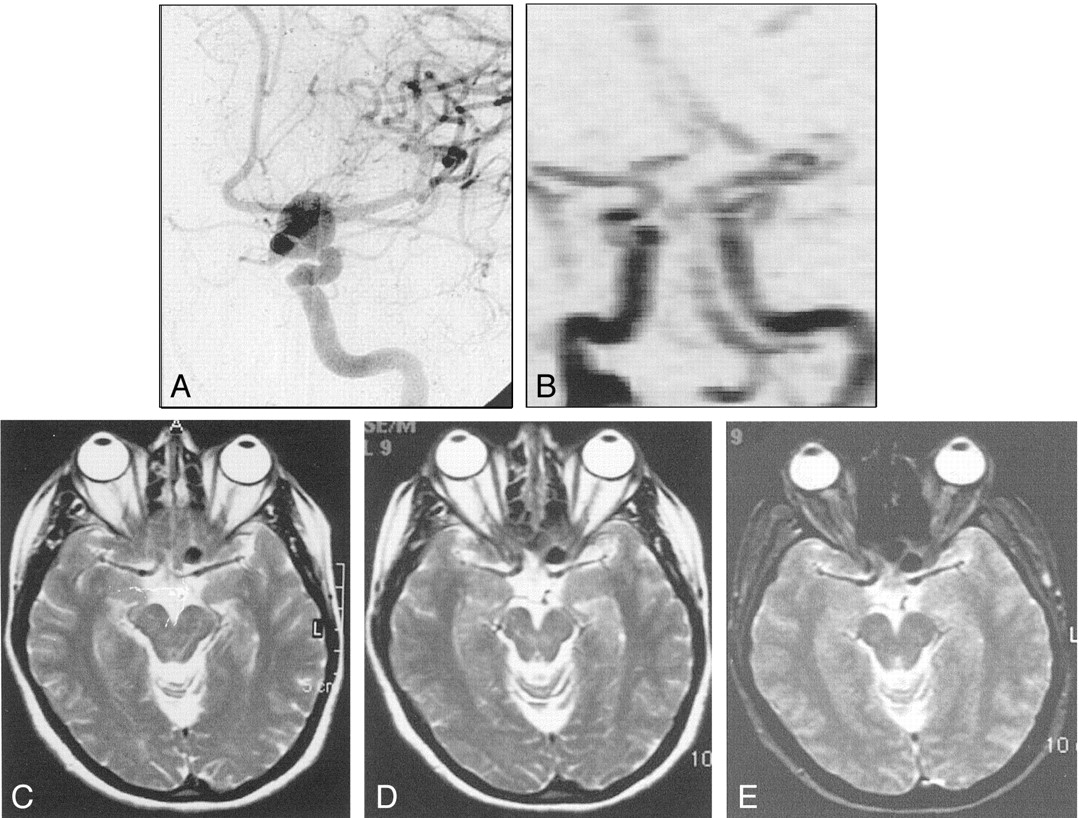
A and B, Right internal carotid angiograms obtained before (A) and after (B) treatment. Images show that the partially thrombosed giant right ICA aneurysm is almost completely occluded; it has a small residual neck.
C, Time-of-flight MRA successfully demonstrates the neck residuum (arrow). Note the slight hyperintensity due to thrombus in the region of giant aneurysm (arrowhead).
D, Pretreatment nonenhanced CT image shows the partially thrombosed giant aneurysm with surrounding edema and mass effect. Arrows indicate the thrombosed portion.
E, Posttreatment CT image (bone settings) shows that the attenuating cast of the polymer fills the aneurysm sac, except for the thrombosed portion.
F–J, Axial MR images through the same level shows the hypointensity of the aneurysm lumen becomes more prominent. The hypointensity extends into the isointense or hyperintense thrombosed portion after treatment; this may indicate the insinuation of the polymer into the thrombus in the sac. The edema and mass effect of the aneurysm persist but do not increase after treatment.
F, Pretreatment T1-weighted image. Note the pulsation artifact with the same caliber as the patent portion (arrows).
G, Posttreatment T1-weighted image.
H, Pretreatment fluid-attenuated inversion recovery image.
I, Posttreatment proton density–weighted image. The artifact disappears on this corresponding image.
J, Posttreatment T2-weighted turbo spin-echo image.
- Fig 4.
A and B, Pre- and posttreatment angiograms demonstrating large ICA aneurysm occluded completely
C–J, Corresponding pre- and posttreatment T1-weighted (C, D), fluid-attenuated inversion recovery (E, F), turbo spin-echo (G, H), and GRE (I, J) T2-weighted MR images. On the pretreatment images, the left ICA aneurysm shows increased signal intensity due to slow flow (arrow, C, E, G, I). After it was filled with the polymer, the aneurysm appears homogeneously hypointense; the appearance resembles the signal void of a patent aneurysm.
- Fig 5.
A, Pretreatment angiogram demonstrates the left ICA aneurysm.
B, Phase-contrast MRA obtained after treatment shows occlusion of the aneurysm with no compromise of the parent artery. The polymer does not create any artifact that hinders the application of MRA.
C–E, Corresponding pretreatment T2-weighted turbo spin-echo (C), posttreatment T2-weighted turbo spin-echo (D) and GRE (E) MR images show the hypointense aneurysm. It has an identical appearance before and after treatment that is not possible to appreciate if the aneurysm is patent.
- Fig 6.
MR imaging appearances of the aneurysms. Graph shows the distribution according to aneurysm size.
- Fig 7.
A and B, Post-treatment subtracted (A) and nonsubtracted (B) selective angiograms of the right ICA show complete occlusion of the aneurysm. A dense cast of the polymer fills the aneurysm. The parent artery is patent.
C and D, Time-of-flight (C) and phase-contrast (D) MRAs show complete occlusion of the giant aneurysm. The parent artery is patent but markedly narrowed (arrows) due to the presence of the stent, which results in a signal intensity loss.








Tables
Patient data
Patient, Aneurysm Location and Size* Calcification Thrombus Mass Effect† Tx/Repeat Tx‡ Examinations after First Tx New Lesion¶ Follow-Up Angiography# Recanali- zation** MRA†† CT§ MR Imaging‖ 1, R sc ICA, giant Yes Yes Yes Onyx16/ Onyx20 + S 2 3 (M) No Yes Yes Yes 2, R cav ICA, giant Yes No Yes Onyx20 + S/none 2 3 (M) No Yes No Yes 3 R cav ICA, small No No No Onyx20/onyx20 2 2 (NI) No Yes Yes Yes R cav ICA, small No No No Onyx20/none 2 2 (NI) No Yes No Yes 4, R pcav ICA, giant No Yes Yes Onyx20 + S/none 1 1 (M) Asymptomatic No NA No 5, L cav ICA, large No No No Onyx20 + S/none 1 2 (H) No Yes No Yes 6, R sc ICA, small No No No Onyx20/none 1 1 (H) No Yes No Yes 7, R sc ICA, small No No No Onyx20/none 1 2 (H) No Yes No Yes 8, L cav ICA, large No No No Onyx20 + S/none 1 2 (M) No Yes No Yes 9, L sc ICA, small No No No Onyx20/none 1 1 (H) Asymptomatic Yes Yes Yes 10, L cav ICA, small No No No Onyx20/none 1 1 (NI) No Yes No No 11, L pcav ICA, giant Yes Yes Yes Onyx16/onyx20 + S 1 2 (M) No Yes Yes No 12, R cav ICA, giant Yes Yes Yes Onyx20 + S/none 1 2 (M) No Yes No Yes 13, L sc ICA, large No No No Onyx20 + S/none 1 0 (NA) Hemorrhage No NA No 14 Basilar tip, large No Yes Yes Onyx16/none 1 0 (NA) No No NA No R sup cb, small No No No Onyx16/none 1 0 (NA) No No NA No 15, L sc ICA, large No No No Onyx20 + S/none 1 2 (H) No Yes No Yes 16, R p ICA, small No No No Onyx20 + S/none 1 1 (H) No No NA No 17, L sc ICA, giant No No No Onyx16/none 1 1 (H) WS ischemia Yes No Yes 18, R cav ICA, giant Yes Yes No Onyx20 + S/none 1 0 (NA) WS ischemia No NA No 19, R cav ICA, giant No Yes No Onyx16/none 2 0 (NA) No Yes Yes No 20, R cav ICA, large No No No Onyx16/none 2 0 (NA) No Yes No No 21, R sup cb, giant Yes Yes Yes Onyx16/none 1 2 (M) Asymptomatic Yes Yes No 22, R sc ICA, giant Yes Yes Yes Onyx20/onyx20 + S 3 2 (M) No Yes Yes Yes 23 L sc ICA, giant No No No Onyx20/none 1 0 (NA) No Yes No No R cav ICA, small No No No Onyx20/none 1 0 (NA) No Yes No No R sc ICA, small No No No Onyx20/none 1 0 (NA) No Yes No No 24, R sc ICA, small No No No Onyx20/none 1 0 (NA) No No NA No 25, L cav ICA, large No No No Onyx20/none 1 0 (NA) No No NA No 26, R pcav ICA, large No No No Onyx20 + S/none 0 1 (M) No Yes No Yes 27, R cav ICA, giant No No Yes Onyx16/none 1 1 (M) Transient CCF Yes No No 28, R cav ICA, giant No No Yes Onyx20 + S/none 1 2 (M) Asymptomatic Yes No Yes 29, R cav ICA, giant No No Yes Onyx20 + S/none 0 1 (M) No Yes No No 30, R sc ICA, large No No No Onyx20/none 1 1 (H) Asymptomatic Yes No Yes 31, R cav ICA, small No No No Onyx20/none 0 1 (NI) No Yes No Yes 32, R sc ICA, giant No No No Onyx20 + S/none 1 2 (H) Asymptomatic Yes No Yes 33, R sc ICA, large No No No Onyx20/none 1 1 (H) Asymptomatic Yes No No 34, L sc ICA, large No No No Onyx20/none 1 1 (H) No Yes No Yes 35, L pc ICA, large No Yes No Onyx20/onyx20 + S 1 1 (M) No Yes Yes No 36, L sc ICA, large No No Yes Onyx20/none 1 0 (NA) No Yes No No 37, L sc ICA, small No No No Onyx20/none 0 2 (H) No Yes No Yes 38, L sc ICA, giant No Yes Yes Onyx20/none 1 2 (M) Asymptomatic Yes No Yes 39, L pc ICA, large No No No Onyx20/none 0 1 (M) No Yes No No 40, R sc ICA, giant No No No Onyx20/none 0 2 (M) No Yes No Yes 41, L sc ICA, giant No No Yes Onyx20/none 1 0 (NA) No Yes No No 42, R sc ICA, large No No Yes Onyx20/none 1 2 (H) No Yes No Yes * Patients 13 and 14 died after receiving the treatment relevant or irrelevant to the endovascular therapy. Aneurysms in the following patients contained previously placed GDCs: 14 (basilar tip aneurysm), 19, 21, 38. Abbreviations: cav indicates cavernous segment; p, petrous; pcav, petrocavernous segment; sc, supraclinoid; and sub cb, superior cerebellar artery.
† In patient 22, edema around the aneurysm increased after treatment.
‡ Onyx16 indicates 16% Onyx (16% EVOH, 84% DMSO); Onyx20, 20% Onyx (20% EVOH, 80% DMSO); and S, stent.
§ In the following patients, the aneurysm was not completely filled with the polymer, as shown on the posttreatment CT scans: 1, 11, 12, 16, 19, 21, 22, 27, 28, 30. That is, the polymer was not cast in the exact shape of the aneurysm.
‖ Data in parentheses are the MR appearances. H indicates hypointense; NA, not applicable because MR studies were not available; NI, not identified due to the small size; and M, mixed signal intensity.
¶ Lesions appearing after treatment. CCF indicates caroticocavernous fistula; WS, watershed.
# Follow-up angiography performed in the third month and/or at 1 year. (Simultaneous control examinations for sectional imaging were performed within 2 days.) No indicates that selective angiography had not been performed yet or that images were not available. That is, the treatment was recent and control imaging had not yet been performed or the patient had refused. Two patients died after treatment and did not undergo control angiography.
** Recanalization detected during selective control angiography.
†† In the following patients, MRAs showed that the parent artery had decreased in diameter: 1, 2, 5, 8, 12, 26, 28, 40. In the following patients, MRAs, showed that the parent artery had no apparent signal intensity: 15, 17, 32, 38. In the following patients, MRA results were comparable to those of selective angiography: 3, 6, 7, 9, 17, 22, 30, 31, 34, 37, 42.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Four dimensional-flow magnetic resonance imaging analysis of carotid-cavernous fistula, dural arteriovenous fistula and spinal arteriovenous fistula: Detecting shunt point and diagnosing based on flow dynamics analysis
- Imaging Artifacts of Liquid Embolic Agents on Conventional CT in an Experimental in Vitro Model
- Evaluation of a novel liquid embolic agent (precipitating hydrophobic injectable liquid (PHIL)) in an animal endovascular embolization model
- Intracranial 4D Flow MRI: Toward Individualized Assessment of Arteriovenous Malformation Hemodynamics and Treatment-Induced Changes