
Article Figures & Data
Figures
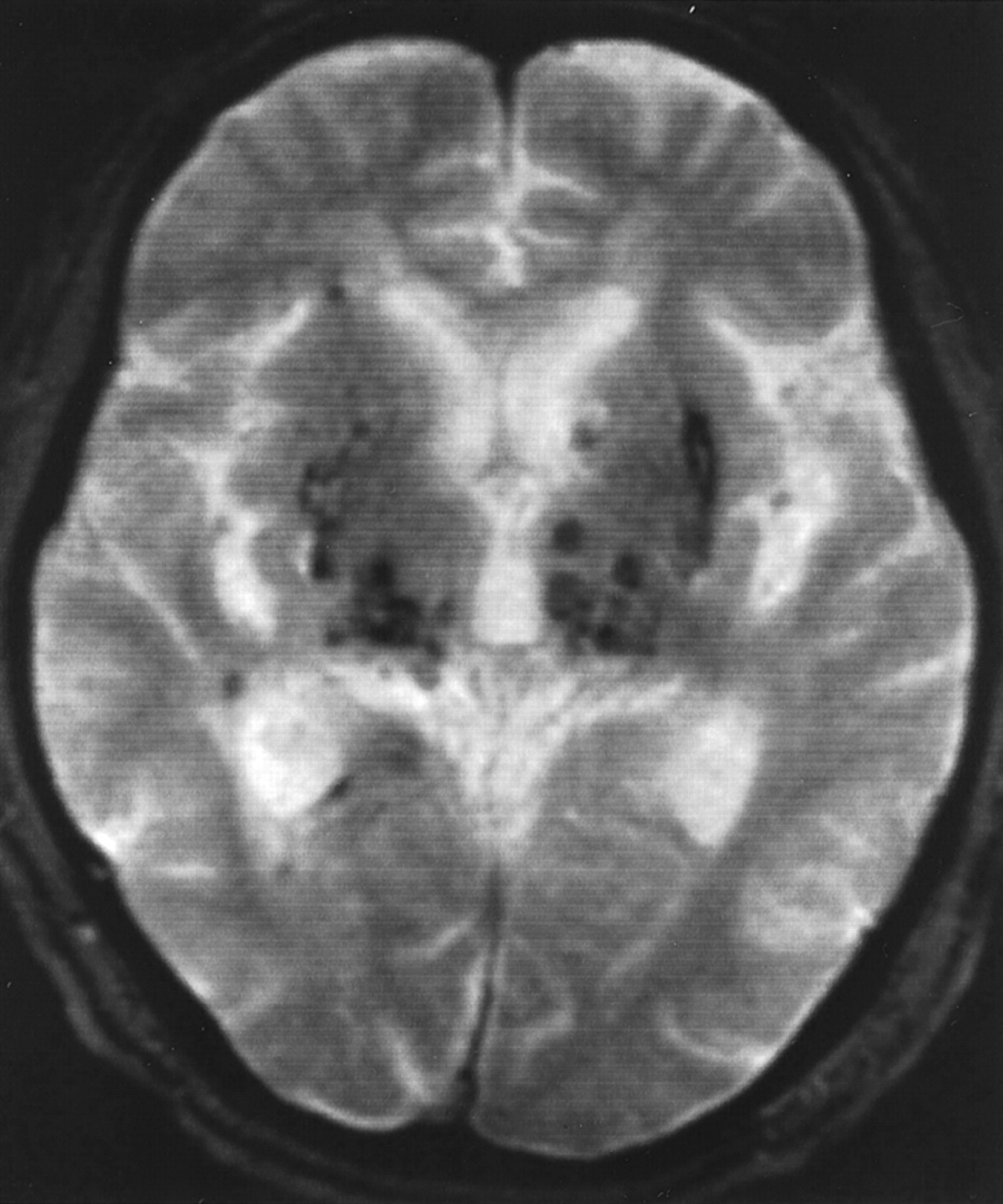
- Fig 1.
Multiple microhemorrhages were detected.
A and B, T2*-weighted gradient-echo images show microhemorrhages.
C and D, Lesions were less conspicuous on T2-weighted fast spin-echo images and were rarely shown on T1-weighted spin-echo images (not shown).
- Fig 2.
Graph shows age distribution (in years) of microhemorrhages. These lesions are usually observed in patients older than 40 years. The incidence of deep microhemorrhages increases with age, but that of lobar microhemorrhages seems to plateau in patients older than 60 years.
- Fig 3.
Graph shows correlation between the severity of white matter hyperintensity and the number of microhemorrhages (r = 0.71, P < .00001). Bars indicate SD.
- Fig 4.
T2*-weighted gradient-echo image of a 67-year-old hypertensive man who had hemorrhagic stroke at the left lentiform nucleus 2 years previously shows many deep microhemorrhages.
- Fig 5.
Graph shows incidence of microhemorrhages in patients with histories of deep and lobar hemorrhagic stroke. The incidence of lobar microhemorrhages is significantly higher in the patients with histories of lobar hemorrhagic stroke (P < .005).
- Fig 6.
Images of a 71-year-old man who had multiple lobar (cortical-subcortical) microhemorrhages.
A and B, T2*-weighted gradient-echo images show multiple lobar microhemorrhages (arrows).
C, New hemorrhagic stroke at the left parietal lobe can be seen 34 days after microhemorrhages were first observed on T2*-weighted gradient-echo images.
- Fig 7.
Images obtained in a 64-year-old woman who had multiple deep microhemorrhages.
A and B, T2*-weighted gradient-echo images show multiple deep microhemorrhages (arrows).
C, New hemorrhagic stroke at the right caudate head can be seen 402 days after microhemorrhages were first observed on T2*-weighted gradient-echo images.







Tables
- TABLE 1:
Demographic and Clinical Data Regarding the Patients With and Without Microhemorrhages
Variables Patients with Microhemorrhages (n = 197) Patients without Microhemorrhages (n = 1822) P Value Age (years) 67.2 ± 11.1 55.5 ± 15.9 <.00001 Sex, male 113 1028 .93 Hypertension 156 (79.1%) 545 (29.9%) <.00001 Diabetes mellitus 56 (28.4%) 289 (15.9%) .00002 Brain stroke history Hemorrhage 49 (24.9%) 20 (1.1%) <.00001 Infarction 67 (34.0%) 165 (9.1%) <.00001 White matter hyperintensity <.00001 Absent 41 (20.8%) 1387 (76.1%) Punctate foci 64 (32.5%) 289 (15.9%) Early confluent 70 (35.5%) 129 (7.1%) Confluent 22 (11.2%) 17 (0.9%) Location of Microhemorrhages No. of Patients No. of Lesions (range) Deep 161 0–40 Lentiform nucleus 96 0–19 Caudate nucleus 14 0–4 Internal capsule 4 0–3 Thalamus 88 0–14 Brain stem 54 0–8 Cerebellum 33 0–9 Lobar 93 0–40 Total 197 1–40 - TABLE 3:
Demographic and Clinical Data Regarding the Patients With and Without Histories of Symptomatic Brain Hemorrhage
Variable Patients with Hemorrhagic Stroke (n = 69) Patients without Hemorrhagic Stroke (n = 1950) P Value Age (years) 62.9 ± 10.1 56.4 ± 16.0 <.000001 Sex, male 48 (69.6%) 1093 (56.1%) .03 Hypertension 57 (82.6%) 644 (33.0%) <.000001 Diabetes mellitus 12 (17.4%) 333 (17.1%) 1.00 History of ischemic stroke 16 (23.2%) 216 (11.1%) .004 White matter hyperintensity <.000001 Absent 11 (15.9%) 1269 (65.1%) Punctate foci 33 (47.8%) 320 (16.4%) Early confluent 19 (27.5%) 180 (9.2%) Confluent 6 (8.7%) 33 (1.7%) Microhemorrhages 49 (71.0%) 148 (7.6%) <.000001 - TABLE 4:
Logistic Regression Analysis Shows That The Presence of Microhemorrhages Has the Highest Significant Correlation With History of Hemorrhagic Stroke
Variable Coefficient Standard P Value Exp (B) B Error Age (years) 0.021 0.01 .06 1.02 Sex, male 0.67 0.30 .02 1.95 Hypertension 1.32 0.37 .0004 3.74 History of ischemic stroke −0.43 0.34 .21 0.65 White matter hyperintensity 0.49 0.17 .005 1.63 Microhemorrhages 2.71 0.34 <.000001 15.03 - TABLE 5:
Demographic, Clinical, and MR Imaging Data Regarding the Patients With Histories of Hemorrhagic Stroke
Variable Hemorrhagic Stroke P Value Lobar (n = 11) Deep (n = 58) Age (years) 65.1 ± 10.1 (range, 42–76) 62.5 ± 10.1 (range, 38–84) .44 Sex, male 7 (63.6%) 41 (70.7%) .72 Hypertension 9 (81.8%) 48 (92.3%) .99 Diabetes mellitus 0 (0%) 12 (20.7%) .19 Periventricular hyperintensity .11 Absent 3 8 Punctate foci 6 27 Early confluent 0 19 Confluent 2 4 Microhemorrhages Lobar 7 (63.6%) 22 (37.9%) .005 Deep 5 (45.5%) 38 (65.5%) .31 Note.—Only the presence of microhemorrhages discriminates between cortical/subcortical and deep hemorrhagic strokes.
- TABLE 6:
Patients With Microhemorrhages, In Whom Hemorrhagic Strokes Were Prospectively Observed
Age (yr)/Sex Number of Microhemorrhages Hemorrhagic Stroke Associated Condition Lobar Deep Location Days* HT DM 71/M 6 0 Parietal lobar 34 − − 75/F† 2 0 Frontal lobar 147 + − 64/F‡ 2 8 Caudate head 402 + − 52/M 0 9 Thalamus 371 + + Note.—There may be a link between the site of hemorrhagic stroke and the distribution of microhemorrhages. HT indicates hypertension; DM, diabetes mellitus.
* Days indicates number of days after the microhemorrhages were first observed on T2*-weighted gradient-echo images.
† This patient had a history of parietal lobar hemorrhage. The other three patients had no previous brain stroke.
‡ This patient had a history of myocardial infarction, pulmonary artery thromboembolism, and deep venous thrombosis, for which she received warfarin.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Age-Related Differences in Human Cortical Microstructure Depend on the Distance to the Nearest Vein
- Remotely controlled drug release in deep brain regions of non-human primates
- Left Ventricular Mass, Brain Magnetic Resonance Imaging, and Cognitive Performance: Results From the Strong Heart Study
- Endothelial depletion of murine SRF/MRTF provokes intracerebral hemorrhagic stroke
- Association of Chronic Kidney Disease With Cerebral Microbleeds in Patients With Primary Intracerebral Hemorrhage
- Cerebral microbleeds and cognitive functioning in the PROSPER study
- Microbleeds Are Associated With Subsequent Hemorrhagic and Ischemic Stroke in Healthy Elderly Individuals
- Brain microbleeds as a potential risk factor for antiplatelet-related intracerebral haemorrhage: hospital-based, case-control study
- Brain Microbleeds and Global Cognitive Function in Adults Without Neurological Disorder
- Cerebral microbleeds in the population based AGES-Reykjavik study: prevalence and location
- Leukoaraiosis and intracerebral hemorrhage after thrombolysis in acute stroke
- Prevalence and severity of microbleeds in a memory clinic setting
- Microhemorrhages in a patient with reversible posterior leukoencephalopathy syndrome.
- Cerebral Microhemorrhages Predict New Disabling or Fatal Strokes in Patients With Acute Ischemic Stroke or Transient Ischemic Attack
- Cerebral Microhemorrhage
- Cerebral microbleeds on MRI: Prevalence, associations, and potential clinical implications
- Cerebral microbleeds are common in ischemic stroke but rare in TIA
- White matter lesions, cognition, and recurrent hemorrhage in lobar intracerebral hemorrhage
- A review of structural magnetic resonance neuroimaging
- Cerebral Microbleeds: Prevalence and Associations With Cardiovascular Risk Factors in the Framingham Study