
Abstract
BACKGROUND AND PURPOSE: Our hypothesis was that symptomatic and asymptomatic carotid plaques are different. The aim of this study was to identify the sonographic tissue and surface characteristics of plaques and their degree of stenosis that corresponded to these two clinical presentations.
METHODS: We studied 81 symptomatic and 111 asymptomatic plaques (150 patients) having 50% to 99% stenosis on duplex scanning. These plaques were imaged on duplex and captured in a computer. We evaluated the gray-scale median (GSM) to distinguish hypoechoic (low GSM) from hyperechoic (high GSM) plaques, and the bending energy (BE), to distinguish plaques with irregular (high BE) versus smooth (low BE) surfaces.
RESULTS: The symptomatic group corresponded to hypoechoic (median GSM, 4) and severely stenosed (median stenosis, 85%) plaques, whereas the asymptomatic group corresponded to hyperechoic (median GSM, 35) and moderately stenosed (median stenosis, 70%) plaques (P < .05 for both variables). The BE failed to separate the two groups; the mean BEs were 1.63 and 1.68 for the symptomatic and asymptomatic groups, respectively (P = .38).
CONCLUSION: Our results suggest that echogenic characteristics and the degree of stenosis are the strongest predictors of carotid plaque behavior. The sonographic surface characteristics failed to qualify as an index of plaque instability.
A longitudinal study of asymptomatic patients with carotid atheroma has shown that the hypoechoic and severely stenosed plaques are associated with a higher rate of an incident stroke (1). This observation stresses the importance of the echogenic characteristics and stenosis of the carotid atheroma in the pathogenesis of stroke.
In addition, a previous study has shown that hypoechoic and ulcerated carotid plaques on sonograms are associated with neurovascular symptoms, whereas hyperechoic and smooth-surfaced plaques are associated with an asymptomatic status (2). This study stresses the importance of sonographic ulcerations in the development of neurovascular symptoms. The plaque features, however, were visually evaluated and therefore not extremely accurate.
The aim of this cross-sectional study was to determine 1) computer-evaluated attributes of carotid plaques (in terms of sonographic tissue and surface characteristics) and 2) the degree of stenosis associated with the presence of neurovascular symptoms. It was hoped that the recognition of these features might elucidate the pathophysiological mechanisms involved.
Methods
We studied 192 carotid bifurcation plaques (from 95 men and 55 women; mean age, 70.32 years; range, 42 to 92 years), producing stenosis in the range of 50% to 99% at duplex scanning. These plaques were associated with no symptoms (n = 111, 57.8%), amaurosis fugax (n = 27, 14.1%), hemispheric transient ischemic attack (n = 35, 18.2%), or stroke (n = 19, 9.9%) on the retinal or hemispheric side ipsilateral to the plaque. Each plaque with its ipsilateral retinal or hemispheric side was treated as an independent case (unit of the study) and defined the side of interest on each patient. In all, 108 patients had unilateral carotid atheromas and 42 had bilateral carotid atheromas that could be analyzed.
Patients were recruited during duplex scanning in our vascular laboratory, and we relied upon referrals from medical, neurologic, and vascular surgical clinics. The reason for referral was to investigate the carotid arteries because of either a neurovascular symptom (symptomatic patients) or a carotid bruit with no symptoms (asymptomatic patients). The sonographic tissue and surface characteristics and stenosis of the carotid plaques were evaluated on presentation; duplex scanning is part of the routine investigation of patients with carotid atheromas in our hospital.
Symptoms were assigned by a neurologist who was unaware of the previous clinical reports and duplex findings, in accordance with the recommendations of the Committee for the Classification of Cerebrovascular Disease III (3). Appropriate to the concept of a cross-sectional investigation, we noted neurovascular symptoms only within the last 6 months on the side of interest (>50% stenosis). Patients with symptoms on the appropriate side more than 6 months before recruitment were excluded. This exclusion criterion was based on the fact that a plaque may change in terms of stenosis, surface, and echogenicity characteristics over time. In the present study, the intention was to “incriminate” the plaque under investigation in the development of symptoms.
Asymptomatic patients were considered those who had never had symptoms on the side of interest. Symptoms on the sides with <50% stenosis and in the vertebrobasilar system were not analyzed. The rationale for the exclusion of plaques producing <50% stenosis was based on the fact that it is more probable for a symptom caused by a carotid atheroma to be ascribed to a stenosis >50%, as suggested by the North American Symptomatic Carotid Endarterectomy Trial collaborators (4).
Patients with cardioembolic conditions such as atrial fibrillation, aortic or mitral valve abnormalities, recent (<6 weeks before the neurovascular event) myocardial infarction, or prosthetic cardiac valves and heart failure were excluded by a cardiologist on clinical and electrocardiographic grounds (3). Additional exclusion criteria included lacunar symptoms (pure motor hemiparesis, pure sensory stroke, motor-sensory stroke, ataxic hemiparesis, dysarthria clumsy-hand syndrome, and absence of cortical dysfunction) and cerebral hemorrhage, diagnosed by a neurologist on clinical and brain CT grounds (3), because lacunae and cerebral hemorrhages are not attributable to carotid atheroma.
These criteria (>50% carotid stenosis and exclusion of cardioembolism, lacunar symptoms, and cerebral hemorrhage) ensured the implication of carotid atheroma as the most likely cause in the pathogenesis of the neurovascular symptoms. The patients (n = 150) were selected from a total of 811 consecutive patients whose carotid stenosis was evaluated in our laboratory from July 1998 to December 1998.
Sonographic Evaluation: Grading of Internal Carotid Artery Stenosis
The severity of carotid stenosis was assessed at duplex scanning upon recruitment, using an ATL HDI 3000 scanner (Advanced Technology Laboratories, Bothell, Washington, USA). This entailed a hemodynamic evaluation of the index stenotic vessel based on standard criteria (Table 1) (5–12). The evaluation was performed by one experienced operator (T.J.T.) who was unaware of the clinical profile of the patients at the time of scanning and was fully familiar with the protocol of the grading of carotid stenosis.
Grading of carotid stenosis
Sonographic Tissue Characteristics of Carotid Plaques
Method
The carotid plaques were scanned on the ATL HDI 3000 scanner with a 7-MHz linear probe in the longitudinal, anterolateral projection at a minimal depth, then their b-mode static images were captured (capturing device: SCREEN MACHINE II version 1.1, Fast Multimedia AG, Munich, Germany) and digitized in a computer (Dell Dimension XPS P90, Berkshire, UK), keeping standard settings (13). The scanner settings were: medium frame rate, time gain compensation vertical to the blood vessel, linear postprocessing curve, minimal persistence, and maximum dynamic range (in this material, 60 dB). For the scanning settings, the gain, magnification, and angle of projection were adjusted so that in the captured image, the blood was dark, the adventitia was horizontal and bright, and the atherosclerotic plaque was well delineated. The source settings, display settings, effect settings, color settings, and capturing resolution (736 × 560 pixels) of the grabber were fixed for image capturing.
The overall brightness of the areas under study in the digital images was evaluated by computer software (Adobe Photoshop, Adobe Systems Inc., version 3, San Jose, CA) by means of the gray-scale median (GSM). This represents the median of the frequency distribution of tones of pixels included in these areas (13). After digitization, all images were normalized with linear scaling by the software, so that the GSM of blood was 0–5 tones, and that of the adventitia, 180–200 (13). By altering the images, we counteracted the effect of the different degrees of sonographic gain on plaque echogenicity, as has been shown (14). After normalization, the overall brightness of the plaques was evaluated by means of GSM.
Plaques included in an acoustic shadow were considered echoically analyzable by echo if more than 50% of their area offered real acoustic information, and only this section was subjected to analysis (the number of pixels in the analyzable area was at least half of the overall number of pixels in the plaque image as calculated by the software) (14).
In the case of poor visualization of the luminal edge, especially in hypoechoic (dark) plaques, we studied color images in parallel to the b-mode (gray scale) images to assist in delineation of the luminal margin. Color images were frozen on the screen, and an automatic switch-off of the color in the ATL HDI 3000 scanner provided the b-mode images on the same plane) (14).
These analyses were performed on presentation by the same experienced operator (T.J.T.) who evaluated the degree of stenosis.
Quantification of Visually Evaluated Echogenicity
The overall brightness of the plaques (n = 192) was evaluated by GSM and visually by one experienced operator (T.J.T.) at different times. The visual evaluation entailed a classification of the plaques into type 1 (hypoechoic, brightness equal to that of blood), type 2 (isoechoic, brightness equal to that of the periadventitia), or type 3 (hyperechoic, brightness greater than that of the periadventitia), as suggested by Polak et al (1). The median GSMs of the three groups (as they were classified visually into types) were compared to show the correspondence of the visual and digital evaluations of plaque echogenicity.
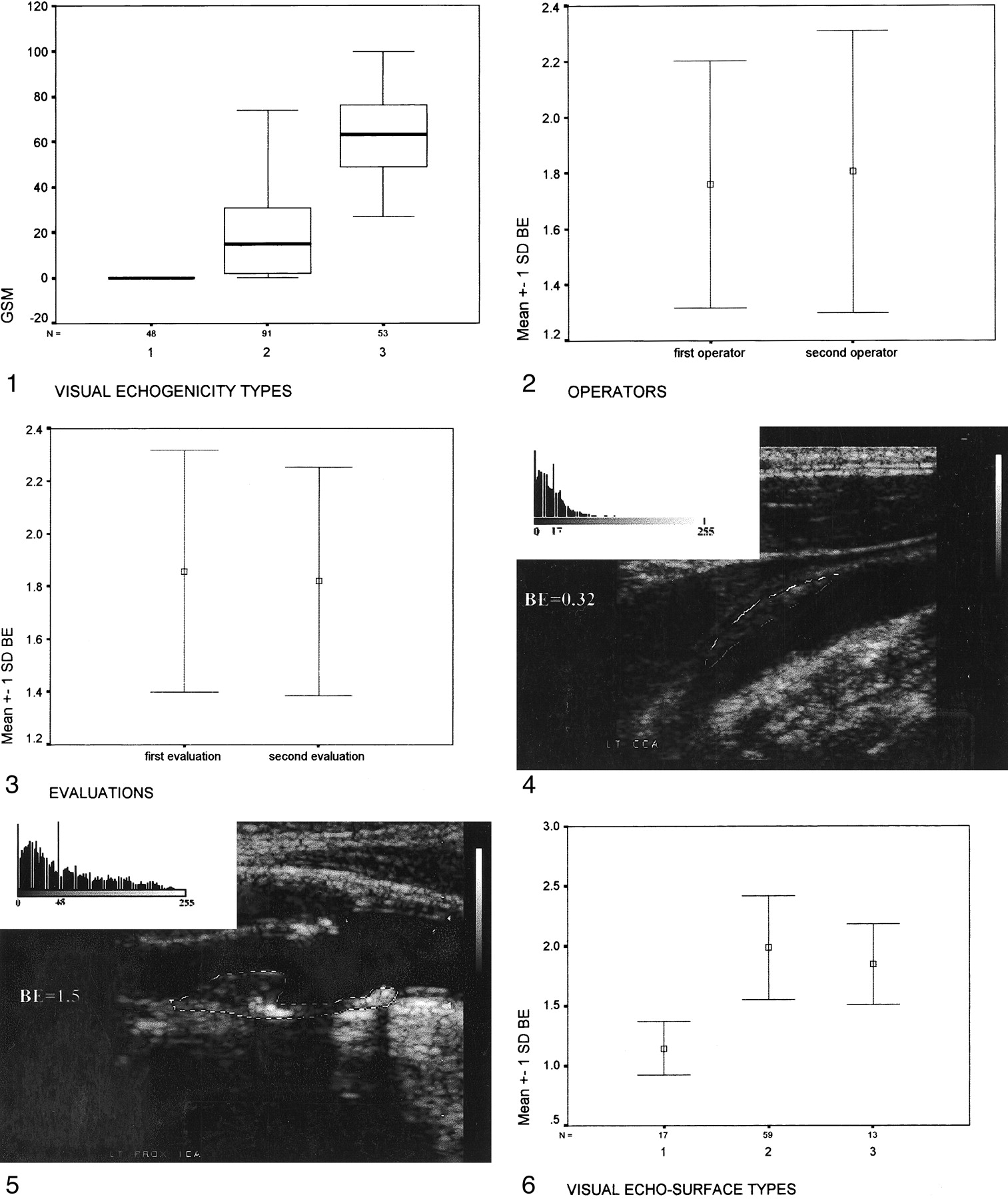
The comparison of the three visually evaluated echogenicity groups of plaque types by terms of GSM showed their separability (median GSM for type 1, 0; interquartile range, 0; median GSM for type 2, 15; interquartile range, 30; median GSM for type 3, 63; interquartile range, 30.5; Kruskal-Wallis test, P = .001 [Fig 1]). The use of medians, interquartile ranges, and nonparametric statistics was justified because the distribution of GSM was nonnormal (one-sample Kolmogorov-Smirnov test, P = .001).

Comparison of the three visually evaluated echogenicity groups of plaques (types 1, 2, and 3) in terms of GSM.fig 2. Interoperator reproducibility of the BE evaluation.fig 3. Intraoperator reproducibility of the BE evaluationfig 4. An intermediate hypoechoic (GSM, 17) and smooth (BE, 0.32) plaque.fig 5. An intermediate hyperechoic (GSM, 48) and intermediately irregularly surfaced (BE, 1.5) plaque.fig 6. Comparison of the three visually evaluated echo-surface groups of the plaques (types 1, 2, and 3) in terms of BE
Interoperator Reproducibility of Echogenecity by Visual Evaluation
The overall brightness of plaques (n = 192) was evaluated visually by two independent, experienced operators, and the interoperator reproducibility was calculated. The visual evaluation entailed a classification of the plaques into the three types described above (1). The results of the interoperator reproducibility were satisfactory (κ = .95; SE, .018; 95% confidence interval, .92–.99 [Table 2]).
Interoperator reproducibility, visual evaluation of plaque echogenicity
Sonographic Surface Characteristics of Carotid Plaques
Method
The sonographic surface characteristics of the digital plaque images were evaluated in the same computer by means of the bending energy (BE) and by the same experienced operator (T.J.T.) who evaluated the plaque echogenicity. The BE is a feature that measures the irregularity of a digital curve and can be perceived as the energy necessary to bend a rod to a desired shape (15). In this study, the BE described the irregularity of the luminal edge of the plaques (irregular or smooth) and was the output of computer software.
The evaluation of BE is based on a semiautomated method. Initially, the operator tracked the luminal edges of the plaques in the digital b-mode images by points and the program smoothed the resultant lines by interpolation. Then, the program identified the pixels corresponding to these lines and produced arrays of pixels. In the next step, the program produced arrays of numbers describing the relative position of every pixel to the following one, starting from the left side of the lines. For example, pairs of neighboring pixels being side by side corresponded to different numbers compared with those placed diagonally at 45° or 225°, one above the other or one below the other. These numbers described the rate of angulation of the lines under study and discriminated straight from curved lines. The end product was the evaluation of curvature vectors and finally of BEs.
The analysis was performed on b-mode images by using as a guide the color images for the identification of the luminal plaque edges. The color images were frozen on the screen, and an automatic switch-off of the color in the ATL HDI 3000 scanner provided the b-mode images on the same plane. These were the same images used for the evaluation of echogenicity.
Interoperator and Intraoperator Reproducibility of BE
The BE of 89 plaques was evaluated in a computer by two independent, experienced operators. The one-sample Kolmogorov-Smirnov test was performed on both distributions of BE and showed normality (first operator, P = .88; second operator, P = .39). This result dictated the use of a parametric test in the analysis of the BE.
The comparison of the two operators in terms of BE, taking into account the within-plaque variability, showed that these two groups were similar in terms of their BE means (mean ± SD 1.8 ± .5 for the first operator vs 1.76 ± .44 for the second; Fig 2). A univariate analysis of variance, with a fixed-effect model and two-way analysis yielded a P value of .68.
The BE of 21 plaques was evaluated in a computer by one experienced operator (T.J.T.) at two different times. The one-sample Kolmogorov-Smirnov test performed on both distributions of BE showed normality (first evaluation, P = .72; second evaluation, P = .88). This result dictated the use of a parametric test in the analysis of the BE.
Comparison of the two evaluations of BE, taking into account the within-plaque variability, showed that these two groups were similar in terms of their BE means (mean ± SD 1.85 ± .69 for the first evaluation and 1.82 ± .57 for the second; Fig 3). Univariate analysis of variance with a fixed effect model, two-way analysis, yielded a P value of .4.
Quantification of Visually Evaluated Surface Characteristics
The surface characteristics of the plaques (n = 89) were evaluated visually and by BE by one experienced operator (T.J.T.) at different time frames. The visual evaluation entailed classification of the plaques into type 1 (smooth surface), type 2 (intermediately irregular surface), or type 3 (completely irregular surface [Figs 4 and 5]). The means and standard deviations of the three groups (as they were classified visually into the three types) were compared to show the correspondence of the visual and digital evaluations of plaque echo-surface.
The comparison of the three visually evaluated echo-surface groups of plaque types by means of BE showed their separability (mean BE for type 1, 1.14 ± .22; for type 2, 1.98 ± .43; for type 3, 1.84 ± .33; one-way analysis of variance, P = .0001, [Fig 6]). The use of means, standard deviations, and parametric statistics was justified because the distribution of BE was normal (one-sample Kolmogorov-Smirnov test, P = .88).
Interoperator Reproducibility of Echo Surface by Visual Evaluation
The irregularity of the luminal surface of 89 plaques was evaluated visually by two independent, experienced operators, and the interoperator reproducibility was calculated. The visual evaluation again entailed a classification of the plaques into the three types. The interoperator reproducibility (Table 3) showed satisfactory results (κ = .72; SE, .075, 95% confidence interval, .57–.86).
Interoperator reproducibility, visual evaluation of plaque echo-surface characteristics
Statistical Analysis
The statistical package SPSS for Windows, release 9, was used for data analysis. The one-sample Kolmogorov-Smirnov test was used to evaluate the normality of the distributions (GSM, ipsilateral stenosis, and BE). The Mann-Whitney U test and the unpaired t test were performed to distinguish the plaques associated with symptomatic and asymptomatic sides, in terms of GSM, ipsilateral stenosis, and BE. Binary logistic regression was performed to assess the value of each variable (GSM, ipsilateral stenosis, and BE) in the prediction of symptomatic versus asymptomatic presentation. The accepted level of statistical significance was 5%.
Results
The distribution of the clinical status of the 192 sides of interest included 81 symptomatic sides (42.2%, the symptomatic group) and 111 asymptomatic sides (57.8%, the asymptomatic group).
The one-sample Kolmogorov-Smirnov test performed on the distribution of the GSM showed nonnormality (P = .001), dictating the use of a nonparametric test in its analysis. The median GSM in our population was 14.5 (range, 0–98). Comparison of the distributions of the GSM between the symptomatic and asymptomatic groups showed that these groups were distinct in terms of this variable (Mann-Whitney U test, P = .001). The median GSM (interquartile range) was 4 (23.5) for the symptomatic group and 35 (55) for the asymptomatic group.
The one-sample Kolmogorov-Smirnov test was performed on the distribution of the stenosis and also showed nonnormality (P = .0001), dictating the use of a nonparametric test in the analysis of the stenosis. The median stenosis overall was 80% (range, 50–99%). The distributions of the stenosis in the symptomatic and asymptomatic groups were distinct, with median values (interquartile ranges) of 85% (20%) and 70% (25%), respectively (Mann-Whitney U test, P = .001).
The one-sample Kolmogorov-Smirnov test performed on the distribution of the BE showed normality (P = .88), dictating the use of a parametric test in the analysis of BE. The mean BE in our population was 1.66 (range, .32–3.08). The distributions of the BE were similar between the two groups, with means (±SD) of 1.63 ± .38 for the symptomatic group and 1.68 ± .43 for the asymptomatic group (unpaired t test, P = .39).
Binary logistic regression (enter method) considering the GSM, ipsilateral stenosis, and BE as independent variables and the presence or absence of neurovascular symptoms as the dependent variable showed the strongest predictors of symptoms to be the GSM (P = .001; regression coefficient, .02; odds ratio, 1.03; 95% confidence interval, 1.01–1.04) and stenosis (P = .001; regression coefficient, −.03; odds ratio, .96; 95% confidence interval, .94–.98). The BE was not a predictor of neurovascular symptoms (P = .51; regression coefficient, .25; odds ratio, 1.28; 95% confidence interval, .6–2.74).
The GSM and stenosis were slightly related in an inverse linear fashion (Pearson's correlation, P = .001, r = -.24), whereas these features were linearly unrelated to the BE (Pearson's correlation for the GSM-BE correlation, P = .26; r = .08; for the stenosis-BE correlation, P = .8; r = .01).
Discussion
Previous studies have shown that dark sonographic tissue characteristics (hypoechogenicity), severe stenosis, and the presence of an “sonographic” ulcer indicate an unstable (symptomatic) carotid plaque (1, 2, 16). The present study was conducted in attempt to identify the strongest determinants of plaque instability. In the current study, the GSM and the degree of carotid stenosis were the discriminators between the symptomatic and asymptomatic groups. The BE failed to qualify as a discriminator.
The current study showed excellent interoperator reproducibility of the visually evaluated plaque echogenic patterns, according to the three-type classification system proposed by Polak et al (1) (κ value of agreement, .95). It also showed the adequacy of the GSM to assess these patterns quantitatively.
Arnold et al (17), using a four-type classification system for echogenicity (Gray-Weale; type 1, hypoechoic plaques, to type 4, hyperechoic plaques), showed κ values of .53 for the intraoperator reproducibility and .52 for the interoperator reproducibility in an off-line image analysis (18). One possible reason for the low κ values is that the reproducibility studies were performed on nonstandardized (nonnormalized) images. In an on-line image analysis, Mathiesen et al showed a κ value of .56 for the interoperator reproducibility of plaque echogenicity using the Gray-Weale classification (19). In this study, there was no provision for the sonographic gain standardization and the angle of interrogation of plaques. Geroulakos et al (20) showed a κ value for interoperator reproducibility of .79 in an off-line analysis of plaque echogenicity, using a five-type classification system and strict scan settings. Possibly, the photographic paper they used for image storage, with the compression it produces, contributed to this result. Joakimsen et al (21), in an off-line analysis using the Gray-Weale classification and following strict criteria for the sonographic settings, gain standardization, and two echoanatomic reference points (blood and adventitia) for evaluation of plaque echogenicity, showed a κ value of .73 for interoperator reproducibility and .69 for intraoperator reproducibility. The present study showed a κ value of .95 for interoperator reproducibility. One possible explanation is the use of a three-type classification system for plaque echogenicity (as opposed to the four- or five-type classification systems) and the normalization of images that makes them more correctly classifiable by the human eye.
Regarding the evaluation of echogenic characteristics of plaques by means of GSM, the present study was based on a published method (13) that showed a satisfactory interoperator reproducibility, and its implementation of this method reduced variability in carotid plaque echogenicity when four different sonographic gains and two different scanners were used (14).
Aly and Bishop (22) used the mean of the gray scale to assess the plaque echogenicity. In the present study, the GSM was preferred because the distributions of the gray tones of the pixels in most plaque images were nonnormal. Another study used the integrated backscatter, the frequency dependence of backscatter, the integrated attenuation, and the slope of attenuation (23).
Our study also showed satisfactory interoperator reproducibility of the visually evaluated plaque echo-surface patterns. We noted satisfactory intra- and interoperator reproducibility in the evaluation of BE and adequacy of this feature to assess plaque echo-surface patterns quantitatively.
Many studies have addressed the significance of carotid plaque echogenicity in the development of neurovascular symptoms. On the basis of the Gray-Weale classification (17), various cross-sectional investigations have shown that the relative frequency of neurovascular symptoms is higher in patients with type 1 or 2 carotid plaques, whereas the frequency of asymptomatic status is higher in patients with type 3 or 4 plaques (20, 24, 25). This pattern was negated in one study, probably because of the absence of sonographic gain standardization (26).
In the pursuit of higher accuracy, El-Barghouty et al (27) used the GSM (a feature of an echo-analysis computer program) as an index of overall plaque brightness. In one cross-sectional study, they showed that carotid plaques with a low GSM (hypoechoic) were associated with a higher relative frequency of neurovascular symptoms than that of plaques with a high GSM (hyperechoic). Pedro et al (28) reached the same conclusion.
This association between the dark sonographic tissue characteristics and neurovascular symptoms has been verified in prospective, natural history studies of asymptomatic patients with carotid plaques that have used as an endpoint the development of neurovascular events. Hypoechoic plaques were symptom-prone compared with hyperechoic ones (1, 29, 30). The findings in all the above studies are in agreement with our results.
Several follow-up studies have addressed the significance of stenosis in the development of subsequent stroke. The greater the carotid stenosis, the higher the incidence of stroke, in both symptomatic and asymptomatic cohorts (1, 4, 30–32). Again, all of their findings agree with our results.
As for the significance of the carotid plaque ulceration, a series of pathologic studies has shown that this feature is associated with the development of neurovascular symptoms, possibly through embolism (33–38). A previous study, however, contradicts this position (39).
Other studies have shown that angiographically defined ulceration of carotid plaque was associated with the development of neurovascular symptoms (35, 40) or middle cerebral artery occlusion (41). In addition, a few angiographic studies have shown that “deep” ulcers (type B) or complicated, cavernous ulcers (type C) are associated with a higher incidence of neurovascular symptoms compared with “shallow” ulcers (type A) (42, 43). This angiographic classification of ulcers based on their size was proposed by Moore et al (42). Other studies have disagreed with these findings, however (44, 45).
Regarding the “sonographic” ulcer, one study showed it to be associated with the presence of neurovascular symptoms and plaque smoothness to be associated with asymptomatic status (46). Other sonographic studies have shown that it is the deep ulcer and not the surface irregularity of plaques that is associated with the presence of symptoms (2, 47). In addition, a similar study showed that irregularly surfaced plaques on sonograms were more likely to be associated with territorial brain CT infarctions than were the smooth plaques (48). The present study failed to discriminate the symptomatic and asymptomatic groups based on the digitally evaluated, sonographic surface irregularity of plaques.
The ability of angiography to identify carotid plaque ulcers verified at pathologic examination varies from poor (49, 50) to satisfactory (35, 51). In addition, sonography has proved to be poor in identifying ulcers detected at pathologic examination (52–56). This might be why our study failed to discriminate the symptomatic and asymptomatic groups on the basis of BE.
In two studies, sonography was superior to angiography in the detection of ulcerated carotid plaques identified by pathologic examination (57, 58), whereas neither method was satisfactory in another study (59).
Our study has shown that the carotid plaque GSM and stenosis are slightly related in an inverse, linear fashion. The findings of a previous study supports this result (25).
The current study showed no correlation between the carotid plaque GSM and BE. Other studies, however, have shown that hypoechoic plaques were associated with “pathologic” ulcers (17) or “sonographic” ulcers (60).
Although we noted no correlation between carotid stenosis and BE, other studies have reported that increasing degrees of carotid stenosis are associated with a high prevalence of “sonographic” ulcers (61) or “pathologic” ulcers (62). One study that evaluated the ulcers sonographically, however, found no such relationship (63), and another found that increasing degrees of carotid stenosis were not associated with angiographically verified ulcers (64).
We noted an association between carotid plaque hypoechogenicity and the development of neurovascular symptoms. In some previous studies, carotid plaque hypoechogenicity has been directly associated with the size of lipid core and inversely associated with the fibrous tissue and calcification as evaluated at pathologic examination (65–67), but not in all (68). Similarly, hemorrhage has (13) and has not (56) been associated with carotid plaque hypoechogenicity. In addition, decreased contrast of the sonographic images of carotid plaque (an index of hypoechogenicity) was found to be associated with soft material (lipids and hemorrhage) (69).
Gronholdt et al (66) hypothesized that the increased size of the lipid core (a determinant of the carotid plaque hypoechogenicity) predisposes to plaque rupture, embolism, and the development of neurovascular symptoms. Indeed, one study has reported a relationship between carotid plaque hypoechogenicity and high embolic count detected in the ipsilateral middle cerebral artery at transcranial Doppler (70).
Our study showed that severe carotid stenosis is associated with the development of neurovascular symptoms but failed to distinguish symptomatic from asymptomatic carotid plaques on the basis of the sonographic surface characteristics. This might reflect the inability of sonography to depict “real” ulcers.
Conclusion
In this study, the echogenic characteristics and degree of stenosis were the strongest predictors of carotid plaque behavior. Sonographic surface characteristics failed to qualify as an index of plaque activity.
It might be interesting to apply these methods—carotid plaque echogenicity and degree of stenosis to prospective natural-history studies of asymptomatic patients with carotid plaques, with the end point of stroke development attributable to carotid atheroma (71). Such studies might identify groups of patients at different risk for stroke. The result will be better refinement of the criteria for carotid endarterectomy, which will offer benefits both to vascular specialists and to patients.
Footnotes
1 Address reprint requests to Dr. T. J. Tegos, Neurology Department, Hammersmith Hospital, 150 Du Cane Road, London W12 0HS, UK.
References
- Received September 15, 2000.
- Accepted after revision March 24, 2001.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- An Ultrasonographic Multiparametric Carotid Plaque Risk Index Associated with Cerebrovascular Symptomatology: A Study Comparing Color Doppler Imaging and Contrast-Enhanced Ultrasonography
- Inter-Rater Reliability of Carotid Atherosclerotic Plaque Quantification by 3-Dimensional Sonography
- Chronologic Echogenicity Changes and Histologic Correlates in Experimental Blood Clots: A Serial Sonographic Study
- Histological Assessment of 526 Symptomatic Carotid Plaques in Relation to the Nature and Timing of Ischemic Symptoms: The Oxford Plaque Study
- Elastin and Calcium Rather Than Collagen or Lipid Content Are Associated With Echogenicity of Human Carotid Plaques
- Relative Value of Normalized Sonographic In Vitro Analysis of Arteriosclerotic Plaques of Internal Carotid Artery
- Quantification of the Wall Inhomogeneity in B-mode Sonographic Images of the Carotid Artery