
Abstract
Summary: An MR arteriogram obtained in a patient with migraine headaches during prodrome showed features of carotid dissection. A repeated study conducted within minutes demonstrated complete patency. Vascular spasm was proposed to be the cause. Migraine occurs in more than 10% of the population. The possibility of misdiagnosing a vascular spasm as carotid dissection is real and should be guarded against since there are great prognostic and treatment implications.
The MR arteriogram of a patient with migraine headaches is reported here. The case demonstrated obstruction of the left carotid artery that was spontaneously released. The obstruction was due to carotid spasm. The MR arteriogram greatly simulated carotid dissection.
Case Report
A 37-year-old woman had unilateral headache attacks for many years, treated with Panadol on demand. She was not taking any pills and did not smoke. The attacks were as frequent as once per week. They typically lasted hours and were associated with nausea followed by vomiting, which usually relieved the headache. The headache was described as throbbing and was moderate in severity. There was no association with photophobia, phonophobia, or neurologic deficit. The patient experienced a spasm over the neck region before some of the attacks. The symptoms fell within the International Headache Society criteria (1) for migraine without aura.
During one weekend, the woman had a severe migraine heralded by intense malaise and followed by a fainting spell. She recovered without any neurologic deficit and there was no actual trauma to the head during the faint.
She was imaged 4 days later with a 1.5-T unit (Siemens Vision, Erlangen, Germany). While in the head coil, she felt a spasm over her left neck. The T1-weighted, proton density–weighted, and T2-weighted images were all normal, showing no noteworthy white matter changes. MR arteriography was done with a multiple overlapping-slabs time-of-flight technique with cranial tracking saturation pulse. There was no lateral presaturation pulse applied in our protocol. This showed decreased flow in the left internal carotid artery siphon (Fig 1A) as well as the left anterior and middle cerebral artery (Fig 1B). The findings pointed to an occlusive disease of the carotid artery, including embolus, stenosis, and carotid dissection. The known association of dissection with migraine made the diagnosis of carotid dissection quite suspicious. Since most carotid dissection occurs in the neck, a head-neck coil was exchanged within minutes. MRA of the neck vessels was performed from the aortic arch upward to overlap the previously imaged segment with decreased flow. However, this showed complete patency of the carotid, including the siphon (Fig 2A and B). When the patient came out of the imager, she showed no neurologic deficit. Typical headache followed but the patient was able to go back to her normal work.

Images from first session with a head coil show suspicion of carotid dissection.
A, Source image shows little flow in the left internal carotid artery as compared with the right side.
B, Maximum intensity projection image shows decrease in flow in the left internal carotid, the left middle cerebral, and anterior cerebral arteries.

Images from first session with a head-neck coil show return of flow in the left internal carotid artery within minutes.
A, Source image shows equal flow in the right and left carotid siphons.
B, Maximum intensity projection image shows complete patency of the carotid arteries including the siphons.
The patient was imaged again after 2 days with MR arteriography from the upper neck to the intracranial region. There was complete patency of all four arteries (Fig 3). The circle of Willis was complete. The patient had a smaller left vertebral artery all along, believed to be a normal variant. However, diffusion-weighted imaging with an apparent diffusion coefficient (ADC) map showed restriction in diffusion over the posterior territory of left middle cerebral artery (Fig 4). This was speculated to be caused by a recent ischemic event. It could not be a complicated migraine with infarction since there was no actual neurologic symptom and the plain MR images were normal on both occasions. Another possible explanation was spreading depression of Leao. Spreading depression causes changes in extracellular and intracellular ion concentrations with corresponding electrochemical gradient changes, depolarization of neurons and glial cells, cell swelling, and shrinkage of the interstitial space (2). Spreading depression as the cause of many neurologic ictus, including epilepsy, transient amnesia, migraine, and even stroke-in-evolution, is controversial. It is associated with the visual aura of classical migraine and may be the primary prerequisite for the vasoconstriction and vasodilatation implicated for migraine. These spreading waves of intermittent depolarization may cause signal abnormality in patients examined days after the onset of attack (3). Our patient's diffusion-weighted imaging was done two days after the event, and spreading depression offers a good explanation. Since there was no visual aura in our patient, ischemia due to the spasm remained the likely possibility. The increase in signal intensity in the diffusion-weighted image and decreased ADC, regardless of whether they were due to ischemia or spreading depression, were caused by reduced diffusion of interstitial water, owing to a relative decrease of the interstitial space.

Images from 2 days after first session on a head coil shows equal flow in the right and left anterior and middle cerebral arteries

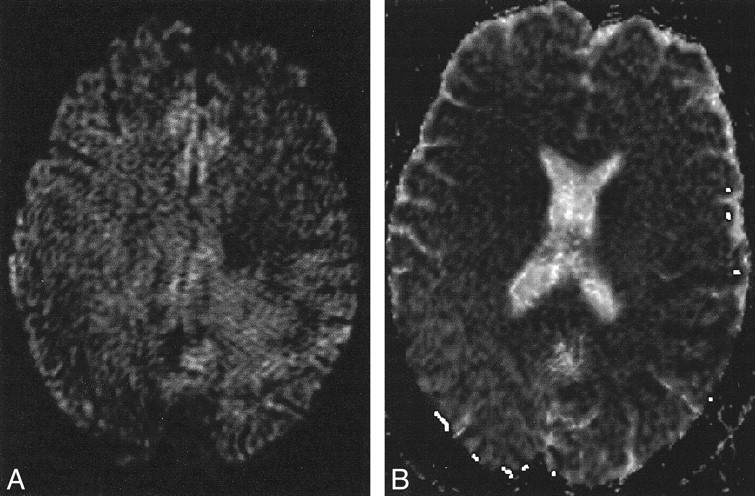
Diffusion-weighted image with ADC map shows restricted diffusion on left middle cerebral artery territory.
A, Diffusion-weighted image with b = 1000 T shows increased intensity over the left middle cerebral artery territory.
B, The ADC map shows decreased diffusion over middle cerebral artery territory as low signal intensity.
Blood investigation in the week showed normal spot sugar, complete blood picture, and normal renal and liver function, except for a slightly raised erythrocyte sedimentation rate of 18 mm (normal < 15 mm) and total protein of 81 mmol/L (normal < 80 mmol/L).
Discussion
The usual central nervous system abnormalities in migraine include a unilateral or bilateral increase in hyperintense spots on T2-weighted images (4), but these are quite common even in normal populations and may have an ischemic basis. Edema (5) has been described in the acute phase, and atrophy (6) in the chronic phase. At phosphorus spectroscopy (7), a defect of brain mitochondrial respiration may be reviewed as interictal low PCr concentration with or without an increase in Pi content.
Vascular spasm and dilatation have long been implicated as the cause of the prodrome and headache in migraine, respectively (8). This case conforms to this theory. In fact, similar cases have been demonstrated with catheter angiograms, but direct catheterization may cause spasm on its own. Cerebral blood flow abnormalities were also demonstrated in other studies (9).
Complicated migraine with cerebral infarction is well known (10). Carotid dissection has been shown to be more common in patients with migraine headaches (9) and is also more common in young and middle-aged women. Carotid artery dissection could easily be misdiagnosed in this case on the first MR arteriogram, with great prognostic and therapeutic implications; the patient might inadvertently undergo anticoagulation.
Because of the high prevalence of migraine in the general population (11), cases with MR arteriographic features similar to that of dissection could easily happen. Since most carotid dissections and spasms occur in the neck region, the neck carotid arteries should be imaged once a decreased flow is detected in the head region. The source images and plain MR images should be scrutinized carefully for the crescent of hematoma (12) to diagnose a dissection. In addition, the authors would propose to reimage any patient with migraine headaches if vascular obstruction is shown on images obtained during an attack. Reimaging should be done after the prodrome so as to guard against misdiagnosing a spasm as dissection.
Footnotes
1 Grant support provided by the Tung Wah Group of Hospitals, Hong Kong.
2 Address reprint requests to P.P. Iu, Department of Radiology, Kwong Wah Hospital, 25 Waterloo Road, Kowloon, Hong Kong.
References
- Received February 22, 2001.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}