
Abstract
Summary: We report the MR findings of parapharyngeal branchial cleft cyst manifesting as multiple, lower cranial nerve palsies in a 35-year-old woman. On MR images, a well-marginated cystic mass was detected in the right parapharyngeal space, with displacement of both the right internal carotid artery and the right internal jugular vein on the posterolateral side. The cyst contained a whitish fluid that was slightly hyperintense on T1-weighted images and slightly hypointense to CSF on T2-weighted images. No enhancement on contrast-enhanced T1-weighted images was present. The right side of the tongue showed high signal intensity on T2-weighted images, suggesting denervation.
Branchial cleft cysts are the most common neck masses in adults. Most are second branchial cleft cysts, which occur in the neck, anterior to the sternocleidomastoid muscle at the mandibular angle. Rarely these cysts may be present in the parapharyngeal space. We describe a case of parapharyngeal branchial cleft cyst manifesting as multiple lower cranial nerve palsies, an unusual location and presentation for this lesion.
Case Report
A 35-year-old woman initially presented with a 1-month history of hoarseness. On physical examination, the gag reflex was decreased, the uvula was deviated to the left, and a right vocal cord palsy and right-sided paresis of the tongue were noted and attributed to palsies of cranial nerves IX, X, and XII. There was no palpable abnormality of the neck, and the patient was afebrile.
MR scanning revealed a large, thin-walled cyst in the right parapharyngeal space, the content of which was slightly hyperintense on T1-weighted images and slightly hypointense to CSF on T2-weighted images (Fig 1A and B). There was no enhancement of the lesion on contrast-enhanced T1-weighted images (Fig 1C). The cyst displaced both the right internal carotid artery and the right internal jugular vein on the posterolateral side. The cyst occupied the right parapharyngeal space from below the skull base to the hyoid bone level on coronal images (Fig 1D). The right side of the tongue showed high signal intensity on short inversion time inversion-recovery (STIR) images (Fig 1E), consistent with denervation. There were no abnormal lymph nodes in either neck area.

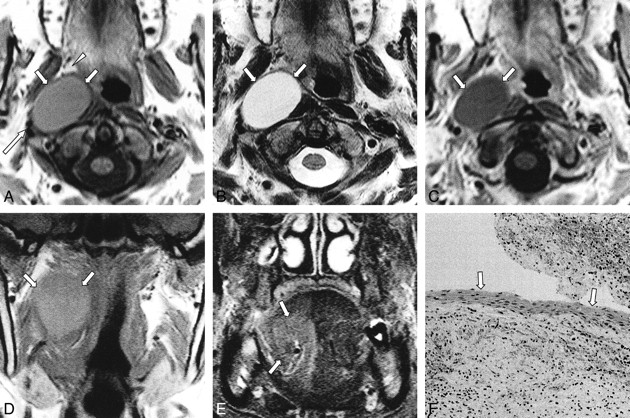
A 35-year-old woman with hoarseness.
A, T1-weighted (627/15 [TR/TE]) axial MR image shows well-marginated mass (arrows) slightly hyperintense to the CSF in the right parapharyngeal space. The mass displaces parapharyngeal fat anteriorly (arrowhead) and compresses the lateral portion of the longus colli muscle. The mass also displaces both the right internal carotid artery and the right internal jugular vein to its posterolateral side (long arrow).
B, T2-weighted (3800/99) axial MR image shows the mass (arrows) is slightly hypointense to the CSF.
C, Contrast-enhanced T1-weighted (627/15) axial MR image reveals no definite enhancement of the mass (arrows).
D, T1-weighted (530/12) coronal MR image shows the mass (arrows) occupies the right parapharyngeal space from below the skull base to the hyoid bone level.
E, The STIR (6500/150/60 [TR/TI/TE]) coronal image shows the right side of the tongue has high signal intensity (arrows), suggesting denervation.
F, Photomicrograph (hematoxylin-eosin, original magnification ×100) of the lesion shows a squamous epithelial-lined cyst wall (arrows), consistent with a branchial cleft cyst.
Excision of the neck mass was performed via a transcervical approach. A 5-cm × 4-cm, well-circumscribed, whitish ovoid mass was identified in the right parapharyngeal space. The mass was cystic and contained thick whitish pus. The adjacent cranial nerves IX, X, and XII were compressed by the mass, but were grossly normal in size and color. Histopathologic evaluation of the mass revealed a squamous epithelial-lined cyst with lymphoid infiltrate, consistent with a branchial cleft cyst (Fig 1F). The mass was identified as an infected second branchial cleft cyst. Gradual recovery of the multiple cranial nerve palsies occurred within 3 weeks.
Discussion
Second branchial cleft remnants account for the majority of branchial cleft abnormalities. Embryologically, the second arch overgrows the second, third, and fourth branchial clefts. This process results in expansion of the second branchial cleft into an elongated common cavity, called the cervical sinus of His, which is obliterated shortly after its formation. Various degrees of incomplete closure of the sinus lead to anomalies of the second branchial cleft. Anomalies can occur anywhere along an embryologically defined tract that extends from the external opening, the anterior border of the junction of the middle and lower thirds of the sternocleidomastoid muscle, passes between the internal and external carotid arteries superficial to cranial nerves IX and XII, and enters the oropharyngeal tonsillar fossa (1, 2). The parapharyngeal space is a very rare location for a branchial cleft cyst. This rare location superior to the tonsillar fossa can best be explained by the fact that a second branchial cleft cyst can have an associated tract that passes to the palatine tonsil. Because this tract passes through the caudal paraphyrngeal space, cysts that occur in this location are usually classified as second cleft anomalies (3). Although two previous reports stated that his type of parapharyngeal cyst was thought to be a first branchial cleft anomaly (4, 5), the site of pharyngeal attachment and lack of deformity of derivatives of the first branchial apparatus support the view that such cysts originate in the second branchial apparatus, as in our study (6).
Symptoms referable to masses within the parapharyngeal space are often minimal; the most common is a bulge in the overlying pharynx (2). Palsy of cranial nerves IX, X, XI, or XII is extremely rare in benign tumors or cysts, and usually suggests direct infiltration of local malignancies or metastatic lymph nodes (7). In our patient, the paralysis of lower cranial nerves IX (decreased gag reflex), X (uvula deviation and hoarseness secondary to vocal cord palsy), and XII (tongue deviation) can be related to mechanical compression of nerves as a result of marked enlargement of the cyst attributable to superimposed infection (8). At surgery, the cranial nerves showed grossly normal morphologic characteristics and color, although they were compressed by the mass. The cranial nerve palsies subsided in a relatively short period probably because the nerves manifested a transitory dysfunction owing to mechanical compression. There have been few reports on cranial nerve palsies associated with branchial cleft cysts (2, 8)
The reported MR findings of branchial cleft cysts do not differ from those of other cysts; ie, a well-marginated, homogeneous, cystic mass. The signal intensity is isointense to the CSF on T1- and T2-weighted images (3, 6). If the cyst is infected, a thin rim of enhancement is possible. Although this was not observed in our case, the margin of the cyst could also be poorly circumscribed because the adjacent fat planes may be obscured, and the signal intensity of the cystic content may be increased on T1-weighted images because of the increased protein content of the cystic fluid (2). An important goal of imaging is to differentiate primary parapharyngeal space lesions from more common, deep-lobe parotid lesions that have infiltrated the space in order to determine the appropriate surgical approach (9). MR imaging can accomplish this by revealing the fat plane between the normal parotid gland and a mass arising within the parapharyngeal space.
The differential diagnosis of a parapharyngeal mass includes cystic schwannomas and minor salivary gland tumors. Although large schwannomas can undergo cystic degeneration, complete cystic change preserving an even, thin wall is very rare, and good enhancement of the solid portion is seen in most cases. Furthermore, anteromedial displacement of the internal carotid artery is frequently present with schwannomas in this region and is highly suggestive of an origin within the carotid space (10). Minor salivary gland tumors, such as pleomorphic adenomas originating within the prestyloid parapharyngeal space, can be distinguished from a branchial cleft cyst because they usually show heterogeneous, intermediate signal intensity on T1-weighted images and intermediate-to-high signal intensity on T2-weighted images, even though they also posteriorly displace the internal carotid artery (9, 10). Furthermore, complete cystic change is very rare in minor salivary gland tumors.
Complete surgical excision is the treatment of choice for preventing recurrence (11), although percutaneous ethanol sclerotherapy could also be used (12). The transcervical approach provides the most complete exposure (11).
In conclusion, the differential diagnosis of a cystic lesion within the parapharyngeal space should include an atypical second branchial cleft cyst. A rapidly growing, infected branchial cleft cyst can present with lower cranial nerve palsies.
Footnotes
1 Address reprint requests to Ho Kyu Lee, M.D., Department of Radiology, Asan Medical Center, 388-1 Poongnap-Dong, Songpa-Ku, Seoul 138-736, South Korea.
- Received August 2, 2000.
- Copyright © American Society of Neuroradiology
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.