
Article Figures & Data
Figures
- fig 1.
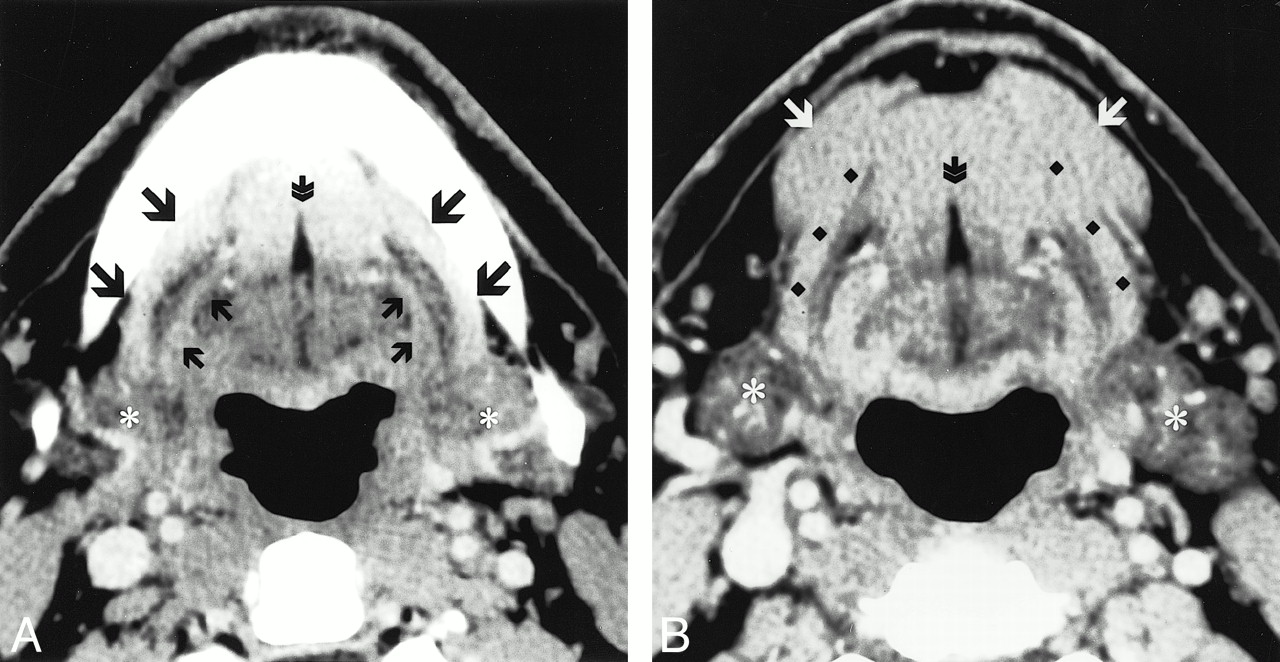
Normal postcontrast axial CT images through the oral cavity. B is caudal to image A. The classic anatomy of the mylohyoid muscle (A, large black arrows: B, black diamonds) is seen forming a continuous muscular barrier separating the deep sublingual space from the superficial SMS. Running parallel to the posterior aspect of the mylohyoid muscle is the hyoglossus muscle (small black arrows). On either side of the fibro-fatty lingual septum (double arrow) are the genioglossus muscles cranially, and the geniohyoid muscles caudally. Caudally, the anterior belly of the diagastric muscle (white arrows) blends with the superficial margin of the mylohyoid muscle. Asterisks signify the submandibular glands (18)
- fig 2.
Postcontrast axial CT images through the oral cavity showing multiple mylohyoid muscle defects. Image A is cranial to image B. On the patients left side, there are two mylohyoid muscle defects. On the right, there is one defect. Accessory salivary tissue is identified bilaterally (large arrows). Note that the accessory salivary tissue has the same attenuation as that of the normal submandibular glands (*).A, large arrow, accessory salivary tissue; small arrows, fat-containing defects. B, large arrows, accessory salivary tissue; small arrow, fat-containing defect (18).
- fig 3.
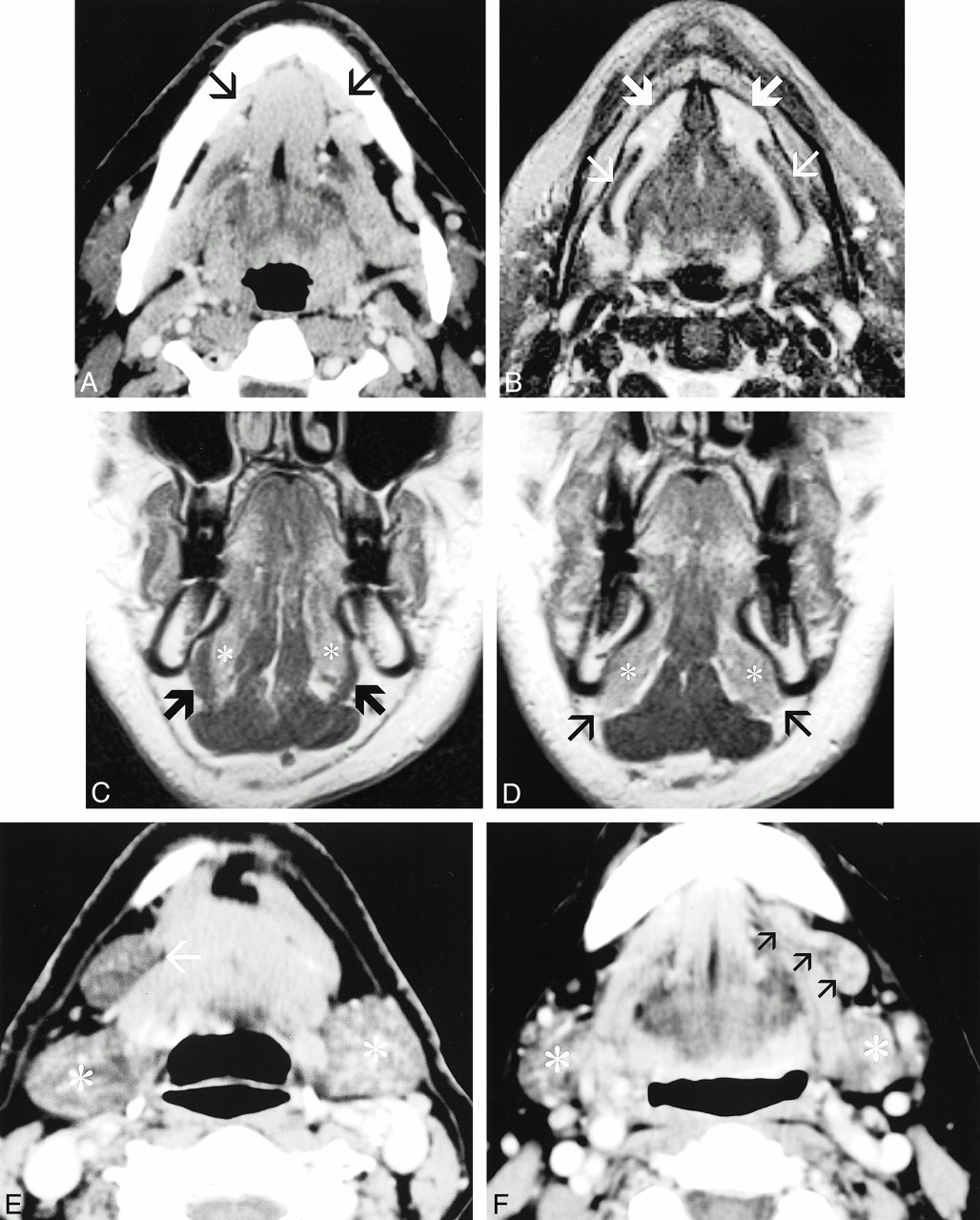
Accessory salivary tissue has a variable appearance and location in the oral cavity. General features include tissue that is associated with mylohyoid defects and is of similar attenuation and appearance as orthotopic salivary tissue.
A–D, CT and MR correlation in the same patient with anterior accessory salivary tissue. A, Postcontrast axial CT scan. B, Axial fast spin-echo fat-saturated T2-weighted image. C and D, Postcontrast coronal T1-weighted image. Image C is posterior to image D. The postcontrast CT scan shows enhancing tissue that extends into the submandibular space through deficiencies in the anterior mylohyoid muscle bilaterally (small black arrows). The deficient mylohyoid muscle is clearly identified on the fat-saturated T2-weighted sequence (small white arrows). The normal hyperintense sublingual salivary tissue is clearly identified, extending into the submandibular space anteriorly (large white arrows). The coronal sequences are very useful for identifying the mylohyoid muscle. C depicts the intact mylohyoid muscle (large black arrows) separating the sublingual space and sublingual salivary tissue (*) from the submandibular space. D is located more anteriorly at the level of the mylohyoid defects. Notice the absence of the mylohyoid muscle at this level allows extension of the sublingual salivary tissue into the submandibular space (small black arrows).
E, Postcontrast CT shows a large deposit of salivary tissue that is located predominately in the submandibular space, with a tapering configuration toward a mid-mylohyoid defect (single arrow). The attenuation and appearance is very similar to the normal submandibular glands (*).
fig. 3 (Continued)
F, Postcontrast CT shows accessory salivary tissue, which spans a defect in the mid aspect of the mylohyoid muscle. The tissue is well defined, elongated in configuration, and located in both the sublingual and submandibular space. The attenuation and appearance is very similar to that of the normal submandibular gland (*) (18).
- fig 4.
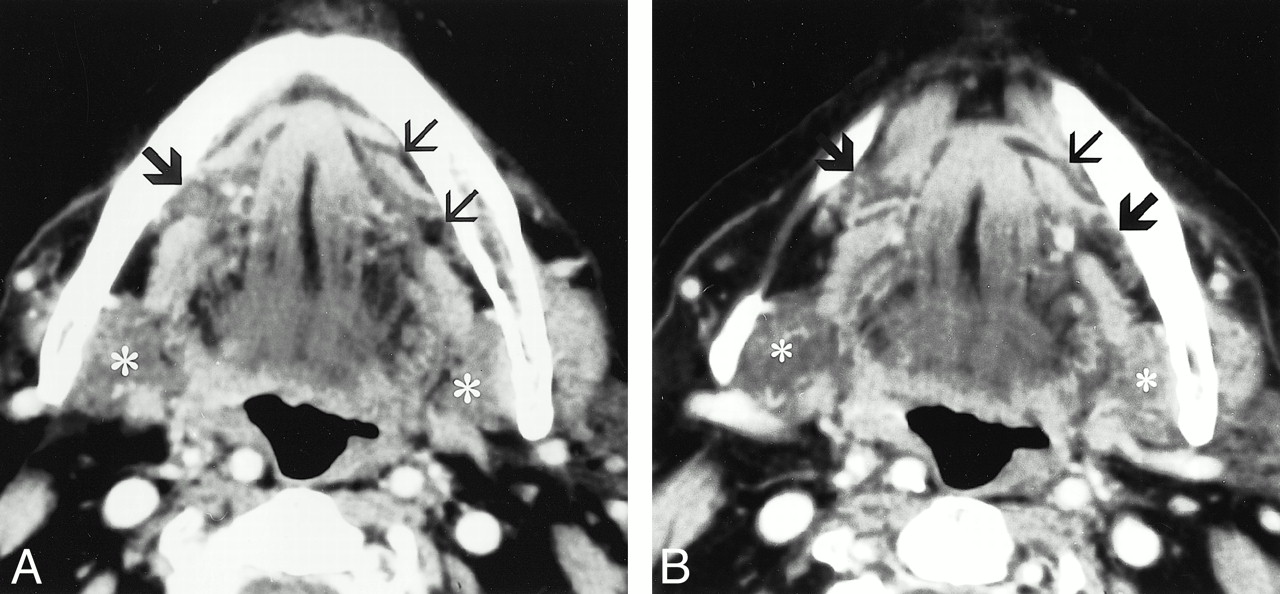
The most common contents of mylohyoid defects are fat, followed by blood vessels. Fat-containing defects are seen as discrete areas of discontinuity in the mylohyoid muscle, containing low-density adipose tissue. Blood vessels may be identified passing through discrete mylohyoid defects or may be seen perforating the mylohyoid muscle, without an identifiable defect.
A and B, Postcontrast CT images in different patients. A, On the patient's right side, there is a discrete, wedge-shaped defect in the mid-to-anterior aspect of the mylohyoid muscle (small arrow). On the patient's left side, there is a blood vessel perforating the mylohoid muscle, without an associated defect (large arrow). B, On the patient's left side, there is a large defect in the anterior half of the mylohyoid muscle, containing both fat and a large blood vessel (arrow).
C and D, CT and coronal CT reformation correlation in the same patient. C is a postcontrast axial CT scan, and D is a coronal, reformatted CT image. These images show a discrete, fat-containing defect in the mid mylohyoid muscle (large arrow). On the coronal image, the small arrow on the patient's left side identifies the intact mylohyoid muscle for comparison (18).
- fig 5.
This line drawing illustrates the superficial anatomy of the submandibular space with mylohyoid defects containing accessory salivary tissue and perforating submental branches of the facial artery and vein.
Large arrow, Accessory salivary tissue; small arrow, mylohyoid defects; large arrowhead, submental branch of facial vein; small arrowhead, submental branch of facial artery; D, anterior belly of diagastric muscle; M, mylohyoid muscle; FA, facial artery off the external carotid artery; FV, facial vein; A, common carotid artery; V, internal jugular vein (18).





Tables

One hundred individuals scanned
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Types of Sublingual Gland Herniation Observed During Sonography of Plunging Ranulas
- CT and MR findings of bilateral submandibular gland aplasia associated with hypertrophied symmetrical sublingual glands herniated through mylohyoid defects
- Imaging the oral cavity: key concepts for the radiologist
- Bilateral submandibular gland aplasia with clinico-radiological mass due to prolapsing sublingual salivary tissue through mylohyoid boutonniere: a case report and review
- Mylohyoid herniation of the sublingual gland diagnosed by magnetic resonance imaging
- Giant Ranula of the Neck: Differentiation from Cystic Hygroma