
Abstract
BACKGROUND AND PURPOSE: Percutaneous transluminal angioplasty (PTA) for significant stenosis involving the origin of the vertebral artery is now a well established treatment for selected patients when posterior cerebral arterial circulation is compromised. Arterial spasm, dissection, and restenosis may occur in some instances, with subsequent hemodynamic compromise. To prevent these potential complications, we combined PTA of the vertebral artery with primary stenting, using coronary stents, in seven patients. We herein present our short- and intermediate-term results.
METHODS: A total of seven lesions affecting the origin of the vertebral artery were treated by primary trans-stenotic coronary stent placement. All patients were symptomatic, fulfilling the general criteria for vertebral artery angioplasty. Patients were followed for up to 36 months after treatment.
RESULTS: All seven lesions were successfully dilated. Residual stenosis was never greater than 20% in diameter. No perioperative complications occurred. Clinical follow-up showed immediate resolution or improvement of symptoms in all patients. One patient's condition deteriorated 15 months after stent placement because of atheromatous stenosis of the prevertebral segment in the ipsilateral subclavian artery.
CONCLUSION: Stent placement to treat significant stenosis involving the origin of the vertebral artery is safe and effective for alleviating symptoms and improving blood flow to the posterior cerebral circulation. Coronary stent design seems to be particularly well suited to cover atherosclerotic lesions of the origin of the vertebral artery. The stent mesh probably prevents elastic recoil and early restenosis after PTA, as it does in coronary arteries.
Obstructive lesions of the vertebral arteries may cause symptoms of vertebrobasilar insufficiency. Although these are often ignored, symptomatic atherosclerotic stenosis involving this circulation will often respond to percutaneous transluminal angioplasty (PTA). There has been some reluctance in the endovascular community to be aggressive with these lesions, partly because of concerns regarding early or late restenosis of atherosclerotic lesions. Technical complications include arterial spasm and intimal dissection with potential subsequent hemodynamic compromise in the posterior circulation. There are, however, real potential benefits to the patient in terms of symptom resolution. We report our initial results and follow-up of proximal vertebral angioplasty and stenting for the treatment of symptomatic atherosclerotic stenoses.
Methods
Seven patients (six male and one female patient; mean age, 68 years) underwent vertebral angioplasty and stenting using balloon-expandable coronary stents (Figs 1 and 2). All lesions were located at the origin of the vertebral artery (three right, four left).

Patient 1.
A, Angiogram of the left subclavian artery shows subocclusive stenosis of the left vertebral artery ostium (arrow).
B, Plain radiograph shows the Palmaz-Schatz stent (arrow) after its delivery. Considering plaque calcifications (arrowheads) as the boundary of the left subclavian artery, the stent is slightly protruding into the subclavian artery lumen.
C, Final control angiogram of the left subclavian artery shows excellent antegrade filling of the left vertebral artery. The prevertebral segment of the subclavian artery is severely diseased (filled arrow). The distal segment of the subclavian artery is chronically occluded. A scapular artery facilitates the arterial circulation of the patient's left arm (open arrow). The patient was doing well at the 3-year follow-up visit.

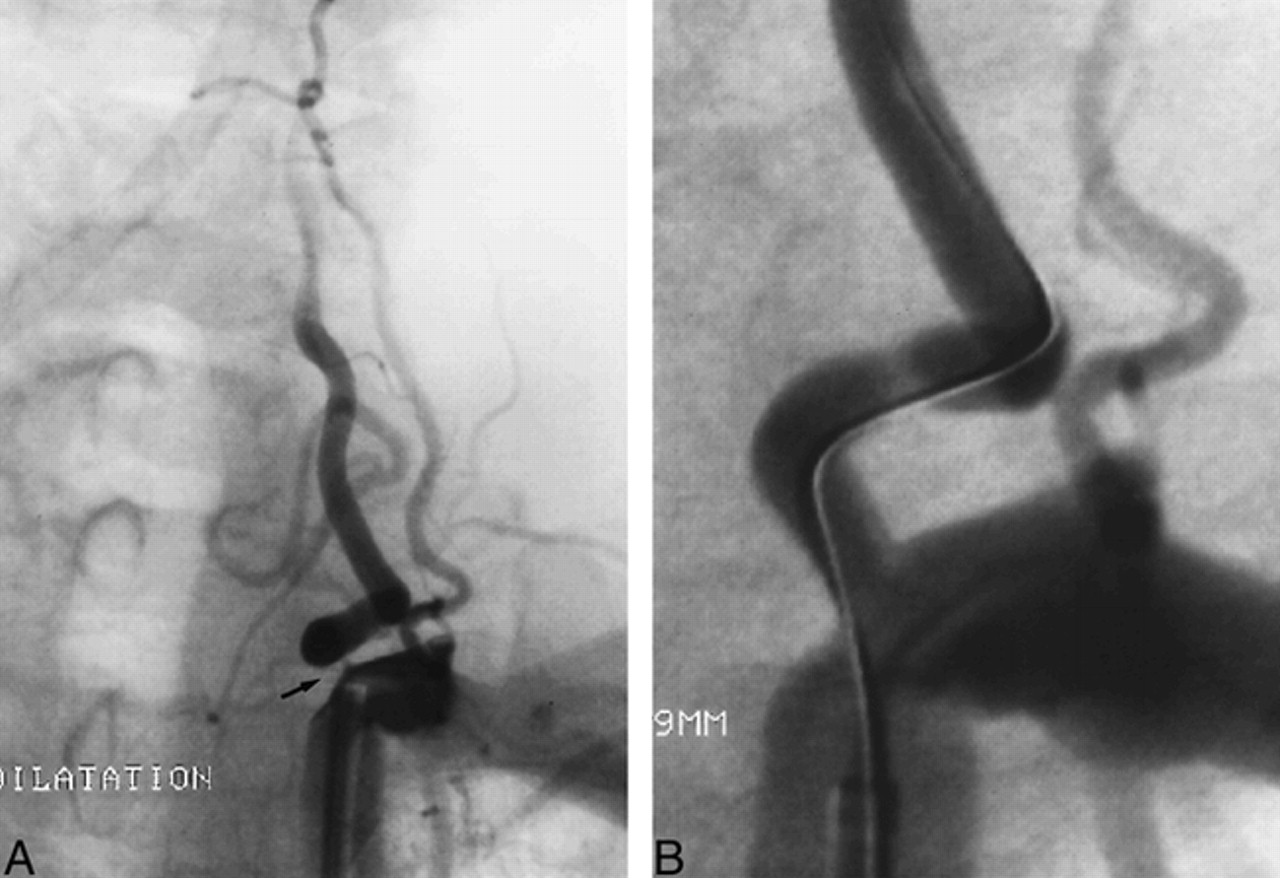
Patient 6.
A, High-grade stenosis of the origin of the left vertebral artery (arrow).
B, Post stenting angiogram (NIR Primo stent) of the left subclavian artery shows excellent antegrade filling of the left vertebral artery. The patient was doing well at the 18-month follow-up visit.
Clinical Evaluation and Indication for PTA
Our population had a wide variety of symptoms of posterior fossa and posterior cerebral ischemia. Symptoms were refractory to medical therapy, including antiplatelet and anticoagulant medication, in all patients. The Table summarizes the patients' clinical data.
Clinical data, cross-sectional imaging and angiographic results
Radiologic Evaluation
CT or MR imaging of the brain was performed before digital subtraction angiography. One patient underwent an hexametazime single-photon emission CT brain study. This showed cerebellar hypoperfusion. Aortic arch angiography and four-vessel digital subtraction angiography were performed to evaluate extra- and intracranial arteries in all patients. Special attention was paid to the subclavian and vertebral arteries and to the collateral blood flow to posterior cerebral circulation. Vertebral artery stenosis was considered to be angiographically significant when greater than 70%, but only if the other vertebral artery was equally diseased or absent. The angiographic appearance of the atherosclerotic vertebral lesions in this series was uniform, showing smooth luminal stenosis without plaque ulceration at the origin of the vessel. There was no evidence of distal vertebral or basilar artery stenosis in any patient.
PTA and Stent Implantation
In all except one case, therapeutic procedures were performed during a second angiographic session. In six cases, the endovascular approach was performed via a transfemoral route with the patients under local anesthesia. In one case, a brachial approach was preferred because proximal vessel tortuosity made access too difficult via a transfemoral route.
After arterial puncture, a 7F sheath was inserted and systemic anticoagulation was achieved with IV administered heparin (5000 IU) and aspirin (250 mg). A 7F guiding catheter was then navigated into the subclavian artery, and an “angiographic roadmap” was made of the subclavian and the vertebral arteries. The narrowed arterial segment was then crossed with a 160-cm-long 0.014-inch guidewire (Transend 14; Scimed, Maplegrove, MA) that was navigated into the normal distal cervical vertebral artery. The PTA balloon catheter, with the crimped stent, was then placed over the guidewire and directed across the lesion site. The balloon was inflated up to the maximum recommended pressure to deploy and impact the stent into the inner arterial wall. Balloon inflation never lasted longer than 20 to 30 seconds.
The vertebral arteries in our patients had diameters of 3 to 5 mm, which is a caliber similar to that of coronary arteries. In the first two cases, we used Palmaz-Schatz (Johnson and Johnson, Warren, NJ) and NIR (Boston Scientific Corporation, Natick, MA) coronary stents that were manually crimped on a 5-mm-diameter coronary balloon catheter (Viva, Boston Scientific Corporation). In the five remaining cases, we used premounted NIR stents (NIR PRIMO; Boston Scientific Corporation). These allowed for easy navigation across the stenotic arterial segment and immediate, rapid, and accurate stent placement without the use of balloon predilation.
Post-PTA Medical Regimen and Follow-up
Immediately after stent placement, digital subtraction angiography was performed to assess the treated vessel. Careful attention was also paid to the intracranial circulation to rule out any sign of distal embolization. Patients were discharged from the neurologic ward 2 to 7 days (mean, 4 days) after the procedure, when their neurologic condition was determined to be stable. They received 500 mg of ticlopidine daily (Ticlid; Sanofi Winthrop, Gentilly, France) for at least 3 months after PTA. The follow-up duration ranged from 4 to 36 months (mean, 15 months) after stent implantation. Duplex Doppler sonography was used during the follow-up period to assess stent patency.
Results
The seven patients presented with acute (two cases) or chronic (five cases) vertebrobasilar insufficiency attributable to severe stenoses at the origin of the dominant vertebral artery, with contralateral vertebral artery flow impairment from vertebral hypoplasia, stenosis, or occlusion. The symptoms resolved in all patients after endovascular treatment. In no case was the residual stenosis greater than 20% nor were there signs of distal embolization on the immediate control angiograms. No transient or permanent neurologic deficits occurred.
Only one patient had a recurrence of his referring symptoms (patient 3). Duplex Doppler follow-up in this case disclosed stenosis of the left subclavian artery. Digital subtraction angiography confirmed the presence of an atheromatous stenosis of the prevertebral segment of the ipsilateral subclavian artery without any restenosis of the stented origin of the vertebral artery. The six other patients, who did well, had no sonographic evidence of restenosis.
Discussion
Patient Selection for Vertebral PTA
Symptomatic posterior circulation atheromatous lesions are now treatable by an endovascular approach (1). PTA of the vertebral artery may be indicated when vertebral arterial flow–obstructing lesions are found in patients with brain stem ischemia (2). Our patients presented with symptoms suggesting vertebrobasilar insufficiency, such as vestibular ataxia, vegetative disturbance (presyncopal episode), nausea, gait disturbance, and drop attacks (Table). The combination of symptoms made the diagnosis of posterior fossa ischemia almost pathognomonic. Medical therapy (anticoagulation) failed to resolve the symptoms, and endovascular revascularization (PTA and stenting) was prompted. The majority of patients with symptoms of posterior cerebral circulation ischemia, however, can be managed by conservative treatment, including anticoagulation and antiplatelet medication (3). Most patients tolerate occlusion of one vertebral artery because there is usually sufficient blood perfusion from the contralateral side. For patients presenting with bilateral vertebral stenosis who are refractory to medical treatment, PTA is a viable alternative to surgery. The goals are to improve blood flow to the posterior cerebral circulation and to reduce the risk of distal embolization (4).
Exhaustive angiography of both the posterior and anterior cerebral circulations is required before performing angioplasty. Special attention must be paid to collateral supply from the contralateral vertebral artery, as well as the external carotid artery, from which collaterals may restitute the distal vertebral artery in cases of vertebral occlusion or severe stenosis. Also, patients may have excellent filling of the posterior circulation via the posterior communicating arteries and may tolerate stenosis of one or both vertebral arteries. Considering these possibilities for collateral blood flow, it is not surprising that lesions in the vertebrobasilar system are often asymptomatic and that only the minority of patients will benefit from treatment.
PTA and Stenting of the Proximal Vertebral Artery
There have been reports of the use of PTA to treat proximal vertebral artery stenosis (1, 5–10). PTA is now a well established therapeutic alternative to operative reconstruction of proximal vertebral artery stenoses and seems to be relatively safe. No mortality has been reported after PTA. Spasm, immediate occlusion secondary to dissection, and long-term restenosis may occur after PTA. These may be asymptomatic or may lead to transient or permanent neurologic complications. Higashida et al (1) reported that 8.8% of their patients had transient neurologic complications after PTA of the proximal vertebral artery. In this series of 34 patients who underwent angioplasty without stenting, the restenosis rate was 8.8% (three patients, two of whom were symptomatic). The cases of restenoses were successfully treated with repeat balloon angioplasty. Bruckman et al (5) reported a restenosis rate of 15% after proximal vertebral artery PTA, again without stenting. Storey et al (11) implanted stents in the proximal vertebral artery in two patients to treat symptomatic restenosis. This resulted in immediate reversal of stenosis and resolution of symptoms in both patients (11). Angiographic follow-up at 1 year showed continued patency of vertebral artery lumina. Feldman et al (12) reported the case of a patient presenting with bilateral proximal vertebral artery stenoses. These lesions were treated with Palmaz-Schatz coronary stents immediately after balloon angioplasty alone failed to achieve a good anatomic result (12).
Repeat angioplasty with stent placement may be a solution to treat immediate or delayed restenosis, but primary stent placement, as it was performed in our series, may obviate the need for repeat angioplasty. Distal embolization in the cerebral circulation is always a major concern when treating diseased vessels of the cerebral circulation. Stent placement may lower the potential for embolism by smoothing luminal irregularities, decreasing turbulence, and increasing flow. Furthermore, fibrous tissue and neointimal growth over the stent mesh has been shown to cover atheromatous tissue in experimental models, thereby lowering the risk for thrombus formation and further distal embolization (13). Also, significantly lower incidence of restenosis has been shown in coronary arteries of patients after the placement of stents greater than 3 mm in diameter (14). Patients in our series underwent stent placement in vessels of 3 to 5 mm in diameter, which is a caliber similar to that of coronary arteries. Coronary stent flexibility allowed for ease of tracking along vessel tortuosity, especially when a brachial approach was used.
Conclusion
Restenosis after angioplasty without stenting is a cause of midterm failure of vertebral angioplasty in atherosclerotic disease. Primary reinforcement of the vessel wall with a stent may improve the immediate and long-term outcomes of proximal vertebral artery PTA. Premounted coronary-designed stent systems are ideal for symptomatic atheromatous stenoses in the vertebral arterial circulation. They allow for one-step angioplasty and stent placement, avoiding the need of primary balloon dilation.
Footnotes
↵1 Address reprint requests to Michel Piotin, MD, 4 rue Euryale Dehaynin, 75019 Paris, France.
References
- Received March 23, 1999.
- Copyright © American Society of Neuroradiology
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Lesion location, stability, and pretreatment management: factors affecting outcomes of endovascular treatment for vertebrobasilar atherosclerosis
- A Systematic Review of Stenting and Angioplasty of Symptomatic Extracranial Vertebral Artery Stenosis
- Doppler Criteria for Identifying Proximal Vertebral Artery Stenosis of 50% or More
- Long-Term Outcome After Angioplasty and Stenting for Symptomatic Vertebral Artery Stenosis Compared With Medical Treatment in the Carotid And Vertebral Artery Transluminal Angioplasty Study (CAVATAS): A Randomized Trial
- Guidelines for Prevention of Stroke in Patients With Ischemic Stroke or Transient Ischemic Attack: A Statement for Healthcare Professionals From the American Heart Association/American Stroke Association Council on Stroke: Co-Sponsored by the Council on Cardiovascular Radiology and Intervention: The American Academy of Neurology affirms the value of this guideline.
- Guidelines for Prevention of Stroke in Patients With Ischemic Stroke or Transient Ischemic Attack: A Statement for Healthcare Professionals From the American Heart Association/American Stroke Association Council on Stroke: Co-Sponsored by the Council on Cardiovascular Radiology and Intervention: The American Academy of Neurology affirms the value of this guideline.
- Vertebral artery origin angioplasty and primary stenting: safety and restenosis rates in a prospective series