
Abstract
BACKGROUND AND PURPOSE: Atherosclerosis of the major intracranial arteries is an important cause of ischemic stroke. We established measurement criteria to assess percent stenosis of a major intracranial artery (carotid, middle cerebral, vertebral, basilar) and determined the interobserver/intraobserver agreements and interclass/intraclass correlations of these measurements.
METHODS: We defined percent stenosis of an intracranial artery as follows: percent stenosis = [(1 − (Dstenosis/Dnormal))] × 100, where Dstenosis = the diameter of the artery at the site of the most severe stenosis and Dnormal = the diameter of the proximal normal artery. If the proximal segment was diseased, contingency sites were chosen to measure Dnormal: distal artery (second choice), feeding artery (third choice). Using a hand-held digital caliper, three neuroradiologists independently measured Dstenosis and Dnormal of 24 stenotic intracranial arteries. Each observer repeated the readings 4 weeks later. We determined how frequently two observers' measurements of percent stenosis of each of the 24 diseased arteries differed by 10% or less.
RESULTS: Among the three pairs of observers, interobserver agreements were 88% (observer 1 versus observer 2), 79% (observer 1 versus observer 3), 75% (observer 2 versus observer 3) for the first reading and were 75% (observer 1 versus observer 2), 100% (observer 1 versus observer 3), and 71% (observer 2 versus observer 3) for the second reading. Intraobserver agreement for each of the observers was 88%, 83%, and 100%. Interclass correlation was 85% (first reading) and 87% (second reading). Intraclass correlation was 92% (first and second readings combined).
CONCLUSION: This method shows good interobserver and intraobserver agreements for the measurement of intracranial stenosis of a major artery. If validated in subsequent studies, this method may serve as a standard for the measurement of percent stenosis of an intracranial artery.
Atherosclerotic stenosis of the major intracranial arteries is an important cause of ischemic stroke. Currently, there are no standard methods for measuring the severity of intracranial arterial stenosis. The established methods for measuring extracranial carotid stenosis are not suitable for measuring percent stenosis of a major intracranial artery because the intracranial arteries have several branches, they become slightly narrower in their distal portions, and they are often tortuous (1–3). Additionally, extracranial carotid measurement techniques have to contend with the carotid bulb, which has no equivalent in any of the intracranial arteries.
In this study, we established measurement criteria for determining percent stenosis of the major intracranial arteries (carotid, middle cerebral, vertebral, basilar) and determined the interobserver/intraobserver agreements and interclass/intraclass correlations of these measurements.
Methods
Equation for Measuring Intracranial Arterial Stenosis
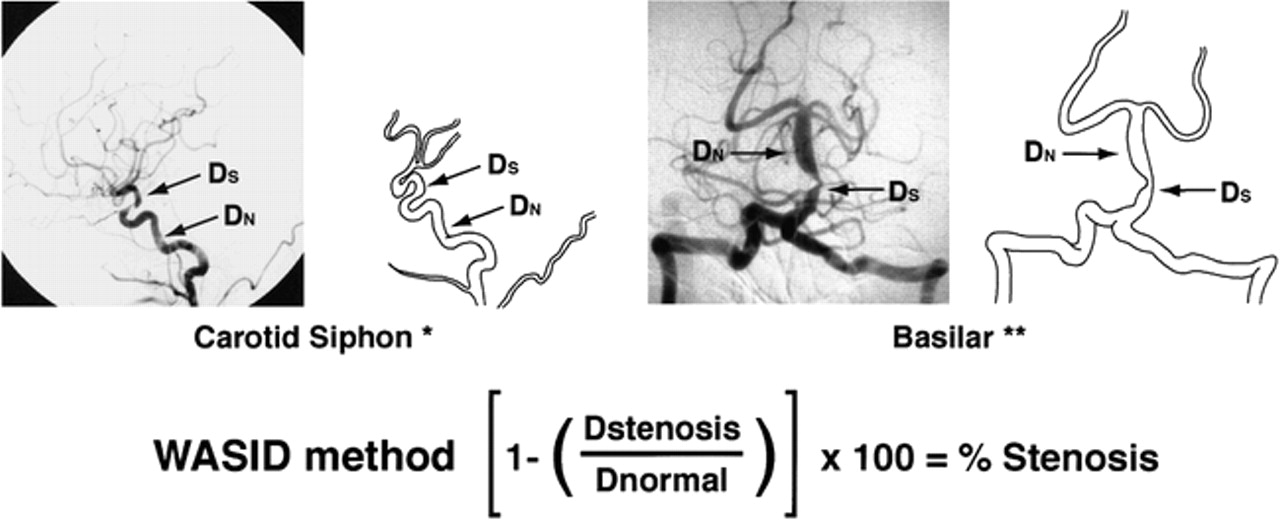
The equation used for determining percent stenosis of a major intracranial artery was as follows: percent stenosis = [(1 − (Dstenosis/Dnormal))] × 100, where Dstenosis = the diameter of the artery at the site of the most severe degree of stenosis and Dnormal = the diameter of the proximal normal artery. Dnormal was determined by the following criteria: for the middle cerebral, intracranial vertebral, and basilar arteries, the diameter of the proximal part of the artery at its widest, non-tortuous, normal segment was chosen (first choice). If the proximal artery was diseased (eg, middle cerebral artery origin stenosis), the diameter of the distal portion of the artery at its widest, parallel, non-tortuous normal segment was substituted (second choice). If the entire intracranial artery was diseased, the most distal, parallel, non-tortuous normal segment of the feeding artery was measured (third choice). For example, if the entire basilar artery was diseased, Dnormal was measured at the most distal, parallel, non-tortuous normal segment of the dominant vertebral artery; if the entire middle cerebral artery was diseased, Dnormal was measured at the most distal, parallel segment of the supraclinoid carotid artery; if the entire intracranial vertebral artery was diseased, Dnormal was measured at the most distal, parallel, non-tortuous normal segment of the extracranial vertebral artery. Because of the variability of vasculature size, slight magnification differences, and subtle differences in anteroposterior projection, the contralateral circulation was not used as the “normal” reference measurements.
Measurement of the intracranial carotid artery required a slightly different approach because the caliber of this artery often gets slightly smaller after the origin of the ophthalmic artery, and measuring the normal cavernous portion of the intracranial carotid artery can be difficult because of the tortuosity of these segments. With this in mind, Dnormal for the precavernous, cavernous, and postcavernous stenoses was measured at the widest, non-tortuous, normal portion of the petrous carotid artery that had parallel margins (first choice). If the entire petrous carotid was diseased, the most distal, parallel part of the extracranial internal carotid artery was substituted (second choice). Figure 1 illustrates how these rules were applied for measuring a stenosis of the carotid siphon and basilar artery.

WASID: Warfarin-Aspirin Symptomatic Intracranial Disease. The WASID method is used in the multicenter clinical trial assessing the efficacy of warfarin versus aspirin in cases of symptomatic intracranial stenosis
If tandem intracranial lesions were present (eg, distal vertebral and mid-basilar), percent stenosis of both sites was measured and the more severe stenosis was selected. When a “gap sign” was present (ie, the lumen of the vessel could not be visualized at the site of severe stenosis), Dstenosis could not be measured with calipers. In these cases, percent stenosis was defined as 99% luminal stenosis.
Angiogram Selection, Measuring Technique
After undergoing detailed training in the measurement criteria outlined above, three neuroradiologists independently evaluated 24 angiograms showing stenoses of 24 diseased intracranial arteries: nine carotid, seven middle cerebral, five basilar, and three vertebral arteries. The angiograms were chosen by reviewing the radiology log reports at Emory University Hospital between March and July 1996. Those angiograms with at least 50% stenosis of a major intracranial artery by “eye ball” estimation were selected. None of the neuroradiologists participated in the selection process. The radiographic view (anteroposterior or lateral) that revealed the highest degree of stenosis of each arterial lesion was provided to each reader. After obtaining a single measurement of Dstenosis and Dnormal, the percent diameter stenosis was calculated. Four weeks later, after rules for measuring intracranial stenosis were reinforced, each observer repeated the readings, blinded to their initial measurements.
Using a hand-held electronic caliper, all measurements were made at 90° to the arterial wall, extended point type (Mitutoyo 573–225010). This caliper has two narrow tips that do not obscure the margins of the arterial wall when measurements are obtained. A liquid crystal display provides measurements to 1/100 mm. The accuracy of the caliper is within 0.025 mm. All measurements were obtained on a horizontal lighted view box using a freestanding adjustable lighted magnifying glass (×10).
Statistical Analysis
Measurements of repeatability (measuring the same film by the same reader) and reproducibility (measuring the same film by different readers) were determined by fitting a nested analysis of variance model in which the reader factor was nested within the film factor and the repeated readings of the same film were nested within the reader factor. Both factors, film and reader, were considered as random factors (4, 5).
As a measure of repeatability, we calculated confidence intervals (95%, 90%, 85%) for the difference between the two readings of the same film by the same reader. The interpretation of this measure is that the difference between two readings of the same film by the same reader would differ by no more than this amount, half the width of the confidence interval, 95%, 90%, or 85% of the time.
As a measure of reproducibility, 95%, 90%, and 85% confidence intervals were also calculated for the difference between two readings of the same film by two different readers. Similarly, the interpretation of this measure is that the difference between the two readings of the same film by different readers would differ by no more than this amount, half the width of the confidence interval, 95%, 90%, or 85% of the time.
The analysis of variance model also provided estimates of the interclass and intraclass correlation coefficients. As a descriptive measure of repeatability, we calculated the percent of films for which the two readings of a film by the same reader were within 10% of each other (intraobserver variation). Similarly, for reproducibility, we calculated the percent of films for which the two readings of the same film by different readers were within 10% of each other (interobserver variation). This was done separately for each pairing of the three readers for both the first and second readings.
Results
Repeatability
Among the three readers, intraobserver agreement or the percent of films in which the difference in percent stenosis between the first and second reading of a film by the same reader were less than 10% varied from 83% to 100% (81% to 100% excluding gap sign films) (Table 1). The intraclass correlation coefficient was 0.93. The estimate of the standard deviation of repeated readings of a film by the same reader based on the analysis of variance model was 3.9.
Intraobserver agreement (% stenosis within 10%)
Based on confidence intervals of 95%, 90%, and 85%, estimates of repeatability were 10.8%, 9%, and 6.8%, respectively. This indicated that 95%, 90%, and 85% of the time, we would expect the difference in measurements of percent stenosis between repeated measurements of the same angiogram by the same reader to be less than 10.8%, 9%, and 6.8%, respectively.
Reproducibility
Among the pairings of the three readers, interobserver agreement or the percent of films in which the difference in percent stenosis measured by two readers was less than 10% varied from 71% to 100% (67% to 100% excluding gap sign films) (Table 2). The interclass correlation coefficient among the three readers was .85 for the first reading and .87 for the second reading.
Interobserver agreement (% stenosis within 10%)
Based on confidence intervals of 95%, 90%, and 85%, estimates of repeatability were 15.7%, 13.2%, and 11.7%, respectively. This indicated that 95%, 90%, and 85% of the time we would expect the difference in measurements of percent stenosis of the same film by different readers to be less than 15.7%, 13.2%, and 11.7%, respectively.
Discussion
Angiographic measurement standards for determining percent stenosis of the extracranial internal carotid artery are well established (1–3, 6). These methods are routinely used in clinical practice to identify patients who may benefit from carotid endarterectomy. Currently, there is no equivalent method for measuring percent stenosis of the major intracranial arteries. This may be because until recently, there were limited data on the impact of the severity of intracranial stenosis on the risk of ischemic stroke. Recent studies suggest that the annual risk of stroke in patients with at least 50% stenosis of a major intracranial artery is 4% to 10% (7). Moreover, patients with severe intracranial stenosis (70% to 99%) have a higher risk of stroke than do patients with moderate intracranial stenosis (50% to 69%) (7). If the prognosis of intracranial arterial stenosis and the choice of therapy (eg, anticoagulation, angioplasty) for these patients are clearly shown to be based on the severity of intracranial stenosis, a reproducible and repeatable method for measuring percent stenosis of the major intracranial arteries will be required. In our study, intracranial arterial stenoses of more than 50% were chosen because of the significance of the stroke risk of high-grade intracranial stenosis as compared with lesions of lesser severity. Future studies may address low- and moderate-grade intracranial stenoses.
The method developed in this study seems to fulfill these criteria. Using a narrow agreement range (ie, within 10% of each reader's measurement of percent stenosis), interobserver agreements for the three readers ranged from 71% to 100% and intraobserver agreements ranged from 83% to 100%. These rates of observer agreements are similar to those reported for the extracranial carotid artery (8) and exceed those reported for the coronary arteries (9). In a study assessing measurement of extracranial carotid stenosis, Rothwell et al (8) reported interobserver agreements of percent stenosis within 10% of two readers' measurements as 70% for the European Carotid Surgery Trial (ECST) method, 74% for the North American Symptomatic Carotid Endarterectomy Trial (NASCET) method, and 75% for the Common Carotid method. Zir et al (9) reported a low interobserver agreement of four coronary angiographers in the interpretation of coronary artery stenosis. In this study, interobserver agreement for proximal or mid-left anterior descending stenosis (within 10%) ranged from 0% to 40%. The four observers in this study agreed regarding the presence of at least 50% stenosis in only 45% of left anterior descending lesions and 65% of right coronary artery lesions. The authors reported that a major reason for the poor results was disagreement regarding where to measure the normal vessel, Dnormal. Thus, development of specific criteria for measuring Dnormal was suggested as one method of reducing interobserver variability. Hence, in the present study, we defined specific rules for determining the specific site at which to measure Dnormal. Moreover, the three participating neuroradiologists in the present study underwent extensive training with reinforcement of the rules before obtaining their second measurements. We suspect that the success of this measuring technique depends in large portion on ability to follow these rules.
This study has shown that obtaining reproducible measurements of percent stenosis of an intracranial artery by using conventional cerebral angiography is possible using standardized measurement criteria. If validated in further studies, this method may serve as a standard for the measurement of percent stenosis of an intracranial artery obtained using conventional angiography.
Footnotes
↵1 Address reprint requests to Owen B. Samuels, MD, Emory University, Department of Neurosurgery, 1365 Clifton Road N.E., Clinic Building B, Suite 6400, Atlanta, GA 30322.
References
- Received August 14, 1998.
- Accepted after revision September 28, 1999.
- Copyright © American Society of Neuroradiology
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Evaluation of flow diverters for cerebral aneurysm therapy: recommendations for imaging analyses in clinical studies, endorsed by ESMINT, ESNR, OCIN, SILAN, SNIS, and WFITN
- The pEGASUS-HPC stent system for intracranial arterial stenosis: a single-center case series
- Comprehensive Analysis of Neurologic Complications following Transradial Cerebral Angiography
- Is invasive fractional flow measurement accurate in intracranial stenosis? A computational simulation study
- Development and validation of a SCORing systEm for pre-thrombectomy diagnosis of IntraCranial Atherosclerotic Disease (Score-ICAD)
- DRug-coated Balloon for Endovascular treatment of sYmptOmatic intracraNial stenotic Disease (DR. BEYOND): the protocol of a multicentre randomised trial
- MetS in the prediction of asymptomatic intracranial arterial stenosis: the potential mediating role of hsCRP
- Comprehensive imaging analysis of intracranial atherosclerosis
- Comparison of drug-coated balloon with bare-metal stent in patients with symptomatic intracranial atherosclerotic stenosis: the AcoArt sICAS randomized clinical trial
- Tmax >4 s volume predicts stroke recurrence in symptomatic intracranial atherosclerotic stenosis with optimal medical treatment
- Effects of different endovascular treatments on cerebral perfusion changes and stroke recurrence in patients with intracranial atherosclerosis
- Prognostic value of angiographic based quantitative flow ratio and anatomic features in intracranial atherosclerotic stenosis
- Prevalence of intracerebral thrombus detected by optical coherence tomography in patients with posterior circulation stroke or transient ischemic attack
- Development and validation of a SCORing systEm for pre-thrombectomy diagnosis of IntraCranial Atherosclerotic Disease (Score-ICAD)
- First-in-human experience of sirolimus coated balloon for symptomatic intracranial artery stenosis
- First-in-human trial of a self-expandable, temporary dilation system for intracranial atherosclerotic disease in patients presenting with acute ischemic stroke
- Association of Cerebral Microbleeds and Risk of Stroke and Mortality in Posterior Circulation Cerebral Infarction
- Impact of qualifying artery on the efficacy of stenting plus medical therapy versus medical therapy alone in patients with symptomatic intracranial stenosis: a post-hoc analysis of the CASSISS trial
- Colchicine in patients with acute ischaemic stroke or transient ischaemic attack (CHANCE-3): multicentre, double blind, randomised, placebo controlled trial
- Hyperintense Acute Reperfusion Marker Sign in Patients with Diffusion Weighted Image-negative Transient Ischemic Attack HARM Sign in DWI-negative TIA
- Detailed phenotype of RNF213 p.R4810K variant identified by the Chinese patients with acute ischaemic stroke or transient ischaemic attack
- Comparison of drug-coated balloon angioplasty versus standard medical therapy on recurrent stroke and mortality rates among patients with symptomatic intracranial atherosclerotic stenosis: protocol for a systematic review and meta-analysis
- Association of the LIfestyle for BRAin Health Score and Brain Vascular Damage in a Community-Dwelling Adults Cohort
- Detailed phenotype of RNF213 p.R4810K variant identified by the Chinese patients with acute ischaemic stroke or transient ischaemic attack
- Clinical Relevance of Plaque Distribution for Basilar Artery Stenosis
- Somatic mutation contributing to clonal haematopoiesis is a risk factor of recurrent stroke in first-ever acute ischaemic stroke: a prospective cohort study
- Association Between the Degree of Vertebrobasilar Stenosis, Location, Infarction Pattern and QMRA Flow State
- Clinical Relevance of Plaque Distribution for Basilar Artery Stenosis
- Risk stratification in symptomatic intracranial atherosclerotic disease with conventional vascular risk factors and cerebral haemodynamics
- Differential associations of lipoprotein(a) level with cerebral large artery and small vessel diseases
- Effect of the RNF213 p.R4810K Variant on the Progression of Intracranial Artery Stenosis: A 15-Year Follow-up Study
- Predictors of incomplete aneurysm occlusion after treatment with the Pipeline Embolization Device: PREMIER trial 1 year analysis
- Somatic mutation contributing to clonal haematopoiesis is a risk factor of recurrent stroke in first-ever acute ischaemic stroke: a prospective cohort study
- Association of residual stenosis after balloon angioplasty with vessel wall geometries in intracranial atherosclerosis
- Safety and efficacy of balloon-mounted stent in the treatment of symptomatic intracranial atherosclerotic disease: a multicenter experience
- Cerebral angiographic features of central retinal artery occlusion patients treated with intra-arterial thrombolysis
- Thromboelastography predicts dual antiplatelet therapy-related hemorrhage in patients with acute ischemic stroke
- Genome sequencing reveals the role of rare genomic variants in Chinese patients with symptomatic intracranial atherosclerotic disease
- Atrial cardiomyopathy in patients with ischaemic stroke: a cross-sectional and prospective cohort study--the COAST study
- Safety of endovascular therapy for symptomatic intracranial artery stenosis: a national prospective registry
- Prevalence of Intracranial Atherosclerotic Disease in Patients with Low-Risk Transient or Persistent Neurologic Events
- Large Culprit Plaque and More Intracranial Plaques Are Associated with Recurrent Stroke: A Case-Control Study Using Vessel Wall Imaging
- Association between coexisting intracranial artery and extracranial carotid artery atherosclerotic diseases and ipsilateral cerebral infarction: a Chinese Atherosclerosis Risk Evaluation (CARE-II) study
- Metabolic syndrome, intracranial arterial stenosis and cerebral small vessel disease in community-dwelling populations
- Correlation between intracranial vertebral artery stenosis diameter measured by digital subtraction angiography and cross-sectional area measured by optical coherence tomography
- Balloon-mounted stenting for ICAS in a multicenter registry study in China: a comparison with the WEAVE/WOVEN trial
- Low serum albumin levels predict poor outcome in patients with acute ischaemic stroke or transient ischaemic attack
- Intracranial arterial stenosis in Caucasian versus Chinese patients with TIA and minor stroke: two contemporaneous cohorts and a systematic review
- Vessel Wall Enhancement on Black-Blood MRI Predicts Acute and Future Stroke in Cerebral Amyloid Angiopathy
- Plaque morphology in acute symptomatic intracranial atherosclerotic disease
- Concurrent intracranial and extracranial artery stenosis and the prognosis of transient ischaemic symptoms or imaging-negative ischaemic stroke
- Association of elevated hs-CRP and multiple infarctions with outcomes of minor stroke or TIA: subgroup analysis of CHANCE randomised clinical trial
- Association between asymptomatic intracranial arterial stenosis and insulin resistance or diabetes mellitus: a cross-sectional study in rural Shandong, China
- Cerebral small vessel disease or intracranial large vessel atherosclerosis may carry different risk for future strokes
- Association between kidney disease measures and intracranial atherosclerosis: The ARIC study
- MRI Vessel Wall Imaging after Intra-Arterial Treatment for Acute Ischemic Stroke
- Fractional Flow on TOF-MRA as a Measure of Stroke Risk in Children with Intracranial Arterial Stenosis