
Article Figures & Data
Figures
- fig 1.
Schematic representation of the three basic drainage pathways of the SMCV according to San Millán Ruíz et al (4). Superior view of the anterior, middle, and posterior cranial fossa (ACF, MCF, and PCF, respectively). The SMCV may continue as a paracavernous sinus coursing laterally over the MCF (a), as an LCS enclosed within the lateral wall of the CS (b), or may terminate into the anterosuperior aspect of the CS (c). Venous outflow toward the pterygoid plexus via a skull base foramen is shown for the LCS. 1, superior ophthalmic vein; 2, CS; 3, inferior petrosal sinus; 4, sigmoid sinus; 5, transverse sinus; 6, SMCV
- fig 2.
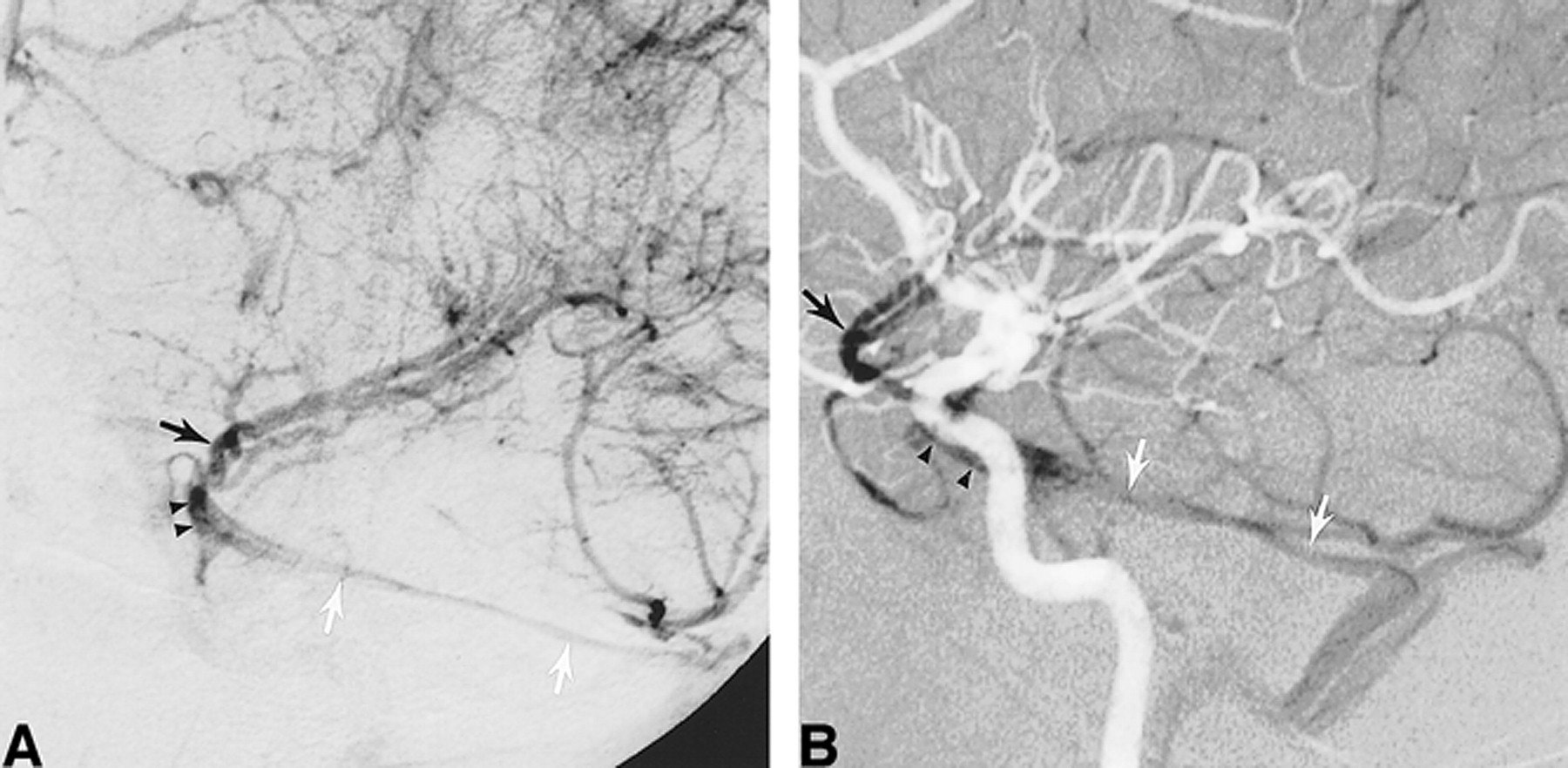
DSA, venous phase, in a 59-year-old man examined for carotid bifurcation atheromatous disease. Intracranial vasculature is normal.
A, Left ICA injection, lateral view. The left SMCV (black arrow) continues as an LCS (arrowheads), coursing posteriorly and inferiorly and projecting over the sellar region. In this case, note that the LCS drains toward the pterygoid plexus (white arrow) through foramina in the middle cranial fossa floor.
B, Left ICA injection, AP view. The left SMCV (arrow) is opacified, as is a left LCS (arrowheads). There is no opacification of the left CS.
C, Right ICA injection, AP view. Venous blood coming from the right cerebral hemisphere opacifies both the right CS (R) and left CS (L) through intercavernous connections. Note also opacification of the left inferior petrosal sinus (arrowheads), which was not visible on the left ICA injection.
- fig 3.
Schematic representation of the laterosellar venous spaces, coronal view. The medial and lateral compartments of the CS and the LCS are shown in different shades of gray, as indicated at the bottom of the figure. The medial and lateral compartments of the CS are plexiform groups of veins lying on the medial and lateral aspects of the ICA, respectively. The LCS is a venous structure showing the morphologic characteristics of a dural sinus, located in between the outer (A) and inner (B) layers of the lateral wall of the CS. ICA indicates cavernous segment of the ICA; MCF, middle cranial fossa; P, pituitary gland; SB, sphenoid bone and sinus
- fig 4.
DSA, venous phase, in a 52-year-old woman examined for subarachnoid hemorrhage.
A, Right ICA injection, AP view. A duplicated SMCV (black arrows) runs medially toward the CS region to continue its course as an LCS (arrowheads), which terminates into the posterior aspect of the right CS via a small anastomotic channel (white arrow). The medial (M) and lateral (L) compartments of the CS and the right inferior petrosal sinus are well delineated. The left CS and inferior petrosal sinus are faintly opacified through intercavernous connections. The inner layer of the lateral wall of the CS is well appreciated as a curvilinear opacification defect located between the LCS and the lateral compartment of the CS.
B, Right ICA injection, AP view, sequential subtraction technique. Simultaneous visualization of the arterial (light) and venous (dark) phases confirms that the small anastomotic channel connects the LCS to the lateral compartment of the CS, the latter abutting the lateral aspect of the cavernous segment of the left ICA.
- fig 5.
DSA, venous phase, in a 46-year-old man examined for subarachnoid hemorrhage. Cerebral angiogram showed an anterior communicating artery aneurysm.
A, Right internal carotid injection, AP view, sequential subtraction technique. The right SMCV (arrow) courses medially toward the CS region and continues posteriorly as an LCS (arrowheads). The LCS is lateral to the ICA, but not in its immediate proximity, and assumes a slitlike appearance. Since there is no connection between the LCS and the CS, the latter do not opacify and the LCS is consequently well appreciated. When connections allow for opacification of both the LCS and the CS, a slitlike LCS may be difficult to observe angiographically. Note the saccular aneurysm located at the right A1/A2 anterior communicating artery junction.
B, Right internal carotid injection, lateral view. Owing to its thin configuration, the slitlike LCS (arrowheads) faintly opacifies on a lateral view. Note the drainage pathway toward the pterygoid plexus (arrow).
- fig 6.
DSA, venous phase, in a 38-year-old man examined for subarachnoid hemorrhage.
A, Left ICA injection, left anterior oblique view. The left SMCV (black arrow) courses medially toward the CS region but continues posteriorly as an LCS (arrowheads) and then as an SPS (white arrows), ending in the left transverse sinus. There is no connection with the CS, which is not opacified.
B, Left ICA injection, lateral view, sequential subtraction technique. The arterial (light) and venous (dark) phases are displayed simultaneously, enabling visualization of their topographic relationship. The LCS (arrowheads) is seen overlying the cavernous segment of the left ICA. Posteriorly, it continues as the left SPS (white arrows) coursing over the petrous ridge before reaching the left transverse sinus. Black arrow indicates the left SMCV.
- fig 7.
DSA, venous phase, in a 37-year-old woman undergoing a presurgical epilepsy workup (Wada test).
A, Right internal carotid injection, AP view. The right SMCV (arrow) drains toward the right transverse sinus via an LCS. A small anastomotic channel (arrowhead) joins the LCS to the posterior aspect of the CS at the skull base.
B, Right internal carotid injection, lateral view. The simultaneous opacification of the LCS and the CS (medial and lateral compartments) makes it impossible to differentiate them on the lateral view.
C, Left internal carotid injection, AP view. The left SMCV (arrow) drains toward the left pterygoid plexus (PP) via an LCS (arrowheads). There is an “en passant” connection between the LCS and the lateral compartment (L) of the CS.
- fig 8.
DSA, venous phase, in a 68-year-old man examined for carotid bifurcation atheromatous disease.
A, Right common carotid injection, AP view. The left SMCV (black arrow) drains into a right LCS (arrowheads). The right CS is opacified as well, although no significant connections are observed. Note the linear opacification defect of the inner layer of the CS lateral wall, separating the LCS from the lateral compartment of the CS. A second, round opacification defect is visible within the CS itself, corresponding to the cavernous segment of the right ICA (white arrow). This anatomic landmark enables one to discern the medial and lateral compartments of the CS.
B, Magnified view of the right laterosellar venous spaces. This dynamic sequence (1 to 6) was acquired at the rate of one image per second. Note that the LCS appears early in the sequence while the medial and lateral compartments of the CS show homogeneous opacification after a delay of approximately 5 seconds. This is consistent with the findings of Bonneville et al (2), who observed, during dynamic CT of the laterosellar venous spaces, a delay of 5 seconds between the visualization of distinct laterosellar veins and a homogeneous opacification of the CS. Note on the last image of the sequence the particularly well delineated inner layer of the CS lateral wall.








Tables
 TABLE 1:
TABLE 1:Indication for cerebral angiography in the studied patient population
- TABLE 2:
Drainage patterns of the paracavernous and laterocavernous sinuses

In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Non-aggressive, sinus-type greater sphenoid wing dural arteriovenous fistula with shunt point in the laterocavernous sinus mimicking a cavernous sinus dural arteriovenous fistula converted to aggressive, non-sinus-type
- Cerebral venous anatomy: implications for the neurointerventionalist
- Cerebral venous anatomy: implications for the neurointerventionalist
- Republished: Embolization of a cavernous carotid fistula through the vein of Labbe: a new alternative transvenous access route
- Embolization of a cavernous carotid fistula through the vein of Labbe: a new alternative transvenous access route
- New Concept in Cavernous Sinus Dural Arteriovenous Fistula: Correlation With Presenting Symptom and Venous Drainage Patterns
- The Sphenoparietal Sinus of Breschet: Does It Exist? An Anatomic Study