
Abstract
BACKGROUND AND PURPOSE: The transluminal angioplasty and stenting procedure has been recently advocated as a potential alternative to surgical endarterectomy for the treatment of severe extracranial carotid stenosis. This study assesses the incidence and significance of intracranial hemorrhage occurring after this procedure.
METHODS: We retrospectively reviewed 104 carotid arteries (96 internal, two external, and six common) in 90 patients (63 male; mean age, 69.4 years; range, 48–88 years) who underwent primary stenting and angioplasty by use of Wallstents (103/104) at three centers between January 1996 and January 1999. Seventy-five (83%) patients were referred by neurosurgery departments. Seventy-one (68%) arteries were symptomatic; the mean stenosis percentage was 85% (range, 40–99%).
RESULTS: Four intraparenchymal hemorrhages occurred, representing 4.4% of patients and 3.8% of vessels, after angioplasty and stent placement. The mean preoperative stenosis percentage was 95% (range, 90–99%). One hemorrhage occurred immediately after stent placement, whereas the three other hemorrhages occurred in a delayed fashion (mean, 2.8 days). The mean hematoma size was 4.8 cm (range, 2–8 cm). Three patients had associated subarachnoid or intraventricular bleeding; the fourth had associated subdural hemorrhage. Three hemorrhages were fatal; the fourth experienced two seizures only. No acute neurologic symptoms were present prior to hemorrhages, and there was no postprocedural hypertension in these patients. All had been receiving antiplatelet agents as well as intraprocedural IV heparin.
CONCLUSION: Intracranial hemorrhage can occur after carotid angioplasty and stenting. We speculate that this represents cerebral hyperperfusion injury. The 3.8% incidence of cerebral hemorrhage observed is approximately sixfold greater than that reported post endarterectomy (0.6%) (95% CI, 0.2–8.7%). This is not statistically significant in this small study group. This trend may reflect patient selection, different anticoagulation protocols, and/or study population size. Additional data are needed to determine the safety and efficiency of carotid stenting as a treatment for carotid stenosis.
Atherosclerotic disease of extracranial carotid arteries is responsible for approximately 20% to 30% of strokes in North America each year. The North American Symptomatic Carotid Endarterectomy Trial (NASCET) (1) and the Asymptomatic Carotid Atherosclerosis Study (ACAS) (2) have demonstrated the utility of carotid endarterectomy in reducing the stroke rate in patients with moderate- to high-grade stenoses: >50% and >60% stenoses for symptomatic and asymptomatic patients, respectively. Recently, the percutaneous transluminal angioplasty and stenting procedure has been advocated as an alternative to endarterectomy (3–5). A randomized clinical trial, the Carotid Revascularization Endarterectomy versus Stent Trial (CREST) is currently being organized to compare these two techniques directly.
Massive intracranial hemorrhage after endarterectomy has been reported in multiple large series as an uncommon but devastating event, occurring in approximately 0.6% of cases (6–9). To date, there has been only one report of an isolated case of intracranial hemorrhage after angioplasty and stenting (10). This study reports the incidence of intracranial hemorrhage after angioplasty and stenting in a consecutive series of patients collected from three centers.
Methods
We performed a retrospective review of 104 consecutive carotid arteries in 90 patients who underwent angioplasty and stenting at three centers between January 1996 and January 1999. All patients were deemed poor surgical candidates. Seventy-five (83%) patients were referred by neurosurgeons; 71 (68%) arteries were symptomatic. Mean stenosis percentage was 85% (range, 40–99%) according to NASCET criteria. A similar stenting technique was used at each center, with predilatation of the stenotic lesion, deployment of a self-expandable stent, and balloon dilatation of the stent. One hundred three of 104 vessels were treated with Wallstents (Schneider Inc., Minneapolis, MN) that measured either 10 × 20 mm or 10 × 48 mm. No distal protection was used. All patients received antiplatelet medication prior to and after the procedure (typically ASA 325 mg PO QD or Ticlopidine 250 mg PO BID). A bolus of IV heparin was administered during the procedure (100 μ/kg plus 1000–2000 μ/hr), which was not reversed at completion. Blood pressure was monitored and controlled pre- and postprocedurally. Aspirin and Ticlopidine were maintained for 4 weeks after the procedure, after which Ticlopidine was discontinued.
Results
Of the 90 patients (104 carotid arteries) who underwent carotid angioplasty and stenting, four had an intracerebral hemorrhage, representing 4.4% of patients or 3.8% of vessels treated. The mean preoperative stenosis was 95% in these patients. No acute neurologic symptoms were present prior to hemorrhages, and there was no postprocedural hypertension in these four patients. No vessel occlusions were identified on postprocedural angiograms. Patient profiles are shown in Table 1.
Acute Intracranial Hemorrhage Postangioplasty and Stenting—Patient Profile
Acute hemorrhage occurred from immediately to 6 days postoperatively, with a mean of 2 days. Three hemorrhages were fatal. The mean hematoma size was 4.8 cm. Associated subarachnoid or intraventricular blood was present in three of four patients; the fourth patient had associated subdural hemorrhage. Three of the hemorrhages occurred at one center, two at the main campus (one fatal and one minor), and one at the secondary campus (fatal). The fourth hemorrhage (fatal) occurred at a different center, and involved operators from both of the other two sites. Results are summarized in Table 2. Case illustrations are presented in Figures 1 through 3.
Acute Intracranial Hemorrhage Postangioplasty and Stenting—Hemorrhage Characteristics

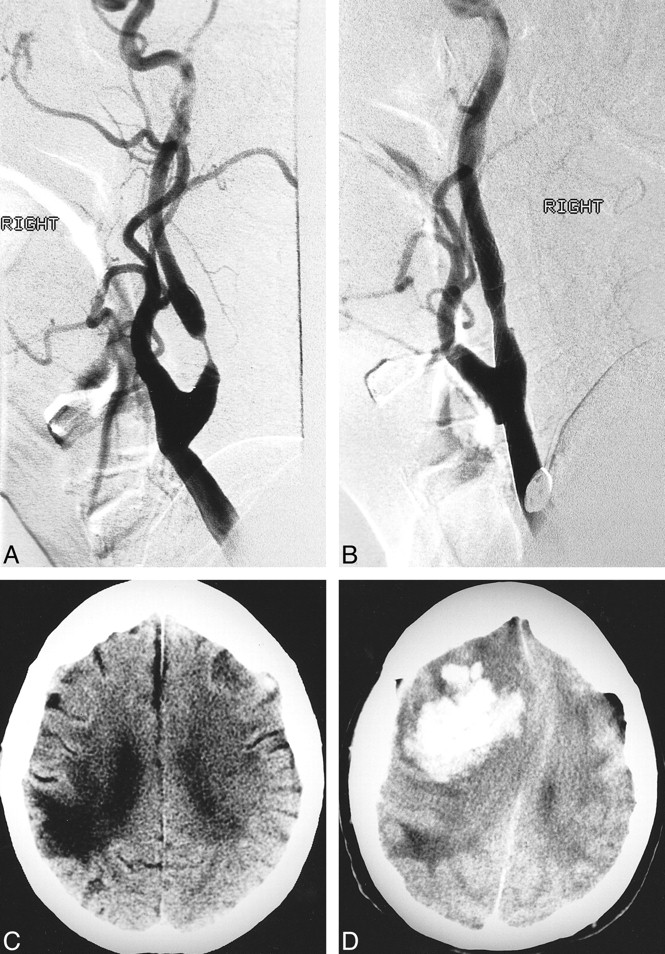
Patient 2. A, Ninety percent right internal carotid artery stenosis.
B, Postoperative angiogram shows a 30% residual stenosis post stenting.
C, CT of head at discharge shows an old, right, parietal infarct.
D, CT head 2 days postoperatively depicts a large, right, frontal hematoma with a small subdural hematoma.

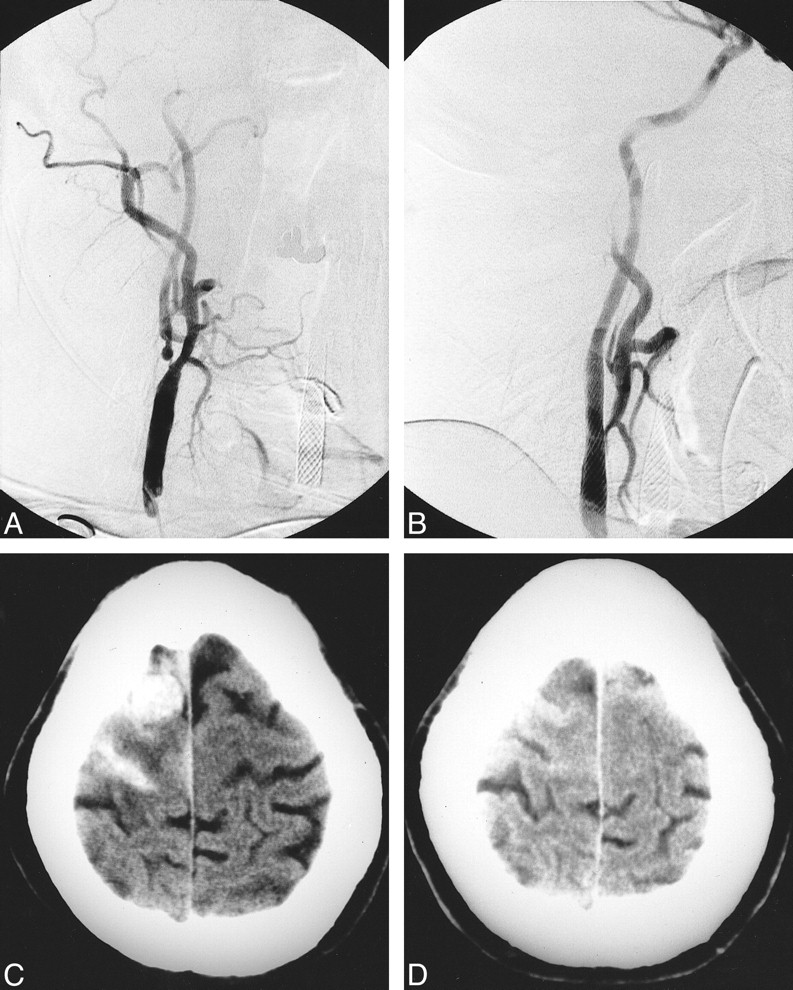
Patient 3. A, Ninety-nine percent right internal carotid artery stenosis. A left external carotid stent is also visualized. The left internal carotid artery is occluded.
B, Postprocedural angiogram with no significant residual stenosis post angioplasty and stenting.
C, CT of head 6 days postoperatively reveals an acute frontal hematoma with associated subarachnoid hemorrhage. The patient was clinically well until he experienced a generalized seizure approximately 2 hours prior to the CT scan.
D, Two-week follow-up reveals marked resolution of hemorrhage.

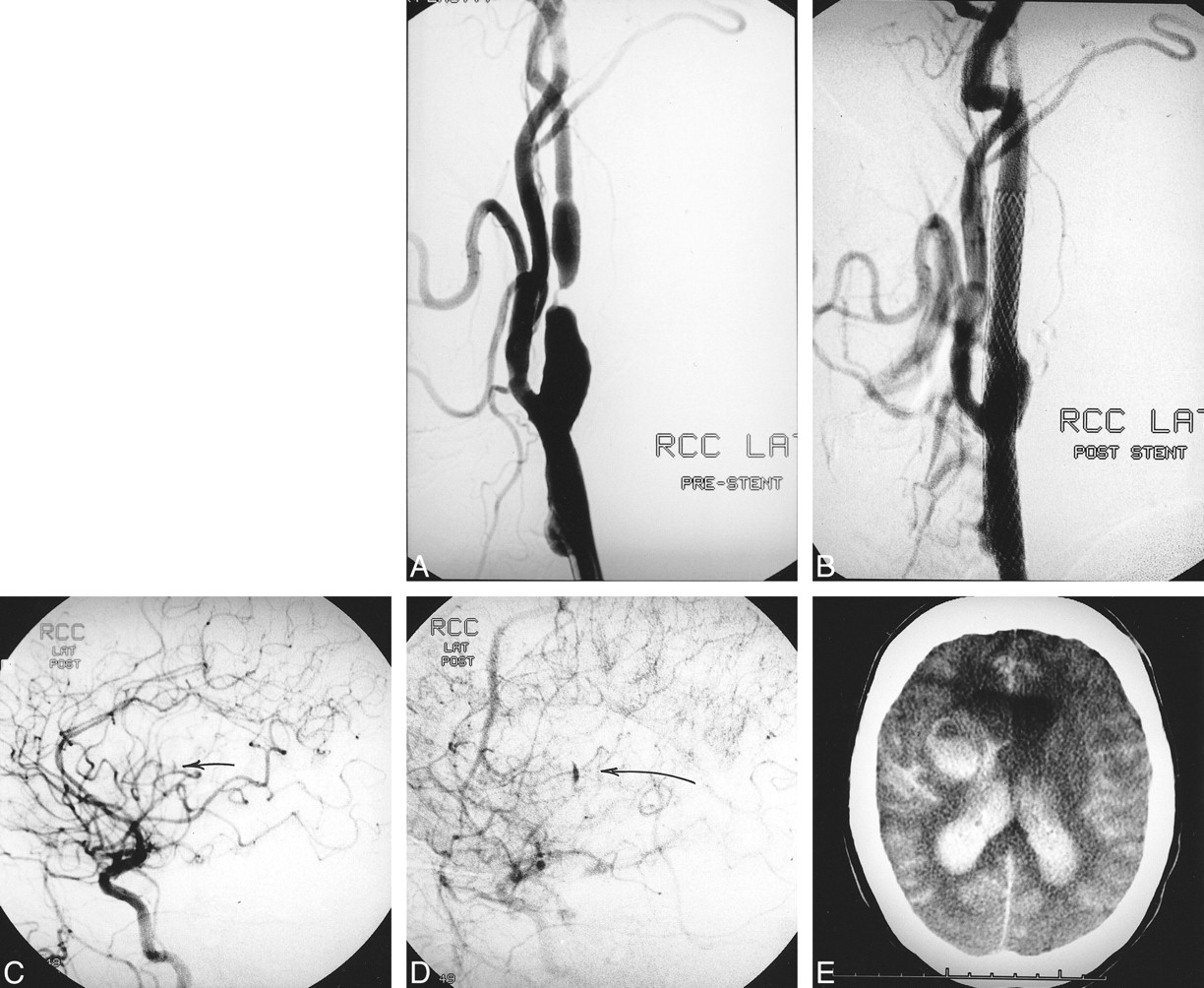
Patient 4. A, Ninety-five percent right internal carotid artery stenosis.
B, Post angioplasty and stenting with no significant residual stenosis.
C and D, Angiogram immediately post stenting demonstrates extravasation from a lenticulostriate artery (arrow). At no time during the procedure did a catheter or guidewire enter into the intracranial circulation.
E, CT of head postoperatively shows a right basal ganglia, intraventricular, and subarachnoid hemorrhage as well as hydrocephalus.
Discussion
Since the emergence of angioplasty and stenting of the extracranial carotid arteries as a potential treatment of carotid stenosis, there has been much discussion surrounding the associated complication rate relative to carotid endarterectomy. Large series of extracranial carotid angioplasty and stenting have revealed the incidence of stroke and death to be in the range of 3.6% to 7.9% (3–5). There has been no report to date in the literature regarding the incidence of postprocedural intracerebral hemorrhage after angioplasty and stenting. This has been reported as a rare complication of carotid endarterectomy, with an incidence of approximately 0.6% (6–9). Intracranial hemorrhage after endarterectomy is believed to result from hyperperfusion injury (6, 8, 11). Although we do not have pathologic evidence to support hyperperfusion injury as a cause of the hemorrhage observed post carotid angioplasty and stenting, the absence of 1) preprocedural acute infarction, 2) vascular occlusions at angiography, and 3) postprocedural systemic hypertension, together with the lobar appearance of the hemorrhages (Figs 1–3), all support a reperfusion-hyperperfusion mechanism of injury. Moreover, our radiographic observations of extravasating blood from a lenticulostriate artery immediately after angioplasty and stenting in a patient with unchanged pre- and postprocedural systemic blood pressure lends further support to the notion that relative hyperperfusion is the cause of intraparenchymal hemorrhage in this setting.
The onset of thromboembolic complications associated with either endarterectomy or angioplasty and stenting most commonly occurs in the immediate operative or perioperative period (5, 12). The onset of intracerebral hemorrhage after carotid revascularization by endarterectomy is variable, ranging from immediate up to 17 days postoperatively. The average time of onset is approximately 4 to 5 days (13). Although patients usually develop sudden neurologic deterioration, there may be some symptoms identified prior to the onset of intracerebral hemorrhage, including ipsilateral headache and focal seizures with or without secondary generalization (14).
In 1975, Sundt et al (15) described five patients who suffered seizures after carotid endarterectomy and all were found to have unusually high ipsilateral CBF attributable to reactive hyperemia from a long-standing carotid stenosis. A subsequent study of 11 patients with postendarterectomy seizures revealed preendarterectomy CBF to be 75% of normal and postendarterectomy ipsilateral CBF to have increased to 170% of normal (16). Furthermore, Schroeder et al (17) measured CBF before and after surgery in patients who underwent carotid endarterectomy and demonstrated hyperemic flow on the first postoperative day bilaterally. These investigators observed that, in patients with preoperative internal carotid artery stenosis greater than 50%, hemispheric flow was significantly increased in the cerebral hemisphere ipsilateral to the endarterectomy site relative to both the contralateral side and normal rates. This cerebral hyperperfusion persisted for up to 11 days.
The hyperperfusion syndrome is thought to be the result of failure of normal cerebral autoregulation involved in CBF, secondary to longstanding decreased perfusion pressure. Autoregulatory failure results in the cerebral arterioles being maximally dilated over a long period of time, with subsequent loss of their ability to constrict when normal perfusion pressure is restored (13, 14). Autoregulatory failure and cerebral hyperperfusion persists for some time after revascularization, but eventually normalizes (14). The pathologic consequence of autoregulatory failure appears to be similar to that of normal perfusion pressure breakthrough occasionally demonstrated after resection of cerebral arteriovenous malformations (18). In both these conditions, the restoration of normal CBF to chronically underperfused brain can result in edema, capillary breakthrough, and perivascular hemorrhages in association with fibrinoid necrosis of small arteries and macroscopic hemorrhages (11, 18). Similar pathologic findings have been reported in the presence of hypertensive encephalopathy in which a severe increase in CBF overwhelms the arteriolar vasoconstriction capacity, producing edema and perivascular hemorrhage (19).
In three large case series reviewing complications of carotid endarterectomies, intracranial hemorrhage was rare, occurring in only approximately 0.6% of patients. Despite this low rate of intracerebral hemorrhage, several variables have been identified as risk factors for the development of postrevascularization intracerebral hemorrhage. These include severe ipsilateral stenosis of 90% severity or greater, impaired collateral blood flow secondary to an advanced occlusive disease in other extracranial cerebral vessels or an incomplete circle of Willis, peri- and postoperative hypertension, and the use of antiplatelet agents or other types of anticoagulation (7, 9, 20).
Compared with the relatively low incidence of cerebral hemorrhage after carotid endarterectomy, we observed a 3.8% incidence of hemorrhage post angioplasty and stenting, representing approximately a sixfold increase in hemorrhage rate (95% CI, 0.2–8.7%). This is not a statistically significant difference, but patient numbers are small in this study. Larger studies will determine if this trend is significant. It is possible that our patients are of overall higher risk because of the severity of their stenoses or because of coexistent medical conditions. All patients in our series were deemed poor surgical candidates. The use of two antiplatelet agents (ASA and Ticlopidine) is a commonly used technique in coronary angioplasty and stenting, with a demonstrated decreased risk of stent thrombosis compared with the use of ASA alone (21). This antiplatelet aggregation protocol has been widely adopted for carotid angioplasty and stenting, and represents an increased level of antiplatelet therapy relative to that employed for endarterectomy. This may be a contributing factor in the increased incidence of intracranial hemorrhage seen in this series. Finally, if stent deployment followed by angioplasty results, at least acutely, in a greater increase in CBF relative to endarterectomy, this could potentially account for increased hyperperfusion injury. However, at this time it remains a matter of speculation whether this greater increase in CBF after angioplasty and stenting does account for increased hyperperfusion injury.
Symptomatic ischemic events occurred 6 weeks and 4 months, respectively, prior to angioplasty and stenting, in two of the four patients. Acute subclinical ischemia cannot be ruled out in this patient group, as diffusion-weighted MR imaging was not performed immediately prior to angioplasty and stenting. Although there was no clinical reason to suspect that these patients experienced subclinical ischemia different than the patient series as a whole, if this occurred, this could bias the results of the study.
Conclusion
Intracranial hemorrhage can occur as a complication of angioplasty and stenting of extracranial carotid arteries. This likely represents cerebral hyperperfusion injury. Our observation of an increased incidence of cerebral hemorrhage with angioplasty and stenting compared with endarterectomy, although not statistically significant in this small study group, may relate to patient selection, the size of the study population or to increased antiplatelet therapy. Additional data are needed to determine the safety and efficacy of angioplasty and stenting for treatment of carotid stenosis. Finally, techniques that measure CBF may help in early identification of patients with ipsilateral hyperperfusion post angioplasty and stenting, and allow for early intervention with aggressive blood pressure control. This, however, remains to be investigated.
References
- Received June 25, 1999.
- Accepted after revision April 26, 2000.
- Copyright © American Society of Neuroradiology
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Acute thromboses and occlusions of dual layer carotid stents in endovascular treatment of tandem occlusions
- Selective-versus-Standard Poststent Dilation for Carotid Artery Disease: A Systematic Review and Meta-Analysis
- Heterogeneous practice patterns regarding antiplatelet medications for neuroendovascular stenting in the USA: a multicenter survey
- Risk of Intracerebral Hemorrhage in Patients With Cerebral Microbleeds Undergoing Endovascular Intervention
- 2011 ASA/ACCF/AHA/AANN/AANS/ACR/ASNR/CNS/SAIP/SCAI/SIR/SNIS/SVM/SVS Guideline on the Management of Patients With Extracranial Carotid and Vertebral Artery Disease: Executive Summary: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, and the American Stroke Association, American Association of Neuroscience Nurses, American Association of Neurological Surgeons, American College of Radiology, American Society of Neuroradiology, Congress of Neurological Surgeons, Society of Atherosclerosis Imaging and Prevention, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of NeuroInterventional Surgery, Society for Vascular Medicine, and Society for Vascular Surgery
- 2011 ASA/ACCF/AHA/AANN/AANS/ACR/ASNR/CNS/SAIP/SCAI/SIR/SNIS/SVM/SVS Guideline on the Management of Patients With Extracranial Carotid and Vertebral Artery Disease: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, and the American Stroke Association, American Association of Neuroscience Nurses, American Association of Neurological Surgeons, American College of Radiology, American Society of Neuroradiology, Congress of Neurological Surgeons, Society of Atherosclerosis Imaging and Prevention, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of NeuroInterventional Surgery, Society for Vascular Medicine, and Society for Vascular Surgery
- 2011 ASA/ACCF/AHA/AANN/AANS/ACR/ASNR/CNS/SAIP/SCAI/SIR/SNIS/SVM/SVS Guideline on the Management of Patients With Extracranial Carotid and Vertebral Artery Disease: Executive Summary: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, and the American Stroke Association, American Association of Neuroscience Nurses, American Association of Neurological Surgeons, American College of Radiology, American Society of Neuroradiology, Congress of Neurological Surgeons, Society of Atherosclerosis Imaging and Prevention, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of NeuroInterventional Surgery, Society for Vascular Medicine, and Society for Vascular Surgery
- 2011 ASA/ACCF/AHA/AANN/AANS/ACR/ASNR/CNS/SAIP/SCAI/SIR/SNIS/SVM/SVS Guideline on the Management of Patients With Extracranial Carotid and Vertebral Artery Disease: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, and the American Stroke Association, American Association of Neuroscience Nurses, American Association of Neurological Surgeons, American College of Radiology, American Society of Neuroradiology, Congress of Neurological Surgeons, Society of Atherosclerosis Imaging and Prevention, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of NeuroInterventional Surgery, Society for Vascular Medicine, and Society for Vascular Surgery
- 2011 ASA/ACCF/AHA/AANN/AANS/ACR/ASNR/CNS/SAIP/SCAI/SIR/SNIS/SVM/SVS guideline on the management of patients with extracranial carotid and vertebral artery disease: executive summary: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the American Stroke Association, American Association of Neuroscience Nurses, American Association of Neurological Surgeons, American College of Radiology, American Society of Neuroradiology, Congress of Neurological Surgeons, Society of Atherosclerosis Imaging and Prevention, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of NeuroInterventional Surgery, Society for Vascular Medicine and Society for Vascular Surgery Developed in collaboration with the American Academy of Neurology and Society of Cardiovascular Computed Tomography
- 2011 ASA/ACCF/AHA/AANN/AANS/ACR/ASNR/CNS/SAIP/SCAI/SIR/SNIS/SVM/SVS Guideline on the Management of Patients With Extracranial Carotid and Vertebral Artery Disease: Executive Summary: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, and the American Stroke Association, American Association of Neuroscience Nurses, American Association of Neurological Surgeons, American College of Radiology, American Society of Neuroradiology, Congress of Neurological Surgeons, Society of Atherosclerosis Imaging and Prevention, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of NeuroInterventional Surgery, Society for Vascular Medicine, and Society for Vascular Surgery Developed in Collaboration With the American Academy of Neurology and Society of Cardiovascular Computed Tomography
- 2011 ASA/ACCF/AHA/AANN/AANS/ACR/ASNR/CNS/SAIP/SCAI/SIR/SNIS/SVM/SVS Guideline on the Management of Patients With Extracranial Carotid and Vertebral Artery Disease: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, and the American Stroke Association, American Association of Neuroscience Nurses, American Association of Neurological Surgeons, American College of Radiology, American Society of Neuroradiology, Congress of Neurological Surgeons, Society of Atherosclerosis Imaging and Prevention, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of NeuroInterventional Surgery, Society for Vascular Medicine, and Society for Vascular Surgery Developed in Collaboration With the American Academy of Neurology and Society of Cardiovascular Computed Tomography
- Change in Cerebral Perfusion after Carotid Angioplasty with Stenting Is Related to Cerebral Vasoreactivity: A Study Using Dynamic Susceptibility-Weighted Contrast-Enhanced MR Imaging and Functional MR Imaging with a Breath-Holding Paradigm
- Intracranial hemorrhage and hyperperfusion syndrome following carotid artery stenting: Risk factors, prevention, and treatment
- Intracerebral Hemorrhages Associated With Neurointerventional Procedures Using a Combination of Antithrombotic Agents Including Abciximab
- Hyperperfusion-induced intracerebral hemorrhage after carotid stenting documented by TCD