
Abstract
Summary: Perfusion CT studies of regional cerebral blood flow (rCBF), involving sequential acquisition of cerebral CT sections during IV contrast material administration, have classically been reported to be achieved at 120 kVp. We hypothesized that using 80 kVp should result in the same image quality while significantly lowering the patient's radiation dose, and we evaluated this assumption.
In five patients undergoing cerebral CT survey, one section level was imaged at 120 kVp and 80 kVp, before and after IV administration of iodinated contrast material. These four cerebral CT sections obtained in each patient were analyzed with special interest to contrast, noise, and radiation dose.
Contrast enhancement at 80 kVp is significantly increased (P < .001), as well as contrast between gray matter and white matter after contrast enhancement (P < .001). Mean noise at 80 kVp is not statistically different (P = .042). Finally, performance of perfusion CT studies at 80 kVp, keeping mAs constant, lowers the radiation dose by a factor of 2.8.
We, thus, conclude that 80 kVp acquisition of perfusion CT studies of rCBF will result in increased contrast enhancement and should improve rCBF analysis, with a reduced patient's irradiation.
Perfusion CT performed for the evaluation of regional cerebral blood flow (rCBF) involves sequential acquisition of cerebral CT sections obtained in axial mode during IV administration of iodinated contrast material. Clinical use of such a technology in the setting of cerebrovascular diseases has classically been reported to be performed at 120 kVp (1–3).
Another method used to measure rCBF is stable xenon CT (Xe-CT), relating to dynamic CT realized during inhalation of gaseous stable xenon (4). In 1978, Kelcz (5) carried out experimental studies that demonstrated that the optimal kVp to perform stable Xe-CT ranges at about 80. However, stable xenon has an atomic number of 54 and a K-edge of 34.6 keV, very close to those of iodine, which are respectively 53 and 33.2 keV. We therefore evaluated the use of an 80-kVp tension to perform perfusion CT studies.
Method
Five patients who underwent cerebral CT examinations (Lightspeed CT; General Electric, Milwaukee, WI) before and after IV administration of iodinated contrast material were selected. CT revealed three normal examinations, one case of agenesis of the corpus callosum, and one case of Alzeihmer's dementia. After the native cerebral CT examination, one section level through the basal nuclei was selected and imaged at 120 kVp (number 1) and 80 kVp (number 2). After IV administration of 70 cc of iodinated contrast material at 1 cc/s (over a 70-s interval), a contrast-enhanced cerebral CT was achieved over 30 seconds. At the end of the injected series, sections at the previously selected level were acquired successively at 120 kVp (number 3) then at 80 kVp (number 4), in a 5-second interval, this delay being short and not significant with respect to the elimination kinetics of the iodinated contrast material. The four additional sections, before (numbers 1–2) and after (numbers 3–4) IV administration of contrast material, were performed at 200 mAs, with a field of view of 25 cm. This study protocol was approved by our institutional review board. Informed consent was obtained from each patient prior to performance of the four additional CT sections.
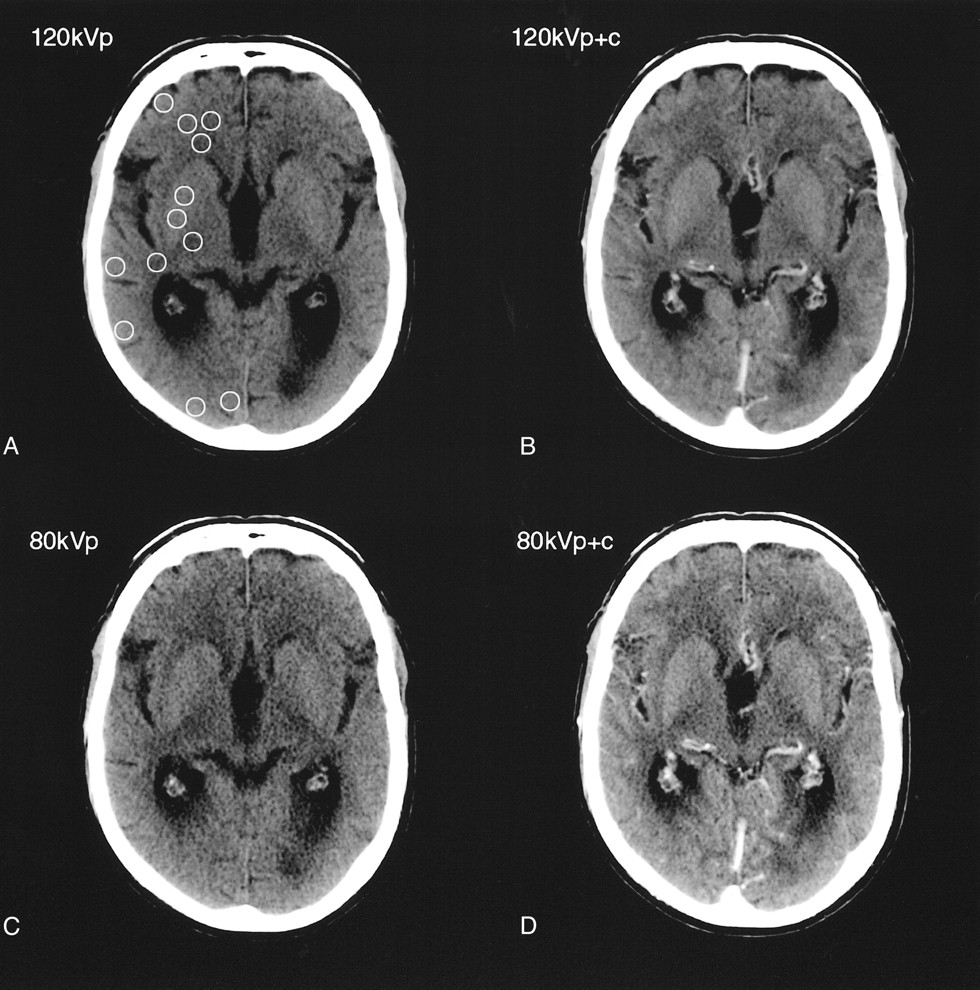
For each of our five patients, we had four cerebral CT sections: native 80 kVp (number 2, Fig 1C) and 120 kVp (number 1, Fig 1A), and 80 kVp (number 4, Fig 1D) and 120 kVp (number 3, Fig 1B) after contrast enhancement. These four cerebral CT sections were analyzed with special interest to contrast, noise, and radiation dose.

Four cerebral CT sections through the basal nuclei obtained at 200 mAs and at 80 kVp (C, D) and 120 kVp (A, B), before (A, C) and after (B, D) IV administration of iodinated contrast material (C, 80 kVp [number 2], A, 120 kVp [number 1], D, 80 kVp + C [number 4], B, 120 kVp + C [number 3]). ROIs were drawn on cortical gray matter, basal nuclei gray matter, and white matter. Typical ROIs chosen for measurements are shown on A. The four sections are displayed with the same window settings (window level: 40 HU, and window width: 80 HU). At 80 kVp, the contrast enhancement is increased, as well as the gray matter-white matter contrast. The signal-to-noise ratio is not significantly altered
We determined the respective values of contrast enhancement, as well as of gray matter-white matter contrast (mean CT number in regions of interest [ROIs] drawn on gray matter divided by mean CT number in ROIs drawn on white matter in the corresponding issue), in ROIs of about 100 pixels, as they related to the typical size of the spatial filtering used in perfusion CT data processing. The ROIs were drawn on cortical gray matter (10 ROIs for each patient), basal nuclei gray matter (five ROIs for each patient), and white matter (10 ROIs for each patient). The same ROIs were chosen on the four sections (Fig 1). Statistical analysis (unilateral t tests for matched variables) was performed for the data related to the various ROIs. On the same images and with the same statistical tests, we analyzed noise related to the standard deviation of CT density in a uniform area chosen in the background, at 80 and 120 kVp, respectively.
The radiation dose for perfusion CT involving 25 successive CT sections obtained in an axial mode at 200 mAs was evaluated for 80 and 120 kVp on the Lightspeed CT unit. This evaluation was achieved through experimental studies on a test phantom in conformity with Food and Drug Administration (FDA) rules, related to a polymethylmetacrylate cylinder of 16-cm diameter (Code of Federal Regulations, 21 CFR Ch. 1, §1020.3, FDA, Washington DC, 1992). Calculation of normalized and weighted CT dose index (nCTDIw) and cerebral effective dose was performed according to European Guidelines on Quality Criteria for Computed Tomography (6), which are very close to those recommended by the FDA. The brain-absorbed dose was deduced from the nCTDIw (7).
Results
Contrast enhancement and gray matter-white matter contrast observed at 80 and 120 kVp, respectively, are summarized in the Table, which describes numerical averages and standard deviations of ROI values in the corresponding issue. Contrast enhancement at 80 kVp is significantly increased for cortical gray matter (P < .001), basal nuclei gray matter (P < .001), and white matter (P < .001). Contrast between gray matter and white matter before contrast material administration is increased at 80 kVp, but not significantly (P = 0.06). On the other hand, contrast between gray matter and white matter after contrast enhancement is significantly increased (P < .001).
Contrast enhancement and gray matter-white matter contrast at 80 and 120 kVp (numeric average ± standard deviation)
Mean noise was 6.6 HU ± 3.9 HU at 80 kVp and 5.3 HU ± 2.6 HU at 120 kVp, a statistically insignificant difference (P = .042).
Considering acquisition of two adjacent 10-mm sections, available thanks to the multidetector-array technology, the measured nCTDIw is 0.090 mGy/mAs at 80 kVp and 0.249 mGy/mAs at 120 kVp. Supposing a perfusion CT protocol of 25 successive slices obtained in axial mode at 200 mAs and with regard to the geometry of radiation delivery on the Lightspeed CT unit (dose efficiency of 65%), the resultant radiation dose is 291 mGy at 80 kVp and 806 mGy at 120 kVp. Regarding the stochastic effect of radiation, these calculated doses must be redistributed on the whole cerebral volume. Because a 20-mm thickness relates approximatively to a 10th of the cerebral volume, the brain absorbed dose at 80 kVp is 29 mGy. Considering a weighting factor of 0.0021 mSv/(mGy x cm) for the brain, the cerebral effective dose is 1.218 mSv, which is inferior to the reference dose level for a standard cerebral CT examination (2.5 mSv) (6).
Discussion
It was impossible to perform successive 120- and 80-kVp perfusion CT studies in human patients for evident ethical and technical reasons. The radiation dose required and the time delay necessary to eliminate contrast between two studies would have been excessive. However, we demonstrated on static cerebral CT sections that using 80 kVp significantly improves steady-state contrast enhancement. It seems reasonable to infer that it will also increase dynamic contrast enhancement obtained during IV administration of iodinated contrast material. Because measurement of rCBF in perfusion CT studies precisely results from dynamic contrast enhancement analysis, acquisition of sequential cerebral CT sections at 80 kVp will facilitate data processing.
Furthermore, contrast between gray matter and white matter at 80 kVp is increased after contrast material administration, which constitutes an additional benefit. This increase of gray matter-white matter contrast after contrast enhancement at 80 kVp results from the more important perfusion of gray matter compared with that of white matter. Moreover, after contrast enhancement, X-ray interaction with soft tissues at 80 kVp relates to the photoelectric effect due to the 33 keV K-edge of the iodine included in the contrast material. On the other hand, X-ray interaction before contrast material administration is mainly due to the Compton effect, and then contrast between gray matter and white matter is not modified at 80 kVp.
Using 80 kVp involves a lower photon flux, but does not result in a statistically significant increase in noise, allowing 80 kVp images to be used in perfusion CT analysis.
Finally, performance of perfusion CT examination at 80 kVp, keeping mAs constant, lowers the radiation dose by a factor 2.8.
Conclusion
Perfusion CT studies of rCBF achieved at 80 kVp will result in increased contrast enhancement and should improve rCBF analysis, with a reduced patient's irradiation. We thus propose to perform perfusion CT studies of rCBF at 80 kVp.
- Received February 16, 2000.
- Copyright © American Society of Neuroradiology
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Comparison of three commonly used CT perfusion software packages in patients with acute ischemic stroke
- Automated CT perfusion imaging for acute ischemic stroke: Pearls and pitfalls for real-world use
- Whole-Brain Adaptive 70-kVp Perfusion Imaging with Variable and Extended Sampling Improves Quality and Consistency While Reducing Dose
- Can Iterative Reconstruction Improve Imaging Quality for Lower Radiation CT Perfusion? Initial Experience
- Pre-intervention cerebral blood volume predicts outcomes in patients undergoing endovascular therapy for acute ischemic stroke
- Comparison of Conventional CTA and Volume Perfusion CTA in Evaluation of Cerebral Arterial Vasculature in Acute Stroke
- Differences in CT Perfusion Summary Maps for Patients with Acute Ischemic Stroke Generated by 2 Software Packages
- Effect of Stenting on Cerebral CT Perfusion in Symptomatic and Asymptomatic Patients with Carotid Artery Stenosis
- CT Perfusion in Acute Ischemic Stroke: A Comparison of 2-Second and 1-Second Temporal Resolution
- Effect of Tube Voltage on Image Quality in 64-Section Multidetector 3D CT Angiography: Evaluation with a Vascular Phantom with Superimposed Bone Skull Structures
- FDA Investigates the Safety of Brain Perfusion CT
- Recommendations for Imaging of Acute Ischemic Stroke: A Scientific Statement From the American Heart Association
- Theoretic Basis and Technical Implementations of CT Perfusion in Acute Ischemic Stroke, Part 2: Technical Implementations
- A quantitative method for estimating hepatic blood flow using a dual-input single-compartment model
- Reproducibility of Quantitative CT Brain Perfusion Measurements in Patients with Symptomatic Unilateral Carotid Artery Stenosis
- Comparative Overview of Brain Perfusion Imaging Techniques
- Quantitative measurement of hepatic portal perfusion by multidetector row CT with compensation for respiratory misregistration
- Perfusion CT: a worthwhile enhancement?
- Guidelines and Recommendations for Perfusion Imaging in Cerebral Ischemia: A Scientific Statement for Healthcare Professionals by the Writing Group on Perfusion Imaging, From the Council on Cardiovascular Radiology of the American Heart Association
- Comparison of Admission Perfusion Computed Tomography and Qualitative Diffusion- and Perfusion-Weighted Magnetic Resonance Imaging in Acute Stroke Patients
- Simultaneous Measurement of Regional Cerebral Blood Flow by Perfusion CT and Stable Xenon CT: A Validation Study