
Abstract
BACKGROUND AND PURPOSE: Percutaneous vertebroplasty is an effective tool for the relief of pain caused by osteoporotic spine fractures. Our purpose is to evaluate this technique and its effectiveness in restoring the height of such fractures.
METHODS: Forty osteoporotic vertebral body fractures in 30 consecutive patients (24 female, six males; mean age, 70 years) were analyzed retrospectively, before and after percutaneous vertebroplasty, for changes in vertebral body height, kyphosis angle, and wedge angle. The ages of the fractures range from 1 to 5 months.
RESULTS: Percutaneous vertebroplasty improved the pretreatment height of compression fractures in these patients by a mean of 47.6% (P < .001), with only 15% showing no improvement. These figures compare favorably with published results for kyphoplasty (47% mean improvement in height in 70% of fractures; no improvement in 30% of fractures). In addition, we achieved a mean improvement in kyphosis angle of 6° and an improvement in the wedge angle of 3.5° (as compared with published results for kyphoplasty of 7.4 and 4.3°, respectively; P < .001).
CONCLUSION: Percutaneous vertebroplasty should be viewed not only as a pain-relieving procedure, but also an effective method for improving vertebral body height, kyphosis angle, and wedge angle.
Percutaneous vertebroplasty is a recognized technique for the stabilization of benign or malignant vertebral body fractures and the improvement and palliation of resulting pain (1–6). Kyphoplasty is an alternative method for such stabilization and, in addition, has been touted as a method to improve the height of vertebral body fractures (7–10). Lieberman et al (7) published their results with kyphoplasty, and in 70% of individuals treated kyphoplasty restored 47% of the lost height from fractures. In 30% of patients, however, no height restoration was noted. This study was undertaken to evaluate percutaneous vertebroplasty in the restoration of vertebral body height secondary to osteoporotic compression fracture and compare this technique with kyphoplasty (7).
Methods
Patients
Forty osteoporotic fractures in 30 consecutive patients, treated over a 1.5-year period with percutaneous vertebroplasty were analyzed, pre- and postprocedure, for height restoration. This group consisted of 24 female patients and six male patients, with a mean age of 70 years and an age range of 40–90 years. The mean age for the male group was 69 years (range, 46–90 years), and the female group had a mean age of 70 years (range, 54–88 years).
Twenty-two thoracic (17 patients) and 18 lumbar levels (16 patients) were treated. Three patients had both thoracic and lumber levels treated. The age of the fractures ranged from 1 to 5 months, with all but three patients having fractures of 2 months or older.
Procedure
Most levels were treated with a bitranspedicular route, by using 11-gauge bone biopsy needles (Cook Inc., Bloomington, IL) for the lumbar levels and 13-gauge needles for the thoracic levels. Three quarters (30 g) of a standard mixture of polymethylmethacrylate (PMMA), bone cement, was mixed with a 20-mL ampule of liquid polymer (Surgical Simplex P, Stryker Howmedica Osteonics, Mahwah, NJ). To improve visualization of the injected cement, 5 g of barium sulfate tracer (Parallax Medical Inc., Scotts Valley, CA) and 1 g of tungsten powder (Balt, Montmorency, France) were added. The total volume of the subsequent PMMA mixture injected at each level ranged from 2 to 8 mL. All but one of procedures (general anesthesia) were accomplished by using local anesthesia (1% lidocaine, Abbott Labs, Abbott Park, IL) and intravenous sedation (1-mg doses of Midaphan, Ben Venne Labs, Bedford, OH; and 50-μg doses of Fentanyl citrate; Abbott Labs). Biplanar fluoroscopy was used in all cases (Siemens Neurostar, Siemens Medical Systems, Munich, Germany). Either 1 g of intravenous Cefazolin (Eli Lilly & Company, Indianapolis, IN) or 1.2 g Tobramycin (Glaxo Smith Kline, Research Triangle Park, NC) combined with the PMMA mixture was used for antibiotic coverage.
Height Restoration Analysis
All measurements were undertaken by one of the authors (A.B.D.). Percutaneous vertebroplasties in the series were performed jointly by two authors (A.B.D. and J.H.). Each of the physicians had an average experience of 2 years for percutaneous vertebroplasty. The midbody of the fracture was measured for height and compared with one adjacent vertebral body, determined to be of “normal height.” Measurements were made pre- and postvertebroplasty. To correct for any differences in magnification during the fluoroscopic procedure—all images were taken with the patient prone—the height of the fractured body was expressed as a percentage of the “normal” vertebral body. For comparison to kyphoplasty, height restoration, as defined by Lieberman et al (7), equals the amount of improvement midbody before and after procedure divided by the original loss of height as calculated by the single adjacent normal vertebral body height. In addition, the kyphosis angle and wedge angle were calculated, pre- and postvertebroplasty, by using the methods described by Teng et al (Fig 1) (11).

Diagrammatic representation of lateral views of the spine and spinal fracture, pre- and post-vertebroplasty, are represented (1 indicates height of the control “normal” vertebral body; 2, height of the vertebral body pre- and postvertebroplasty; 3, kyphosis angle as according to the method of Cobb, as described by Teng et al [11]; 4, wedge angle as described by Teng et al [11]).
Statistical Analysis
To evaluate the significance of the data set obtained, the single-tail Student t test (Excel, Microsoft Corporation, Redmond, WA) and the Wilcoxon paired difference signed rank test were used (12). A P value < .05 for both statistical tests would be considered significant.
Results
Percutaneous vertebroplasty, in our series, improved the pretreatment height of compression fractures (40 fractures in 30 patients) by a mean of 47.6%, a median of 38%, and a range of 0–100%, as defined by the formula above (Fig 1), with only 15% showing no height improvement from this technique. There was a mean improvement in wedge angle and kyphosis angle of 3.5° and 5°, respectively. Both the single-tail Student t test and the Wilcoxon paired difference signed rank test yielded a P value < .001 for all of these measurements, which indicates the statistical significance of these results.
Discussion
Percutaneous vertebroplasty is an established technique for the alleviation of pain from fractures of various etiologies (1–5). Only a few reports, however, have mentioned the possible benefit of vertebroplasty in vertebral body height improvement (11, 13, 14). The latter factor may have been overlooked, because many elderly osteoporotic patients, in our experience, are not necessarily concerned with the restoration of a normal lordosis of the lumbar spine or the reduction of a kyphosis of the thoracic spine but are more focused on pain and medication reduction.
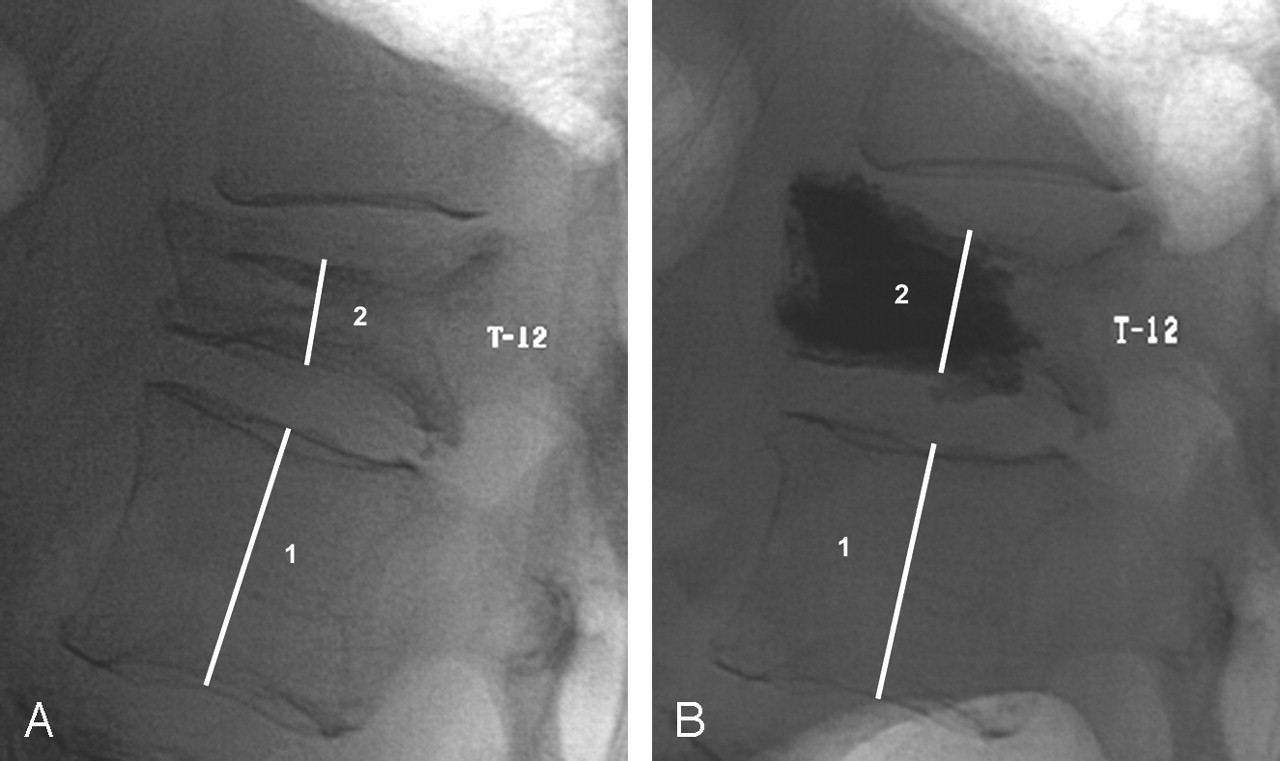
The mechanism of restoration of height during vertebroplasty is probably due to two factors. First, it is a well-known phenomenon in the orthopedic literature to experience improvement of fracture height simply by placing the patient prone, before instrumentation and stabilization (15). In addition, a recent article by McKiernan et al (14) demonstrated the dynamic mobility of vertebral compression fractures in 44% of individuals undergoing vertebroplasty, from upright to supine position. Second, the pressure and volume of PMMA injected helps preserve fortuitous positional changes and may further restore fracture height. In addition, some fractures associated with unstable fluid-filled cavities that may expand and fill with bone cement. The latter is probably the major mechanism of height restoration in the case illustrated by Figure 2 (11, 15, 16). Teng et al (11) also suggested the effects of height restoration were most marked in fractures containing gas.

Height improvement with prone positioning and vertebroplasty.
A, Prevertebroplasty, T-12 osteoporotic fracture, with subtle anterior vertebral body cystic cavity, prone position, lateral (1). Midvertebral height of the fracture is compared with the adjacent normal appearing vertebral body height (2).
B, Postpercutaneous vertebroplasty, prone, lateral, with improvement in height. The improvement in height by using the method of Leiberman et al, is approximately 30%. The improvements of the wedge angle and kyphosis angle, by using the method of Teng et al are eight and 7°, respectively.
Ex vivo biomechanical kyphoplasty studies have shown significant restoration (97%) of vertebral body height lost after compression fracture in 16 cadaver specimens with experimentally created vertebral body fractures (8). The same study produced less-effective height restoration with simple vertebroplasty (30%). In clinical practice, however, kyphoplasty has demonstrated less-impressive results, with several publications suggesting mean restoration of height ranging from 47% to 66%, depending on the population studied and the method of measurement (7, 9–10). The differences may be due to biomechanics that favor kyphoplasty in an isolated cadaver model and favor vertebroplasty in clinical practice (e.g., ligamentous influences, adjacent vertebral level factors, weight distribution, and so forth).
Hiwatashi et al (13) used a different calculation technique of absolute height change, measured in millimeters, rather than percentages, although this technique does not take into account size difference between patients, while the percentage calculation technique corrects for such size variations.
What may be of greater interest, however, is the percentage of improvement of fractures from the baseline. Thus, an improvement of 5–100%, or 95–100%, pre- and posttreatment, by using Lieberman’s method of measurement, would be 100% restoration in either case, although the change from 5% to 100% is certainly the more impressive of the two figures. Using a different method of calculation (posttreatment percentage of normal minus pretreatment percentage of normal divided by posttreatment percentage of normal), the theoretical case 1 (improvement of 5–100%) yields an improvement of 95%, whereas the theoretical case 2 as described above yields an improvement of only 5%. Using this latter method of calculation, the mean improvement of our series is 17.6% ± 35% (1 SD), with 11 cases (27.5%) achieving complete restoration of estimated normal height. By using a similar measurement for the midvertebral body, Teng et al (11) suggest 14% improvement in midbody height by percutaneous vertebroplasty. A similar analysis for kyphoplasty cannot be deduced from the published data, but such a study might form the basis of a prospective study between the two techniques.
If the degree of height restoration is comparable between kyphoplasty and vertebroplasty, as our data suggest, then there is little to support the use of kyphoplasty, particularly as charges, at least at our institution, are approximately 10-fold for the latter, predominantly related to the materials, costs, and use of general anesthesia (3). Further, general anesthesia is usually required for kyphoplasty, but not vertebroplasty (3).
The limitations of this study include different volumes of cement injected, injection pressures (hand injection in all cases in our study), and the further comparison of kyphoplasty to the new method of calculation described above. The presence of clefts or cysts may also impact the final results, suggested by Teng et al (11), although the prediction of clefts or cysts may be difficult to recognize with conventional radiographs only, without additional CT or MR imaging. In addition, a double versus single transpedical approach might have some impact on the height restoration. One of the major questions that might be asked is whether height restoration plays any significant role in alleviation of pain. Finally, as emphasized by Kallmes and Jensen (6), there may be some placebo effect with percutaneous vertebroplasty may be present. A blinded examination of protocol may be of further benefit.
Although restoration of height may be desirable and important with severe thoracic kyphosis, to prevent respiratory compromise and skin ulceration, our experience suggests that most patients are much more desirous of pain relief than kyphotic curvature improvement. Further, many of the individuals with kyphosis suffer from a mixture of old as well as new fractures, and the former are not suitable for either kyphoplasty or vertebroplasty.
Finally, as a technical note, we currently use only intravenous antibiotics for the vertebroplasty procedure. We continue to add small amounts of tungsten to the cement mixture, because this combination improves the visualization of the cement and allows early detection of unwanted venous or epidural leakage of the cement contents.
Conclusion
Percutaneous vertebroplasty offers equivalent height restoration as compared with kyphoplasty. Further evaluation of both techniques with standardized measurements other than Lieberman et al (7, as described above, may shed additional light on differences between the two therapies. Finally, we achieved similar but slightly lower mean improvement in wedge angle and kyphosis angle as compared with Teng et al (11).
References
- Received March 1, 2004.
- Accepted after revision April 27, 2004.
- Copyright © American Society of Neuroradiology
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- In Not Only Vertebroplasty but Also Kyphoplasty, the Resolution of Vertebral Deformities Depends on Vertebral Mobility
- Significance of Dynamic Mobility in Restoring Vertebral Body Height in Vertebroplasty
- Vertebral Augmentation for Compression Fractures Caused by Malignant Disease
- Kyphoplasty and Vertebroplasty Produce the Same Degree of Height Restoration