
Spontaneous intracranial hypotension is caused by a spinal CSF leak. Currently, various classification schemes for CSF leaks exist, with 1 system dividing leaks into ventral dural tears (type 1a), lateral/posterior dural tears (type 1b), leaks from meningeal diverticula (type 2), and CSF-venous fistulas (type 3).1 Farb et al2 subsequently classified these leaks in a similar fashion. Ventral and lateral dural tears essentially always result in extradural CSF collections that can be detected on spine MR imaging or CT myelography.3 These are usually intraspinal epidural collections, though CSF can extend through the foramina in some instances. Leaks from meningeal diverticula, in contrast, usually result in only paraspinal CSF accumulation (Fig 1A), though intraspinal extradural CSF can rarely be seen. CSF-venous fistulas essentially never have associated extradural CSF.

Lateral CSF leaks in 3 patients (A, Leaking meningeal diverticulum. B and C, Lateral dural tears with herniated arachnoid diverticula). In the first patient, 30-minute delayed left lateral decubitus CT myelography (CTM) shows paraspinal contrast accumulation at L2 (A, solid arrow) adjacent to a small meningeal diverticulum (A, dashed arrow), compatible with a leaking diverticulum. In the second patient, a coronal image from decubitus photon-counting CTM (B) shows a left T12 lateral dural tear with an arachnoid diverticulum herniating through the dural defect (B, solid arrow) and separate extradural contrast accumulation (B, dashed arrows). In the third patient, axial image from a decubitus photon-counting CTM (C) shows a right T11 lateral dural tear, again with an arachnoid diverticulum herniating through the dural tear (C, solid arrow) and separately leaking extradural contrast (C, dashed arrow). In this case, the precise site of the dural defect was clearly seen (C, arrowhead).
Although these different types of CSF leaks are generally well-understood, lateral dural tears can be difficult to discriminate from leaking meningeal diverticula. Lateral dural tears most commonly occur along the axilla of nerve root sleeves, but they also less frequently occur at the nerve root sleeve shoulders or at the level of the pedicle.3 They are commonly, though not always, associated with an arachnoid diverticulum that herniates or billows through the dural defect (Fig 1B, -C). This herniated diverticulum involves only the arachnoid and therefore differs from the typical perineural meningeal diverticula, which are lined by the dura and arachnoid. The cause of arachnoid herniation from lateral dural tears is unclear, but it is possible that the more capacious lateral epidural space (compared with the ventral epidural space) and lack of penetrating osseous spicules causing lateral leaks play a role. Most important, the arachnoid diverticulum is a secondary manifestation of the lateral dural tear and not the source of CSF leak. Rather, CSF usually leaks from the margins of the lateral dural tear.3 On decubitus DSA or CT myelography, contrast opacification of this diverticulum is usually seen concurrently with epidural contrast leakage.4 The dural defect itself is usually not seen. Thus, lateral dural tears may falsely appear to represent a “ruptured” or “leaking” meningeal diverticulum on myelography. Many lateral dural tears are likely inadvertently diagnosed as leaks from meningeal diverticula, because both result in a lateral leak and harbor a diverticulum at the site of the leak.
High-resolution modalities such photon-counting CT may sometimes reveal the precise site of lateral dural tears, clarifying the diagnosis (Fig 1C). Often, surgical exploration is the only way to visualize the actual dural tear (Fig 2). Further study with surgical correlation will be necessary to determine how frequently lateral leaks diagnosed on myelography represent lateral dural tears with secondarily herniated arachnoid diverticula versus primarily leaking meningeal diverticula. Although 1 initial study on this topic suggested that leaks from meningeal diverticula were common (up to 42% of CSF leaks), this was before the routine use of decubitus myelography to diagnose CSF-venous fistulas and lateral dural tears.1 We suspect that lateral dural tears and CSF-venous fistulas are far more common than initially believed.

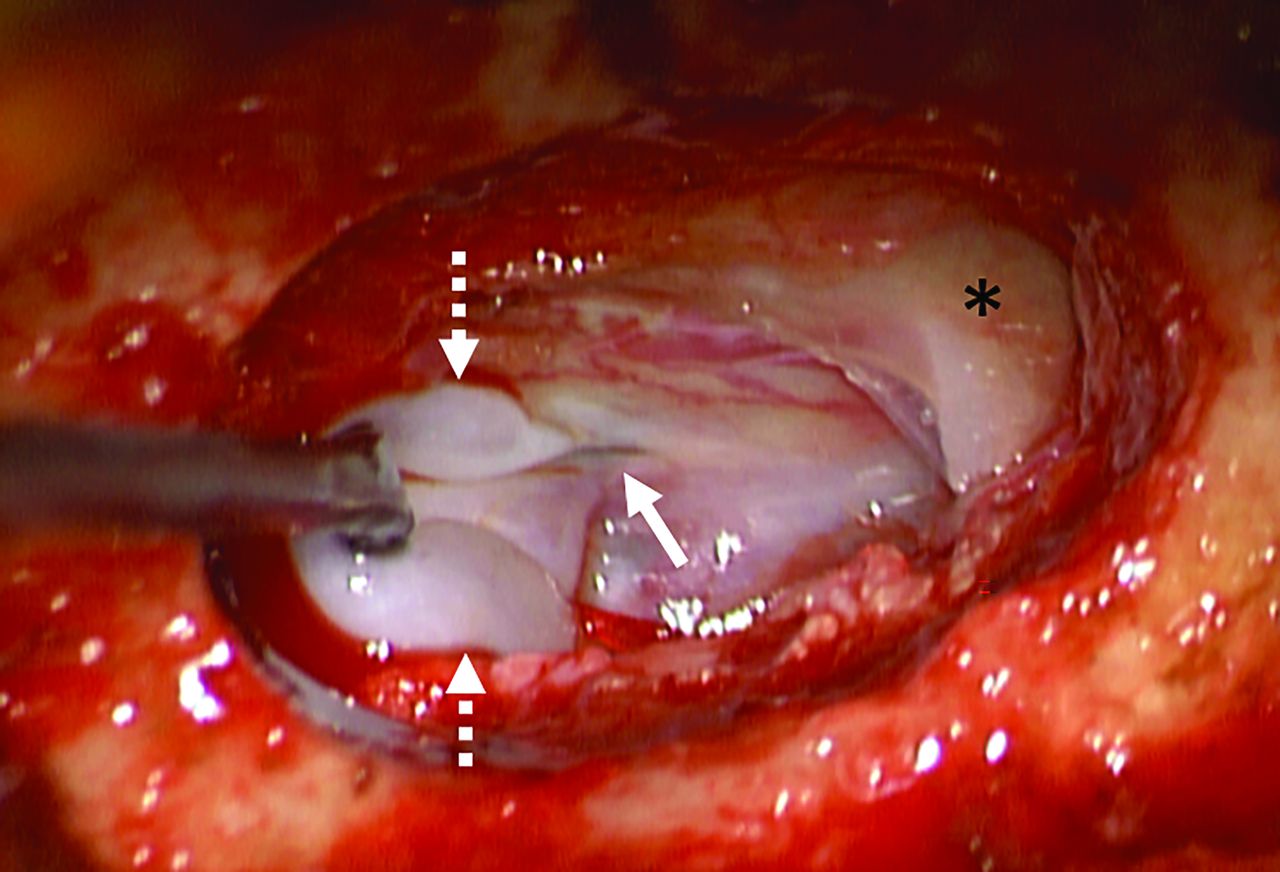
Intraoperative photograph demonstrating the typical appearance of a lateral dural tear inferior to the nerve root sleeve (asterisk). A dural tear (solid arrow) is seen with a thin arachnoid diverticulum (dashed arrows) herniating or “billowing” out from the defect. The actual site of CSF leak was from the edges of the dural tear itself (solid arrow) rather than the diverticulum.
The distinction between lateral dural tears and leaks from meningeal diverticula is important for 2 reasons: First, accurate epidemiologic data about these leaks are needed to understand their pathophysiology; second, it is important to determine how these different leak types respond to treatment, such as blood patching or surgery. To conclude, we encourage close attention to the distinction between lateral dural tears associated with herniated arachnoid diverticula versus leaking meningeal diverticula. While these 2 leak types share some similarities on myelography, lateral dural tears are generally more common and essentially always associated with intraspinal extradural CSF collections. Leaking diverticula, by contrast, are relatively uncommon and usually cause paraspinal CSF accumulation rather than intraspinal extradural collections. Further study with radiographic and surgical correlation will be helpful to corroborate these suppositions.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
- © 2024 by American Journal of Neuroradiology




{kind=link}
{kind=link}
Related Articles
Cited By...
- Advanced Imaging of Type 2 Spinal CSF Leaks with Ultra-High-Resolution Conebeam CT Myelography
- Additional Diagnostic Value of Conebeam CT Myelography Performed after Digital Subtraction Myelography for Detecting CSF-Venous Fistulas
- Spontaneous Intracranial Hypotension in Children: A Multi-Institutional Review of Spinal CSF Leaks Localized on Advanced Myelography
- Spinal CSF Leaks: The Neuroradiologist Transforming Care