Abstract
SUMMARY: This study aimed to assess the utility of DTI in the detection of olfactory bulb dysfunction in COVID-19-related anosmia. It was performed in 62 patients with COVID-19-related anosmia and 23 controls. The mean diffusivity and fractional anisotropy were calculated by 2 readers. The difference between the fractional anisotropy and mean diffusivity values of anosmic and control olfactory bulbs was statistically significant (P = .001). The threshold of fractional anisotropy and mean diffusivity to differentiate a diseased from normal olfactory bulb were 0.22 and 1.5, with sensitivities of 84.4% and 96.8%, respectively, and a specificity of 100%.
ABBREVIATIONS:
- COVID-19
- coronavirus disease 2019
- FA
- fractional anisotropy
- MD
- mean diffusivity
- OB
- olfactory bulb
- SARS-COV-2
- Severe Acute Respiratory Syndrome coronavirus 2
In coronavirus disease 2019 (COVID-19), morbidity and mortality are primarily attributed to pulmonary causes. However, there is a substantial body of literature reporting a broad range of neurologic manifestations, including stroke, dural sinus thrombosis, cerebral microhemorrhage, acute necrotizing encephalopathy, and olfactory and gustatory dysfunction.1-3
Olfactory dysfunction was underestimated early in the COVID-19 pandemic. Nevertheless, in a study including 1480 patients, anosmia was demonstrated in 68% of patients. Anosmia persisted in 26% of them even after testing negative for Severe Acute Respiratory Syndrome coronavirus 2 (SARS-COV-2).4 The reported incidence of anosmia varied internationally: as low as 30% in South Korea, and as high as 88% in Europe. The olfactory bulb (OB) is considered an immunologic organ that shields the CNS from viral infection, so its involvement could risk the CNS being subjected to infection. Consequently, the early detection of OB involvement in case of COVID-19 infection is very important.5,6
MR imaging can provide anatomic data about the olfactory pathway. One of the primary parameters to evaluate the olfactory pathway is the measurement of OB volume. However, the volume measurements are not routinely used to assess the olfactory pathway because they are more difficult and time-consuming than visual analysis. Moreover, it is not easy to measure these thin structures with great variations, even among healthy individuals, making its efficiency as a diagnostic tool limited.7-9
DTI is a noninvasive technique that is increasingly implemented. The 2 main parameters extracted from DTI are mean diffusivity (MD) and fractional anisotropy (FA). MD demonstrates the degree of diffusion restriction of water molecules, while FA reflects the degree of the tissue anisotropy.10 DTI of the OB has been performed in some diseases, such as OB gliomas and paranasal sinus diseases.11-13 However, to our knowledge, the validity of DTI in the evaluation of OB neuropathy has been scarcely studied in COVID-19-related anosmia. The aim of the current study was to assess the validity of DTI in the diagnosis of OB dysfunction in COVID-19-related anosmia.
MATERIALS AND METHODS
Subjects
This prospective case-control observational study was approved by the institutional review board. Informed consent was acquired from all patients and controls. The study was conducted on 62 consecutive patients with COVID-19-related anosmia and 23 age- and sex-matched healthy controls. The olfaction in both groups was assessed by the Smell Diskettes olfaction test.14 All patients were anosmic with a score of zero on the Smell Diskettes olfaction test with the polymerase chain reaction test positivity confirming COVID-19 infection. Control group consisted of individuals who had negative polymerase chain reaction test results for COVID-19, showed no signs of anosmia (scores of 6–9 on the Smell Diskettes olfaction test), no history or prior imaging studies of sinus disease, and no prior neurologic insult nor previous operations.
MR Imaging Protocol
All scans were performed using a 1.5T MR imaging unit (Ingenia; Philips Healthcare). All patients with symptoms of anosmia were scanned using a coronal 3D-FLAIR sequence with the following parameters: TR/TE = 8000/133 ms; bandwidth = 120 Hz/pixel; TSE factor = 80; section thickness = 2mm; interslice gap = 0.5mm; FOV = 230 × 230 × 20 mm2 (from the nose tip anteriorly to the posterior sphenoidal sinus wall, from the skull vault to the hard palate); voxel size = 0.95 × 0.95 × 2 mm; matrix = 240 × 240; echo-train length = 220 with variable flip angles; time of acquisition = 270 seconds. DTI was performed using a single-shot echo-planar sequence with TR/TE = 3200/90 ms. Diffusion gradients were obtained along 32 axes using b-values of 0 and 1000 s/mm2. We used the following scanning parameters: FOV = 184 × 184 mm2; voxel dimensions = 1.8 × 1.8 × 1.8 mm3; number of averages = 14; data matrix = 92 × 88, obtaining 48 slices with no interslice gap. The total examination time was 7–8 minutes. We used parallel imaging and chose not to cover the whole brain, limiting the acquisition to the olfactory tracts to reduce the acquisition time.
Image Analysis
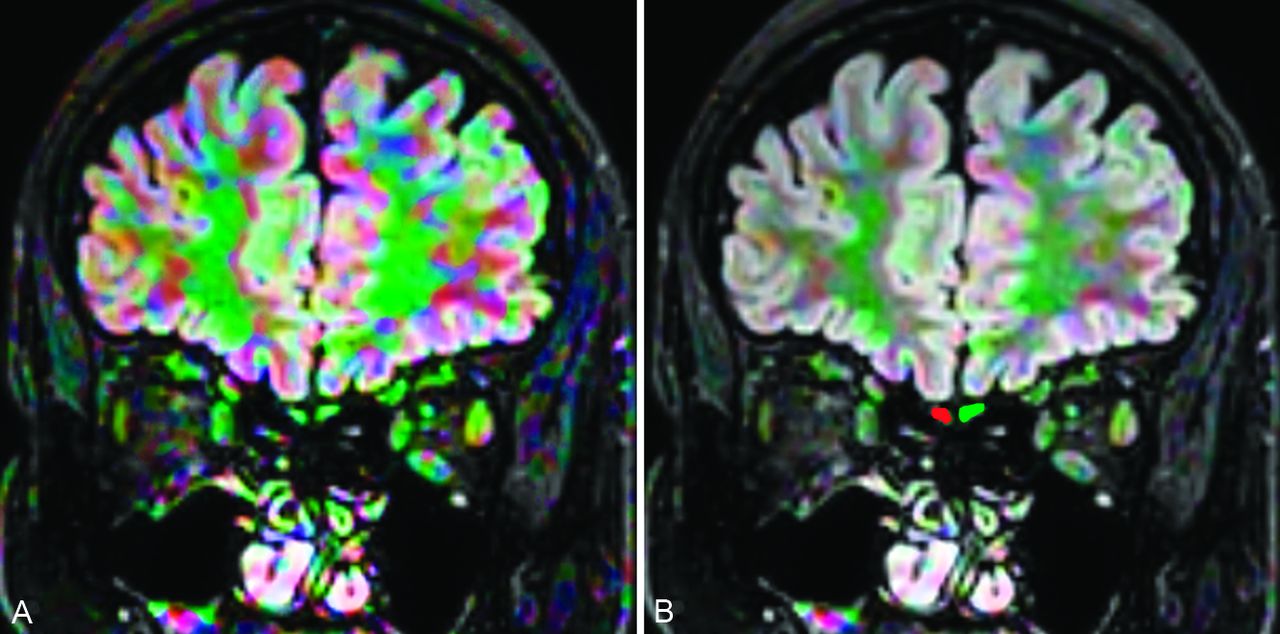
Image analysis was performed by 2 experienced neuroradiologists (F.S., M.M.G.) with 17 and 14 years of experience, respectively, who were blinded to the clinical history of the studied individuals. Images were transmitted to a workstation (Extended MR WorkSpace 2.6.3.5, Philips Medical Systems) for DTI analysis followed by precise positioning of the ROI. The FA maps were coregistered with the 3D-FLAIR images and positioned at the OB (Fig 1). MD and the FA were measured on the right and the left OBs by each reader separately. Then the mean values of the FA and MD for readings on both sides were calculated independently.

The OB in a patient with COVID-19-related anosmia. DTI of the OB with displays on the 3D-FLAIR image. The mean MD and FA of the OB values were 1.97 mm2/s and 0.18, respectively.
The OB volume was assessed by the box frame method.15 First, the number of images with clear visibility of the OB was counted. Second, the imaging having the most visibly distinct voxels for both OBs was chosen as the standard image, and the OBs were framed by a box. Furthermore, annotations were drawn between 2 extreme points of the OB box to calculate the width (w) and height (h). The length (l) was calculated by multiplying the total number of images that showed visibly distinct OBs by the section thickness. The final OB volume was calculated as w × h × l in cubic millimeters.
Statistical Analysis
The data were analyzed using SPSS 22 (IBM). Using descriptive statistics, we calculated the mean (SD) of the MD and FA. The significant differences between DTI metrics in anosmic and healthy control group were analyzed. A P value ≤ .05 was considered significant. We implemented κ statistics to calculate the interreader agreement for the estimated DTI parameters. The receiver operating characteristic curve was established, and the area under the curve was calculated to determine the cutoff point of DTI parameters used for diagnosing OB neuropathy. The cutoff point with highest sensitivity and specificity of DTI parameters was determined by the Youden index. Sensitivity, specificity, and accuracy were also registered.
RESULTS
The COVID-19 anosmic group (n = 66) consisted of 48 females and 14 males with an age range of 16−83 years (median, 37 years), while the control group (n = 23) consisted of 17 females and 6 males with an age range of 17–61 years (median, 36 years). The severity of COVID-19 ranged from mild to moderate. All patients in the anosmic group presented with a loss of smell and taste (100%); other presenting symptoms were headache (80.3%), low-grade fever (65.1%), dry cough (27.3%), dyspnea (16.6%), sore throat (46.9%), gastrointestinal symptoms (22.7%), and rhinorrhea (60.6%). The presentation of anosmia ranged from as early as the first day (24 patients) to a slightly delayed presentation within 2–5 days in the remainder of the patients. The median duration of anosmia was 60 days (range, 15–135 days). This study analyzed 124 OBs in 62 patients in comparison with 23 control individuals with 46 OBs. The Online Supplementary Data demonstrate the MD and FA of diseased and control OBs. The Online Supplementary Data show the receiver operating characteristic curve and diagnostic performance of MD and FA for diseased and control OBs.
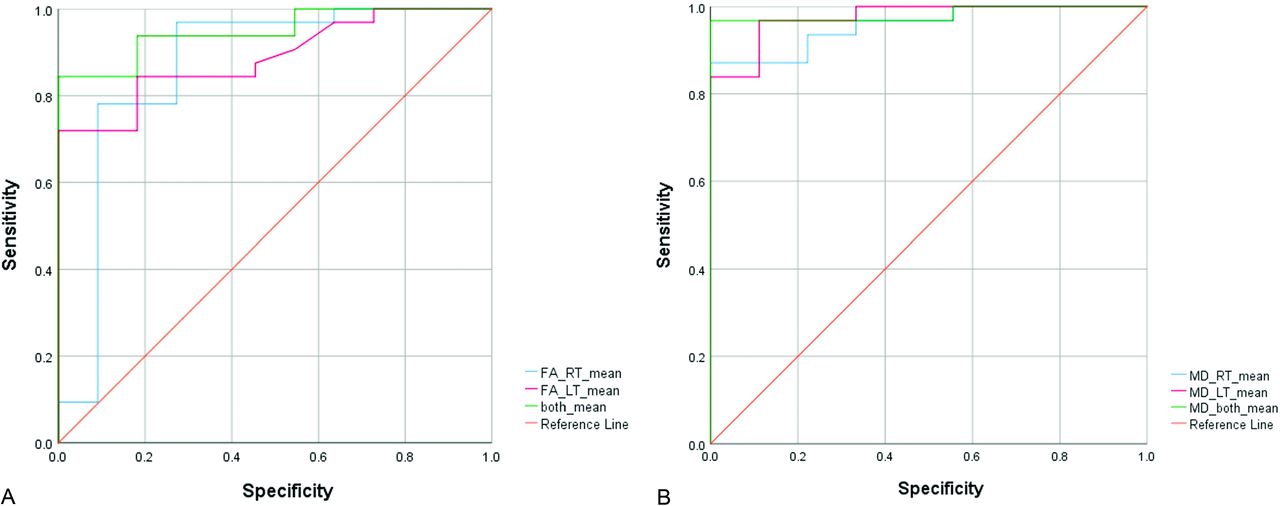
The mean OB volume calculated by the box frame method was significantly higher (P < .0001) in the anosmic group (83.6 [SD, 29.6] mm3) compared with control group (30.5 [SD, 8] mm3). The mean FA values of the 2 included groups in our study were 0.18 (range, 0.12–0.3) for diseased OBs and 0.27 (range, 0.23–0.42) for control OBs. The FA values showed significant variation between diseased and control OBs with P < .0005. The area under the curve of the mean FA to differentiate both entities was 0.949. The resulting threshold of FA to differentiate diseased from normal OBs was 0.22, with a diagnostic accuracy of 88.4%, sensitivity of 84.4%, and specificity of 100% (Fig 2A). The mean MD value of the diseased OBs was 2.3 (range, 1.3–3) and of control OBs, 1.4 (range, 1–1.5) ×10−3mm2/s. A significant difference between MD values of diseased and control OBs was demonstrated with P < .0005. The under the curve of the mean MD to differentiate both entities was 0.982. The resulting threshold of MD to differentiate diseased from normal OBs was 1.51, with a diagnostic accuracy of 97.5%, sensitivity of 96.8%, and specificity of 100% (Fig 2B). The diagnostic performance of these cut off values was excellent when tested on 30% of the sample which was chosen at random.

{kind=link}
{kind=link}
Receiver operating characteristic curves of FA (A) and MD (B) used for differentiation of a diseased and normal OB by both readers. RT indicates right; LT, left.
In a secondary analysis, we compared the DTI parameter between patients with COVID-19 and anosmia having sinus disease (26/62) with other patients negative for sinus disease (36/62). There was no significant difference (P = .6) in mean FA between positive and negative groups (0.17 [SD, 0.02] and 0.18 [SD, 0.05], respectively). Similarly, there was no significant difference (P = .6) in mean MD between both groups (2.3 [SD, 0.7] and 2.2 [SD, 0.4] ×10-3mm2/s, respectively). The results demonstrated excellent interobserver agreement between both readers using FA and MD in sorting the OBs of diseased and control individuals (κ = 0.915 and 0.892, respectively).
DISCUSSION
In the current study, DTI with its unique parameters (MD and FA) revealed a noteworthy significance in differentiating patients with COVID-19 and anosmia from control individuals. Moreover, an excellent interobserver agreement of the MD and FA readings was obtained denoting the consistency of their significance. The impact of the MD values of the OB in patients with anosmia must be highlighted because it varied greatly from values of the control group, being much higher in subjects with anosmia. This finding is a mere reflection of the inflammatory edema in the virally infected OBs. This could be a long-lasting sequala, even after the subsidence of the COVID-19 viral infection. It also concurs with studies reporting improvement of the smell sensation after topical and systemic corticosteroid therapy.16 On the other hand, the FAs of the OBs were significantly less than those in the control group. On the basis of our results, MD was introduced as a more powerful differentiating parameter than FA, as the difference in MD values between the 2 groups was more evident than the difference between the 2 groups regarding the FA values. This finding could be attributed to the relative preservation of the intercellular anisotropy. Similar results were reported by Taha et al,13 who reported a significantly lower FA in 11 patients with anosmia and 3 with hyposmia secondary to chronic sinonasal polyposis compared with the control group. Another study reported changes in the DTI parameters in Parkinson disease and showed significant FA reduction (P < .05) for the hyposmic Parkinson disease group compared with controls.12 Moreover, Güllmar et al11 reported improvement in the results of olfaction tests and the DTI parameters measured in the olfactory pathway, including the OBs after functional endoscopic sinus surgery.
The persistent prolonged rise of MD after recovery from SARS-COV-2 infection is suggestive of an extended inflammatory process, even after the subsidence of other COVID-19 symptoms. This inference could be supported by the results of the study of Lu et al,17 in which MR imaging was performed 3–4 months after SARS-COV-2 infection. Their MR volumetric analyses reported significantly increased gray and white matter volumes compared with those of control noninfected individuals. Lee et al18 performed MR microscopy, histopathologic evaluation, and immunohistochemical analysis of postmortem brain and olfactory bulbs for patients who died from COVID-19 and found multifocal microvascular injury without evidence of viral infection. These data may explain the changes observed on DTI parameters of the OBs in patients with anosmia and COVID-19.
The current study had some drawbacks. The relatively limited number of patients included in both groups is a shortcoming. Future studies comprising a greater number of patients might yield more applicable results. Moreover, this study was conducted using DTI metrics solely, without correlation between the volume calculation and signal intensity alteration. A more thorough investigation highlighting multiparametric MR imaging parameters including quantitative volumetry, signal intensity analysis, and other clinical tests for olfaction is recommended.
CONCLUSIONS
DTI parameters are valuable noninvasive quantitative tools that could help in diagnosis of the OB dysfunction in COVID-19-related anosmia.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
Indicates open access to non-subscribers at www.ajnr.org
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- Received January 10, 2022.
- Accepted after revision May 22, 2022.
- © 2022 by American Journal of Neuroradiology