Abstract
BACKGROUND AND PURPOSE: Few articles in the literature have looked at the diameter of the optic nerve on MR imaging, especially in children, in whom observations are subjective and no normative data exist. The aim of this study was to establish a data base for optic nerve diameter measurements on MR imaging in the pediatric population.
MATERIALS AND METHODS: This was a retrospective study on the MR imaging of pediatric subjects (younger than 18 years of age) at the Department of Diagnostic Radiology at the American University of Beirut Medical Center, Beirut, Lebanon. The optic nerve measurements were obtained by 3 raters on axial and coronal sections at 3 mm (retrobulbar) and 7 mm (intraorbital) posterior to the lamina cribrosa.
RESULTS: Of 211 scans of patients (422 optic nerves), 377 optic nerves were measured and included. Ninety-four patients were female (45%) and the median age at MR imaging was 8.6 years (interquartile range, 3.9–13.3 years). Optic nerves were divided into 5 age groups: 0–6 months (n = 18), 6 months–2 years (n = 44), 2–6 years (n = 86), 6–12 years (n = 120), and 12–18 years (n = 109). An increase in optic nerve diameter was observed with age, especially in the first 2 years of life. Measurements did not differ with eye laterality or sex.
CONCLUSIONS: We report normative values of optic nerve diameter measured on MR imaging in children from birth to 18 years of age. A rapid increase in optic nerve diameter was demonstrated during the first 2 years of life, followed by a slower increase. This was independent of sex or eye laterality.
The optic nerve anatomically starts from the optic disc and ends in the optic chiasm and comprises 4 distinct parts: the optic nerve head, the intraorbital portion, the intracanalicular portion, and the intracranial portion.1⇓–3 Just posterior to the sclera, the nerve acquires arachnoid membranes continuous with those of the brain,4 composing the optic nerve sheath complex. While fundoscopy and optical coherence tomography can study the disc portion with high resolution, the remaining 3 portions are less accessible and require imaging studies, including MR imaging, sonography, and CT.5,6 In fact, MR imaging is superior due to its high soft-tissue resolution, the absence of ionizing radiation, and its high diagnostic accuracy as demonstrated by several studies evaluating the sensitivity of MR imaging compared with histopathologic examination in the detection of tumor invasion.7⇓–9 According to Chawla et al7 and Schueler et al,8 the MR imaging sensitivity in detecting optic nerve abnormality is 60%–75%, while its specificity is up to 90%. Indeed, the optic nerve has been studied in healthy individuals and in pathologic states using MR imaging, CT, sonography, and cross-sectional anatomy.10⇓⇓⇓–14 These studies, however, have reported either qualitative parameters5,15 or normative values of both the optic nerve and sheath as a complex.16⇓⇓–19
Ample literature exists on the use of MR imaging to classically describe the optic nerve sheath diameter, which has been associated with increased intracranial pressure from various causes like trauma, brain tumors, and idiopathic intracranial hypertension. Such studies are not sensitive to the optic nerve itself because measurements include the sheath, CSF, and optic nerve. Measurements of the optic nerve diameter have historically been difficult, due to problems in the methodology to be adopted, such as the differing appearance of the nerve sheath in the various MR imaging sequences and the width, which differs from anterior to posterior. With the use of new volumetric methods, thin-cut images, and the availability of fat-suppression sequences, such measurements can be accurately performed. Few articles in the literature have looked at the diameter of the optic nerve proper on MR imaging, especially in children, in whom observations are subjective and no normative data exist. Pathologic changes in the diameter of the optic nerve itself are not uncommonly encountered in different disease entities affecting the pediatric population, including optic nerve hypoplasia or atrophy, Leber optic neuropathy, multiple sclerosis, and optic nerve enlargement, such as from gliomas in neurofibromatosis type 1.4,10,20⇓⇓–23 Measuring the optic nerve proper is essential to the diagnosis of such entities.
Our study aimed to report normative values for the optic nerve diameter on MR imaging in the pediatric population and examine its development across different age groups to generate a set of objective measurements for use by radiologists and ophthalmologists.
Materials and Methods
Patient Selection
This was a retrospective review conducted at the Department of Diagnostic Radiology at the American University of Beirut Medical Center in Beirut, Beirut, Lebanon. The study was approved by the institutional review board, and informed consent was waived. We performed a thorough search on the institutional PACS for scans of patients younger than 18 years of age at the time of acquisition who underwent any MR imaging of the head and/or orbit with or without contrast enhancement between January 2010 and December 2015. Patients were divided into 5 age groups: younger than 6 months, 6 months to 2 years, 2–6 years, 6–12 years, and 12–18 years. We then reviewed patient charts and applied the following exclusion criteria: history of any brain or orbit tumor, enucleation of 1 eye, optic nerve lesions, enlargement or atrophy of the optic nerve, raised intracranial pressure (treated or not), and ischemia, hemorrhage, or atrophy along the optic pathway. We included patients who had indications for MR imaging other than optic nerve lesions, such as seizures and epilepsy, neck mass investigation, temporal bone abnormality, developmental delay, recurrent headaches, and others. Scans with poor visualization of the optic nerve were excluded.
MR Imaging Measurements
All MR images were performed on the Ingenia 3T or 1.5T systems (Philips Healthcare, Best, the Netherlands). The brain and orbit MRIs were performed with a 16-channel head coil. The sequences analyzed consisted of 2-mm sections. A T1-weighted inversion recovery sequence in the axial and coronal plane was performed with the following parameters: TR range = 5000–7000 ms, TE range = 15–30 ms, TI = 400 ms, matrix size range = 168 × 100 to 212 × 130, FOV range = 180 × 180 mm to 230 × 230 mm, section thickness/spacing range = 2–0.3 to 2–0.5 mm, acquisition time = 5 minutes 16 seconds; and an orbit-dedicated STIR sequence in the axial and coronal planes was performed with the following parameters: TR range = 2240–2650 ms, TE range = 80–90 ms, TI = 200 ms, matrix size range = 256 × 195 to 320 × 255, FOV range = 200 × 200 mm to 250 × 250 mm, section thickness/spacing range = 2–0.3 mm to 3–0.3 mm, acquisition time = 2–3 minutes. The axial images were obtained parallel to the intraorbital portion of the optic nerve, and the coronal images were placed on the sagittal cuts perpendicular to the optic nerves.
Image analysis and measurements were performed by a trained cognitive neuroscientist (R.N.T.), a senior radiology resident (M.G.S.), and a neuroradiologist (R.G.H.) using OsiriX Imaging Software (http://www.osirix-viewer.com) on a high-resolution monitor. The measurements were obtained on axial and coronal sections at 3 and 7 mm posterior to the lamina cribrosa. Measurements at 3 mm were retrobulbar, and measurements at 7 mm were at the midaspect of the intraorbital segment of the optic nerve (Fig 1). These 2 loci were chosen to examine whether the midaspect is smaller than the retrobulbar portion of the optic nerve. For every patient, each eye was treated individually. In some cases, on the axial or coronal cuts, 1 optic nerve was used for measurements, while the second one was not clearly delineated.

Axial (A) and coronal STIR (B) images of the orbits. An example of our measurement method. The optic nerve is measured without the nerve sheath, 3 (a) and 7 (b) mm posterior to the lamina cribrosa. It is also measured on the coronal plane (c) at the same 2 locations: retrobulbar and midaspect.
Statistical Analysis
All statistical analyses were performed with STATA 13 (StataCorp, College Station, Texas). The results were reported as mean ± SD. Interrater agreement was evaluated with intraclass correlation coefficients and corresponding 95% confidence intervals to ensure reliability and reproducibility of the results. After confirming agreement among the 3 raters, we averaged the measurements. Data normality was assessed by the Shapiro-Wilk test for normality coupled with visual inspection of the data via histograms. Accordingly, differences between the right and left eyes were evaluated using the paired Student t test or Wilcoxon signed rank test, and between-sex differences, with the unpaired t test or Mann-Whitney U test. ANOVA testing was performed to reveal between-group differences with a Šídák correction for multiple comparisons for more detailed results on confidence intervals and significances between each age group. Finally, measurement results were plotted versus age, and Pearson or Spearman correlation coefficients were calculated.
Results
Two hundred eleven scans of patients were collected for measurement. The median age at MR imaging acquisition was 8.6 years (interquartile range, 3.9–13.3 years), and 94 (45%) patients were females. Interrater agreement was excellent, with an intraclass correlation coefficient of 0.842 (95% CI, 0.821–0.861; P < .001). The agreement between the readers for the patients younger than 6 months of age and children between 6 months and 2 years was good as well (intraclass correlation coefficient = 0.82; 95% CI, 0.579–0.931; P < .001; and intraclass correlation coefficient = 0.766; 95% CI, 0.693–0.823; P < .001, respectively).
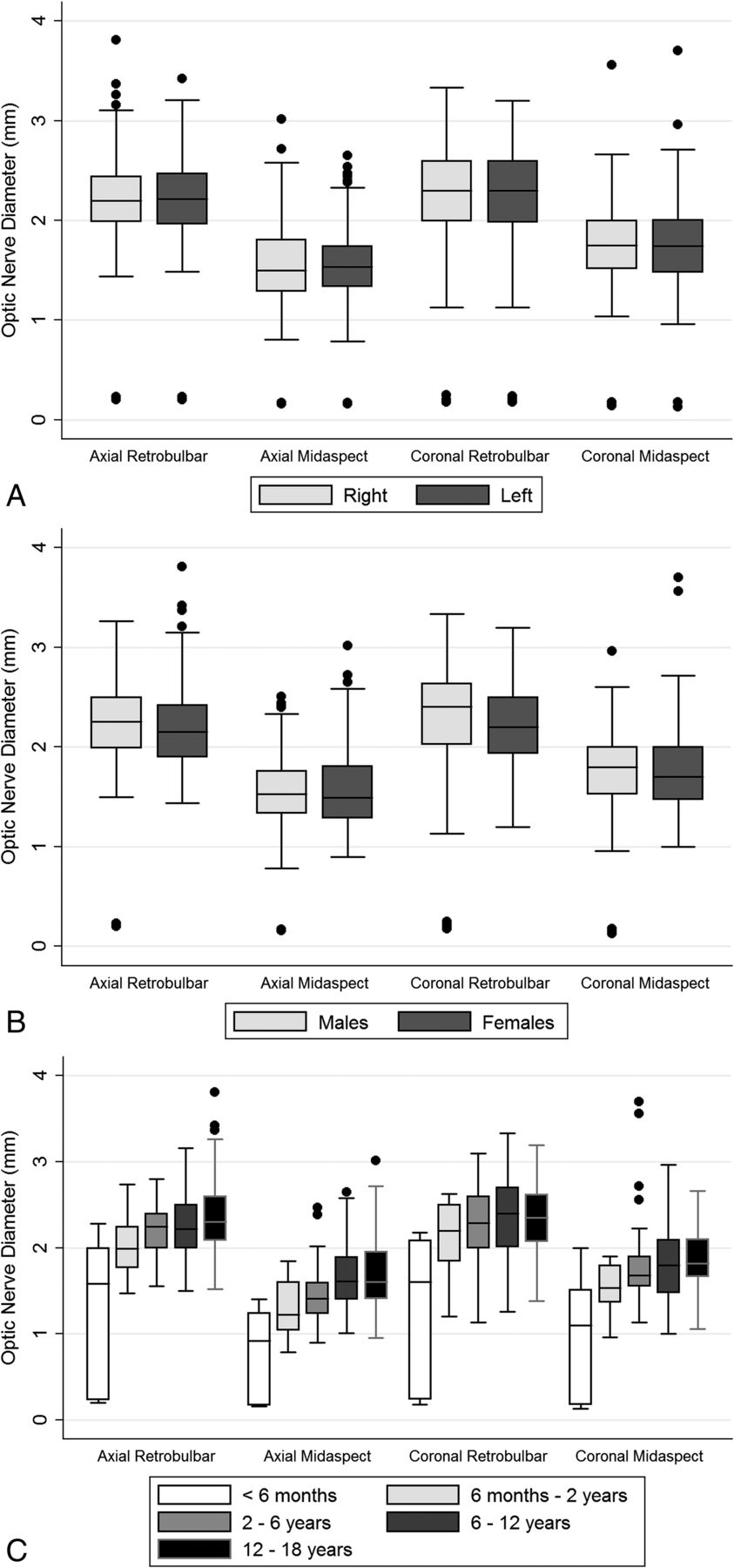
Table 1 shows the optic nerve measurements on MR imaging at the retrobulbar and midaspect levels for each of the axial and coronal cuts. Optic nerve diameter measurements did not differ between the right and left eyes (Fig 2A) or between males and females (Fig 2B), regardless of the section and location of the measurement. However, the optic nerve significantly increased in diameter across age groups, which was also observed in all measurements (Fig 2C). At the axial cut, the mean diameter steadily increased with the age from 1.35 ± 0.82 mm among patients younger than 6 months up to 2.26 ± 0.38 mm and 2.35 ± 0.40 mm for patients between 6 and 12 years of age and between 12 and 18 years, respectively on the retrobulbar level (Table 2). Similarly, in the axial cuts, the mean diameter of the optic nerve increased with age from 0.73 ± 0.55 mm among patients younger than 6 months up to 1.67 ± 0.36 mm for patients between 6 and 12 years of age and between 12 and 18 years of age and to 1.67 ± 0.40 mm between 12 and 18 years of age on the midaspect level.
Optic nerve diameter at each of the retrobulbar and midaspect locations on axial and coronal MRI sections

Optic nerve diameter measurements (millimeters) at each of the retrobulbar and midaspect locations on the axial and coronal MR imaging sections, according to eye laterality (A), sex (B), and age group (C).
Optic nerve diameter measurements at each of the retrobulbar and midaspect locations on axial and coronal MRI sections
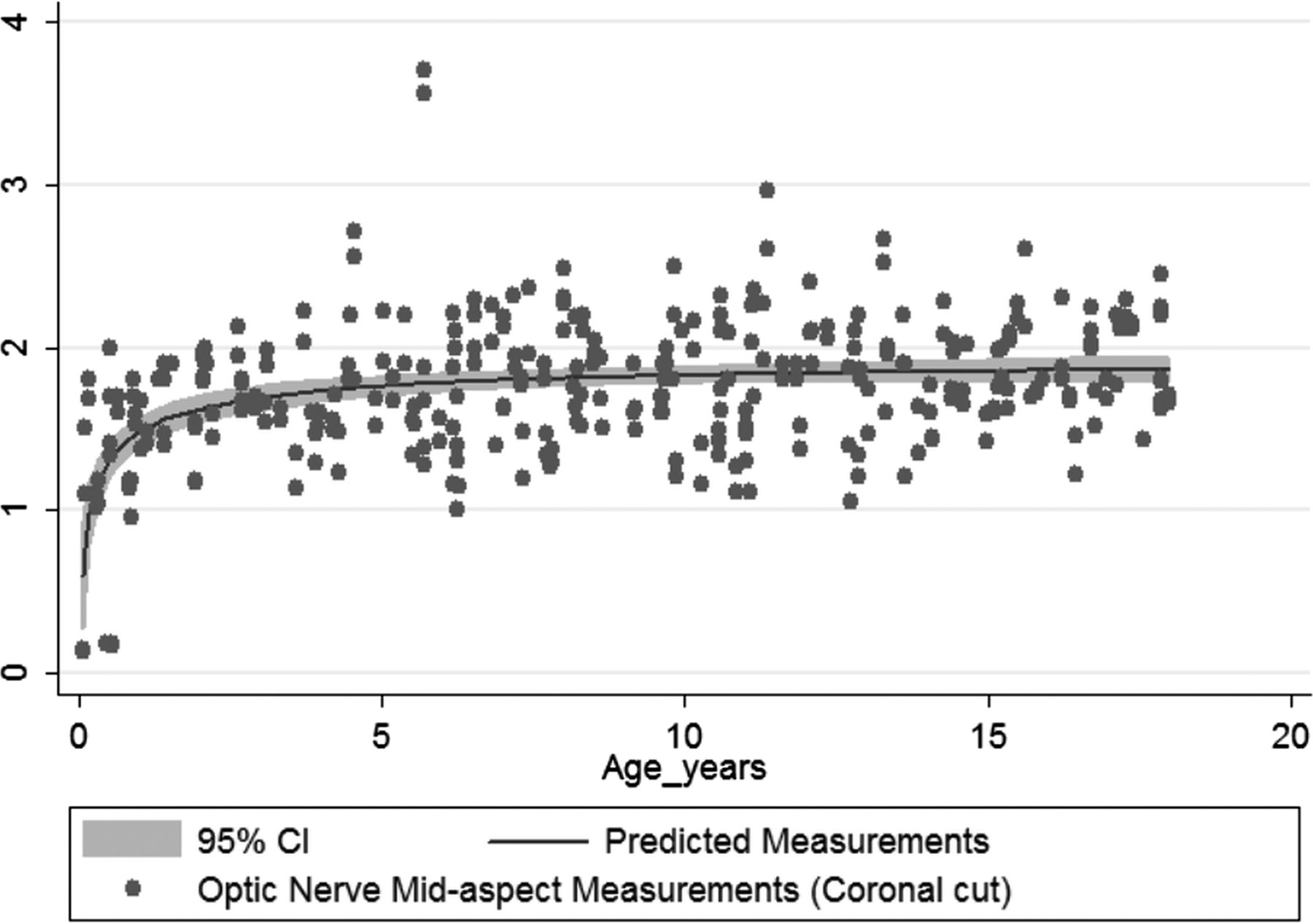
Significant between-group differences for all 4 measures were observed on 2 by 2 comparisons (Table 3). The results were then plotted in a measurement-versus-age comparison. The graphs show a steep increase in diameter in the first 2 years, after which the curve plateaus; this finding applied to both axial and coronal measurements and at the 2 loci, retrobulbar and midaspect. The most representative graph, obtained from midaspect measurements on the coronal cut plotted against age, is shown in Fig 3.
Two by 2 group comparisons of the optic nerve diameter measurements on different scans

{kind=link}
{kind=link}
{kind=link}
Optic nerve midaspect diameter growth with age on a coronal cut.
Most interestingly, there was a consistent difference in optic nerve diameters between the midaspect and retrobulbar portions, which was observed on both axial and coronal images and in most age groups.
Discussion
In this study, we report normative values of optic nerve diameter measured on MR imaging in children from birth to 18 years of age, dividing them into 5 age groups: 0–6 months, 6 months–2 years, 2–6 years, 6–12 years, and 12–18 years. Our results showed significant between-group differences in measurements, with a rapid increase in optic nerve diameter demonstrated during the first 2 years of life, followed by a slower increase to the 6 years of age with no significant change later. This was independent of sex or eye laterality.
Despite the technical challenges in the pediatric population, MR imaging was reliable in quantitatively assessing the size of the optic nerve proper. Multiple other studies have confirmed this finding with MR imaging for the diagnosis and early detection of optic nerve hypoplasia in children.18,22,24⇓⇓–27 However, there was no standardized method to obtain these measurements; thus, cross-study comparisons could not be performed accurately. Also, while there are reports on MR imaging measurements in healthy children, they focused on the optic nerve sheath complex as a whole and not the optic nerve itself.19,28 Therefore, there is a need to establish a standardized method for the measurement of the optic nerve on MR imaging in the pediatric population. These patients are at risk of multiple disease entities affecting the optic nerve,29 such as optic nerve hypoplasia or atrophy, optic neuritis,30,31 optic neuropathies,32 and other associated optic nerve pathology with failure to thrive.33 Objective assessment by MR imaging will aid in earlier and more accurate diagnoses of these various disorders in this vulnerable population.
Several studies have assessed the optic nerve sheath using various imaging modalities. This was mainly done to establish a normative data base in adults,5,10⇓⇓⇓–14,27,28 or to use the optic nerve sheath complex as a surrogate to diagnose increased intracranial pressure. The latter outcome was studied both in children and using sonography, CT, or MR imaging and in different clinical settings.19,34⇓–36 In fact, MR imaging proved to be superior to high-resolution ultrasonography and CT in demonstrating optic nerve measurements without the risks of exposure to ionizing radiation.11,27,37
Our results show that most of the optic nerve growth occurs in the first 2 years of life, which is in accordance with other published data regarding the early development of the optic nerve. In fact, the optic nerve increases in size in utero to reach normal neonate size at 36 weeks of gestation38; then, it continues to grow up to 2 years of age and less rapidly thereafter according to histologic studies.39,40 Ophthalmologists and radiologists ought to be aware of this finding while interpreting MR imaging scans in various clinical scenarios in infants with early signs of cerebral palsy, developmental delays, delayed visual maturation, and poor visual behavior/fixation. Hence, it is important to obtain normative measurements of the optic nerve diameter in the pediatric population; these measurements are very sensitive to age, especially in the first 2 years of life. Our data are also in agreement with other literature in that there was no laterality or sex differences in optic nerve thickness on MR imaging.41 The midaspect portion of the optic nerve would be expected to be thinner than the retrobulbar portion on both axial and coronal cuts, consistent with our reported results. This is a consequence of the optic nerve itself becoming more organized as it acquires its sheath traveling posteriorly through the narrow bony orbit.1,2
There are some limitations to this study. The relatively small sample size, particularly in the group of subjects younger than 2 years of age, could potentially affect the measurements. Moreover, these patients often require the administration of sedatives or general anesthesia, which may deviate their eyes from the primary position and may induce motion artifacts, which could explain the differences in measurement seen with changes in eye position and axial-versus-coronal cuts. The coronal cuts of the orbits were not obtained perpendicular to the axis of each optic nerve separately; this feature partly explains the difference in the measurements between the axial and coronal sections. Last, a prospective study with thorough general medical, neurologic, and ophthalmologic assessment of pediatric subjects before undergoing a standardized MR imaging examination of the orbit using the measurement criteria presented in this article is needed to confirm our findings.
Conclusions
We report normative values of the optic nerve diameter measured on MR imaging in children from birth to 18 years of age. A rapid increase in optic nerve diameter was demonstrated during the first 2 years of life followed by a slower increase. Our measurements can give radiologists and neuroscientists a reliable reference to diagnose optic nerve abnormalities in children.
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.
- 41.
- Received May 23, 2017.
- Accepted after revision September 13, 2017.
- © 2018 by American Journal of Neuroradiology