Abstract
SUMMARY: We report the case of an early ISR that was due to platelet aggregation despite correct observance of a standard antiplatelet regimen. Biologic testing showed clopidogrel inefficiency, and ISR disappeared on angiography after a loading dose of clopidogrel. This result suggested that the arterial lumen reduction was due to platelet aggregation rather than in-stent myointimal hyperplasia. This observation emphasizes the importance of verifying the efficacy of clopidogrel before placing a stent.
Abbreviations
- AP
- anteroposterior
- CTA
- CT angiography
- ISR
- in-stent restenosis
- MCA
- middle cerebral artery
- TCD
- transcranial Doppler
- TIA
- transient ischemic attack
- VASP
- vasodilator-stimulated phosphoprotein.
ISR is a well-known delayed event in coronary interventions. With the expansion of intracranial stent placement, ISR has been recognized in some series up to 30%.1–3 The admitted mechanism of ISR is myointimal hyperplasia. This led, in the cardiologic field, to the development of a drug-eluting stent whose purpose was to inhibit arterial wall cell proliferation. We present an observation that tends to question this unique mechanism. In-stent platelet aggregation may have the same imaging presentation as ISR. Therefore, verifying the efficacy of antiplatelet treatment becomes more and more crucial.
Case Report
A 46-year-old man, a current smoker with a history of untreated hypertension, presented to the emergency department with a recent history of multiple TIAs characterized by 2 episodes of transient left hemiparesis lasting for 15 minutes. TCD and MR angiography revealed the presence of a tight stenosis of the right MCA, which was confirmed by conventional angiography (Fig 1). Despite the administration of clopidogrel, aspirin, and unfractioned heparin, the patient had recurrent symptoms with a new lesion on MR imaging (diffusion-weighted imaging hypersignal) at the junction of the anterior cerebral and MCA vascular territories. Emergency angioplasty and stent placement were performed with a favorable clinical outcome. Two loading doses of 300 mg of clopidogrel were given in 8-hour intervals. The patient was treated in the emergency department the day after this administration. Intervention was performed with a balloon angioplasty of 2-mm diameter (Gateway PTA balloon catheter; Boston Scientific, Fremont, California) followed by the implantation of a Wingspan stent (2.5 × 9 mm; Boston Scientific, Natick, Massachusetts). The control angiogram showed restitution of a normal arterial lumen diameter (Fig 2). At that time, a VASP test was performed showing the efficacy of clopidogrel. The patient was discharged with the usual 75-mg dose of clopidogrel and 160 mg of aspirin.

Conventional angiogram (AP view) shows a tight short stenosis of the M1 segment of the right MCA (arrow).

Conventional angiogram (AP view) shows the lumen restitution of the M1 segment of the right MCA after stenting.
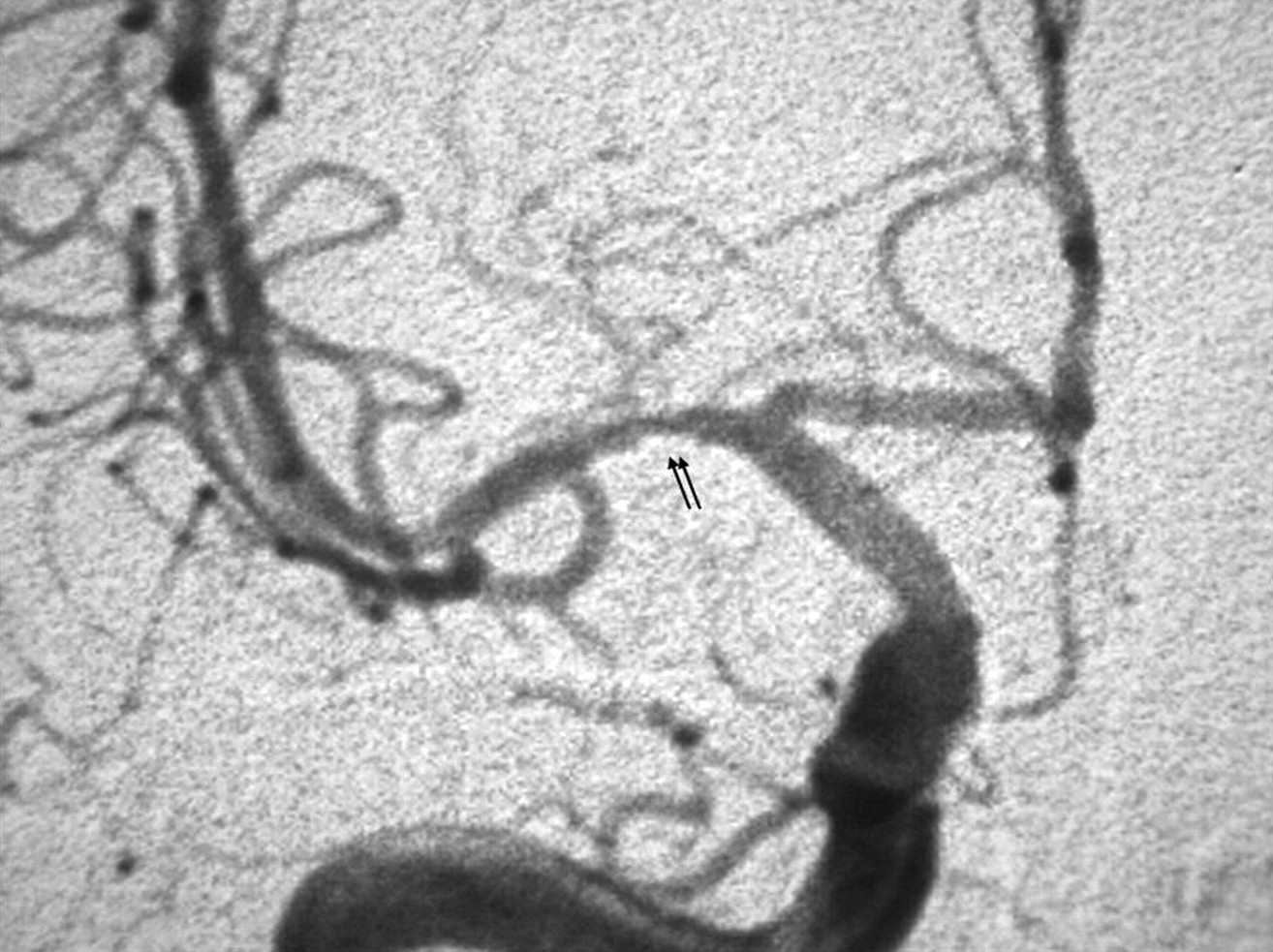
Three months after the procedure, a systematic TCD revealed elevated velocities in the right MCA (mean systolic velocities, 217 cm/s), suggesting ISR. The angiogram confirmed a 50% MCA in-stent lumen reduction (Fig 3). This event occurred when the patient was still receiving aspirin and clopidogrel. At this time, the patient was asymptomatic but was scheduled for an endovascular treatment due to the recurrence of this early ISR. Biologic testing (aggregometry) showed clopidogrel inefficiency; and as a consequence, 2 loading doses of 300 mg of clopidogrel were given. The findings of the angiogram obtained the day after the loading dose were normal without any in-stent lumen reduction (Fig 4). The patient was discharged with a daily dose of 150 mg of clopidogrel. Further control of VASP showed good efficacy. Control TCD showed normal velocities of the MCA within a follow-up of 18 months.

Conventional angiogram (AP view) shows in-stent lumen reduction 3 months after stenting (double arrow).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Conventional angiogram (AP view) shows normalization of the in-stent lumen after a loading dose of clopidogrel.
Discussion
ISR is not an uncommon evolution after intracranial stent placement and is, in general, considered as myointimal proliferation.2 However, to our knowledge, data regarding patient platelet aggregation status are not available in published studies. The identification of an in-stent lumen reduction may be sometimes challenging, and the mechanism of the stenosis is a critical issue. Therefore, other differential diagnoses, such as in-stent platelet aggregation, should be considered, as illustrated in this case. In-stent platelet aggregation was initially misdiagnosed and thought to be an ISR. Noninvasive imaging techniques and conventional angiography were not relevant for identifying the real mechanism of in-stent lumen reduction. As shown in this case, in-stent platelet aggregation should be ruled out in patients with increased velocities after intracranial stent placement. This point is crucial because the usual antiplatelet regimen (75-mg clopidogrel and aspirin) may be insufficient in up to 40% of patients.4
The concept of resistance to clopidogrel or aspirin has been debated, given the fact that some patients are low responders and may be inadequately classified as being resistant. Additionally, poor platelet inhibition may be related to noncompliance, inadequate dosing, or absorption.5,6 In coronary patients undergoing stent placement, aspirin and clopidogrel resistance have been reported,7,8 but the therapeutic management of this condition is not clearly established. Double-antiplatelet therapy in intracranial arteries has been extrapolated from the coronary stent placement practice, but data regarding aspirin and clopidogrel regimens among patients who undergo intracranial stent placement are lacking. Some groups have reported that in intracranial stent placement, nearly 50% of the patients might be low responders to clopidogrel, whereas aspirin resistance appears to be an uncommon condition.9 Furthermore, diabetes and age older than 55 years have been identified as predictors of low response to clopidogrel. Although there are no data regarding the beneficial effect of a loading dose of clopidogrel, in our patient, the dose of 300 mg of clopidogrel was associated with in-stent lumen reduction disappearance. The long-term intracranial bleeding risk of high doses of clopidogrel remains unknown and may hamper the expected benefit of such antiplatelet regimen.
The inefficiency of the antiplatelet treatment may explain some ISRs that are not actually due to myointimal hyperplasia but platelet aggregation. We suggest that antiplatelet-agent resistance should be investigated before intracranial endovascular procedures to reduce per-procedural in-stent thrombosis or delayed in-stent lumen reduction due to thrombus formation.
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- Received May 5, 2009.
- Accepted after revision June 3, 2009.
- Copyright © American Society of Neuroradiology