Abstract
SUMMARY: We report a small cohort of patients with severe osteoporotic fractures treated with vertebroplasty. We note a high prevalence of small, central, intraosseous clefts in these severe fractures. Rather than filling the small amount of residual bone marrow around the periphery of these severe fractures, as suggested by previous authors, we suggest central needle placement to fill these central clefts.
Vertebroplasty, which is widely applied for the treatment of painful, osteoporotic fractures, is considered by some practitioners to be relatively contraindicated in cases of severe compression fractures.1–4 Severe fractures may present technical challenges in placing needles into the bone marrow space. Previous case series of vertebroplasty in cases of severe fracture have recommended lateral placement of 2 needles, to target the small amount of remaining marrow space around the periphery of the vertebral body.5–7
In this technical note, we describe an alternative treatment approach for severe vertebral compression fractures. For the purposes of this study, we define “severe” compression fracture as vertebrae with complete loss of height of the central aspect of the vertebral body. In the proposed alternative treatment approach, care should be taken to identify on pretreatment imaging the presence of small, intravertebral fluid cavities, commonly associated with vertebral osteonecrosis.8,9 Notwithstanding the complete loss of central vertebral body height, we recommend central needle placement in hopes of filling the small, intravertebral cleft. We present technical features and clinical outcomes in a small cohort of patients with severe vertebral compression fractures who were treated with vertebroplasty.
Patients and Technique
Institutional review board approval was obtained for this study. A retrospective review was made of a vertebroplasty data base consisting of more than 700 patients treated between February 1999 and July 2007, to identify patients with severe compression fractures who were treated with vertebroplasty. Some of these patients had been previously included in a report of our complete vertebroplasty experience but were not separately analyzed.10 We define severe compression fracture as vertebrae with complete loss of height of the central aspect of the vertebral body. Our definition of complete collapse is that there is essentially no more height to be lost in the body. However, there still remain thin regions of fluid or air between the endplates. We identified 11 patients with 12 severe compression fractures who had undergone vertebroplasty between July 2003 and May 2007. Preprocedure imaging in these patients included plain radiographs and MR imaging of all patients and CT in 1 patient. We define the presence of an intravertebral cavity or cleft as follows: 1) an air-filled cavity on plain radiograph, 2) an air-filled or fluid-filled cavity on CT or MR imaging, or 3) a filling pattern during vertebroplasty compatible with preexisting cleft, in which globular filling is obtained.
In typical circumstances, a transpedicular approach was performed with an 11- or 13-gauge bone biopsy needle (Osteo-Site; Cook, Bloomington, Ind) under fluoroscopic guidance. The needle tip was advanced into the vertebral cleft, if noted on preprocedure imaging, or otherwise into the central aspect of the ventral portion of the compressed vertebral body (Fig 1). In 1 patient, bilateral transpedicular injections into the lateral vertebral body were performed. Cement was infused until extraosseous extravasation was noted or until cement reached the posterior one quarter of the vertebral body.

Anteroposterior and lateral plain radiographs during vertebroplasty at L3 show the tip of the 11-gauge cannula in the ventral aspect of the midline of the vertebral body. Barium-opacified cement fills a small ventral cleft and a small portion of the right lateral aspect of the vertebral body, with a small amount of extravasation through the superior endplate.
Severity of pain at rest and with activity was measured on the basis of a semiquantitative pain scale (0–10). A 2-hour follow-up by the treating neuroradiologists as well as follow-up telephone interviews conducted by vertebroplasty nurses at 1 week, 1 month, and 6 months after the procedure were recorded.
Results
Among our 11 patients (8 women and 3 men), 12 severe fractures were treated (8 thoracic and 4 lumbar vertebrae). Mean patient age was 75 years. All patients had osteoporotic fractures. In 3 cases, patients also had myeloma, but the treated levels showed no evidence of local myelomatous disease. Three patients had nonsevere fractures treated with vertebroplasty at the same sitting as the treatment of the severe fractures. In 7 fractures, 13-gauge needles were used and in 5 fractures, 11-gauge needles were used. Clefts were present on preprocedure MR imaging in 6 of 12 fractures (Fig 2). Among the 11 cases of patients in which central needle placement was made, clefts were filled during vertebroplasty in 9 (81%), 3 of which had no cavity on preprocedure MR imaging (Fig 3). In some cases, small clefts noted on MR imaging were noted to be large when filled with cement (Fig 4).

A, Sagittal T2-weighted MR imaging of the lumbar spine shows severe fractures at T12 and L2 with fluid-filled clefts. B, lateral plain radiographs after vertebroplasty show cement-filled clefts corresponding with clefts seen on preprocedure MR imaging shown in A.

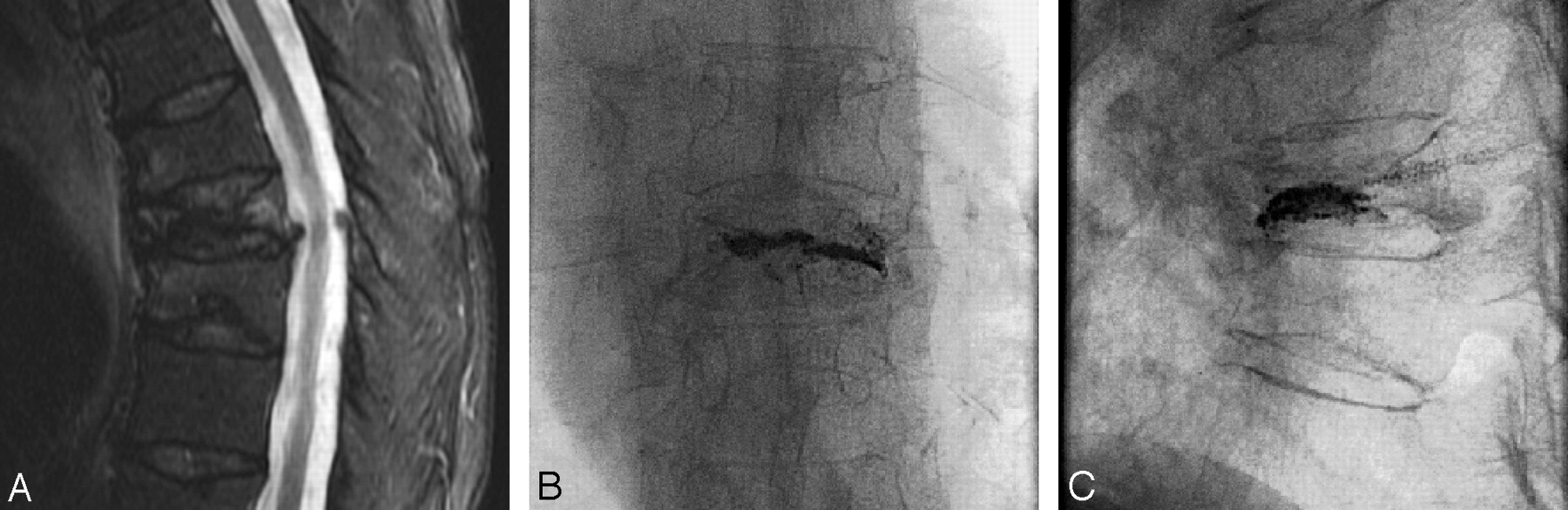
A, Sagittal T2-weighted MR imaging shows severe fracture at T8 without evidence of a cleft. B and C, Anteroposterior and lateral plain radiographs after vertebroplasty show cement filling a linear cleft.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
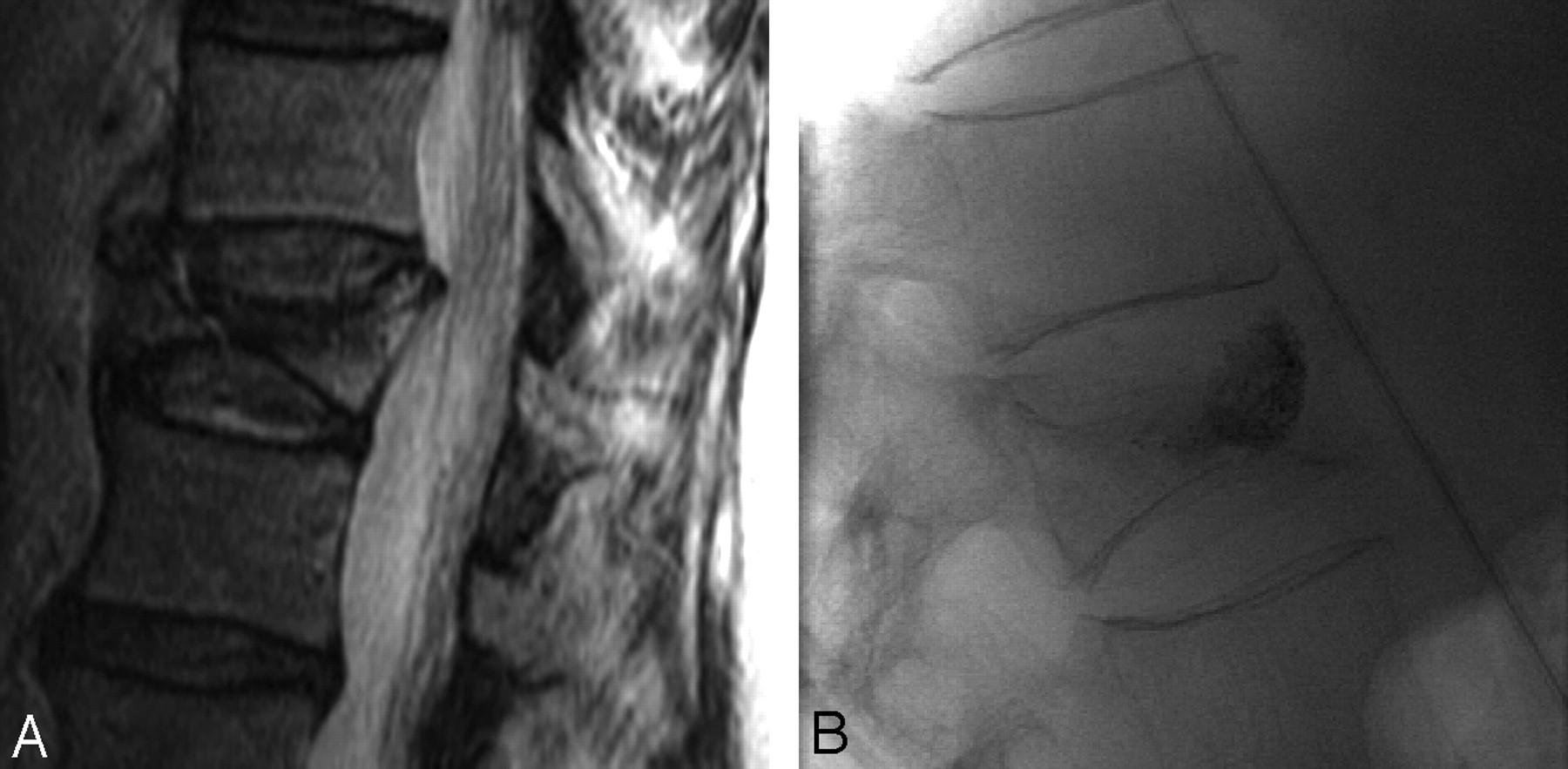
A, Sagittal T2-weighted image shows small cleft within the severe fracture at T12. B, Lateral plain radiograph after vertebroplasty shows filling of a large cleft.
The mean injected cement volume was 1.2 mL (range, 0.2–2.1 mL). Cement leakage appeared in 6 levels in very small amounts (superior endplate, 4; inferior endplate, 2) without evidence for clinical complication.
We were able to obtain follow-up in 100%, 80%, and 55% of patients at 1 week, 1 month, and 6 months, respectively. Pain before the procedure was present for a mean of 3 months (range, 1–7 months). As shown in the accompanying Table, pain relief was obtained in 90% (54% partial and 36% complete) of patients at rest and 100% (64% partial and 36% complete) of patients with activity. The single patient who indicated no improvement at 1 month was the patient who was treated with the lateral cement infusions.
Pain relief after vertebroplasty procedure
Discussion
This brief note suggests that identification and treatment of small, intraosseous clefts within severe vertebral fractures is technically feasible, safe, and is associated with good pain relief. Although only half of our cases of severe fracture showed evidence of intraosseous clefts before the vertebroplasty on MR imaging, most cases had evidence of clefts during vertebroplasty. Small amounts of cement were used, and extravasation was not problematic. Our small series may suggest not only that patients with severe fractures are good candidates for vertebroplasty, but also that unipedicular, central needle placement can render the procedure simple, rapid, and efficacious.11
Previous authors have noted good outcomes in patients with severe fractures who were treated with vertebroplasty. O'Brien et al proposed bipediculate injections with “…the trocar …placed as far laterally as possible,”5evidently to fill the residual marrow space along the periphery of the vertebral body. Although they do not mention this in their study, O'Brien et al showed 1 image (Fig 2G from O'Brien et al) in which a central cleft had been filled with cement. A large series of severe fractures Peh et al6 reported that because of “…severe central compression of the vertebra, the needle was placed more to the side of the vertebral body to decrease the chance of placing PMMA [polymethylmethacrylate] into the disk.” As with the study by O'Brien et al, the study by Peh et al shows a case with a central cleft filled with cement (Fig 3 from Peh et al), but the importance or relevance of central clefts was not discussed. In contrast to these 2 previous reports, we suggest central needle placement to fill a cleft, if present, rather than lateral needle placement.
Our study had several limitations. For one, the number of patients was small. We were unable to perform any meaningful comparison between central and lateral needle placement because we only reported a single case of a patient with lateral needle placement. It is interesting to note that this single patient had not responded well at 1 month. Furthermore, use of a relatively steep oblique lateral needle approach may have been difficult in the setting of poor imaging, inexperienced operators, or distorted anatomy. Recent release of a curved infusion cannula (AVAflex; Cardinal Health, Dublin, Ohio) might have assisted in entering small clefts by using a relatively straight anteroposterior guiding needle approach.
References
- Received October 9, 2007.
- Accepted after revision November 2, 2007.
- Copyright © American Society of Neuroradiology