Abstract
Summary: A varix occurring with a cerebral venous angioma is a rare combination of cerebral vascular malformations. The most common vascular anomaly associated with a venous angioma is a cavernous angioma. We report a case of bilateral supratentorial venous angioma with 2 varices involving the angioma situated on the right frontotemporal region. Multiple subependymal veins were seen in the right supratentorial region, which joined to form multiple collector veins, which, in turn, unified into a tortuous channel in the region of the sylvian fissure and continued into venous varices.
Cerebral varices in combination with a venous angioma are very rare. Only 8 cases were reported through 1995 (1). After that, to the best of our knowledge, no case has been reported in the literature. Also, the occurrence of multiple venous angiomas is very rare. In our patient, CT demonstrated a venous varix associated with a right-sided supratentorial venous angioma. Digital subtraction angiography further delineated the presence of 2 varices associated with this venous angioma. CT and digital subtraction angiography also demonstrated a left supratentorial venous angioma in our patient. To the best of our knowledge, this is the first reported case of double supratentorial venous angiomas with the larger one associated with 2 varices.
Case Report
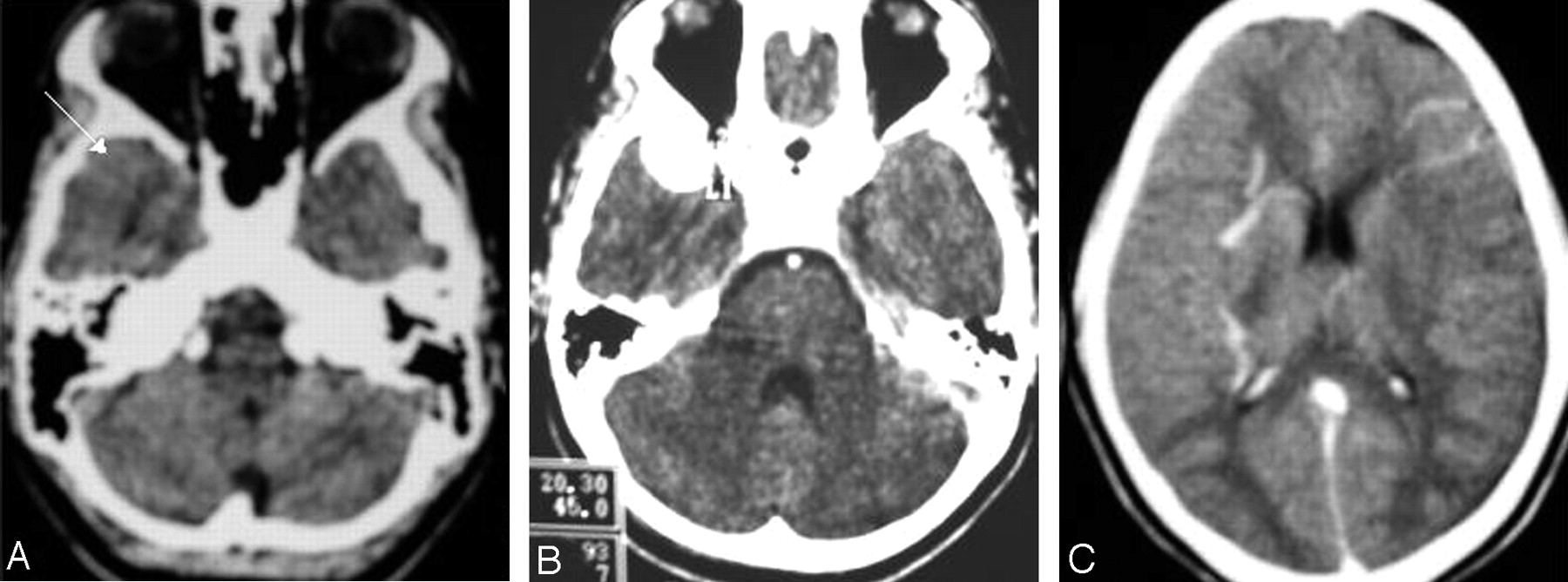
A 14-year-old girl presented with 2 episodes of generalized seizures within a week. She had no history of seizure or any other significant medical illness. Findings of her routine blood investigations, neurologic examination, and other systemic examinations were normal. Plain CT of the head showed an isoattenuated extraaxial well-defined oval lesion anterior to the right temporal pole (Fig 1A). On contrast administration, this lesion was seen to be intensely enhancing and measured 2 × 1.6 cm, which was suggestive of a vascular structure (Fig 1B). Multiple subependymal veins were seen in the right supratentorial region, which joined to form multiple collector veins, which in turn unified into a tortuous channel in the region of the sylvian fissure and continued to the region of this enhancing vascular structure, probably a venous varix. Abnormal enhancing vascular channels were also noted in the left frontal region, extending to the periphery from a subependymal location (Fig 1C). Therefore, the possibility of an arteriovenous malformation with an aneurysm or venous ectasia with dural feeders was considered. Because multiple vascular channels drained into collector veins, the possibility of a venous angioma with venous ectasia was also considered.

A, Noncontrast axial CT scan shows an isoattenuated extraaxial lesion anterior to the right temporal pole. B, Contrast-enhanced axial CT scan shows intense enhancement of the lesion. C, Contrast-enhanced axial CT scan shows multiple subependymal veins joining to form collector veins unifying into a tortuous channel in the region of the right sylvian fissure and continuing to the region of the anterior temporal enhancing extraaxial lesion. Abnormal enhancing vessels are also seen in the left frontal region.
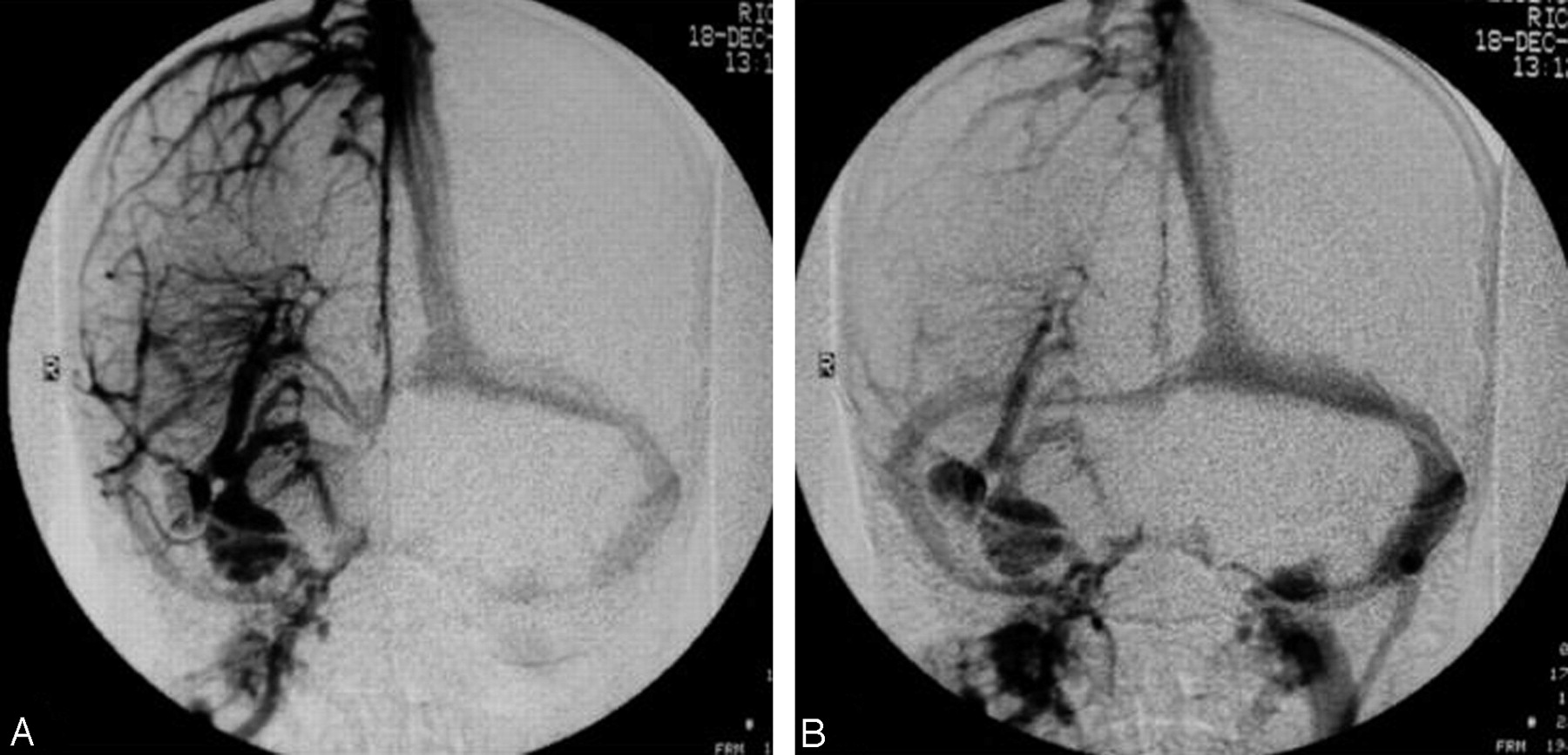
Digital subtraction angiography showed a normal arterial phase of the right internal carotid artery (Fig 2), whereas the venous phase in anteroposterior and lateral views showed multiple subependymal veins joining to form 4 collector veins, which, in turn, coursed anteroinferiorly to drain into 2 large venous varices in the region of the superficial middle cerebral vein (Fig 3, 4). These features were suggestive of a venous angioma with varices. A left internal carotid artery injection showed another supratentorial venous angioma in the frontal region, without any venous varix, that drained into the superior sagittal sinus (Fig 5). Findings in the arterial phase were normal on the left side. The posterior circulation was normal.

A, -B, Right and left internal carotid artery angiograms show a normal arterial phase.

A, -B, Anteroposterior view of early and late venous phases of the right internal carotid artery angiograms shows the presence of 2 varices and the venous angioma.

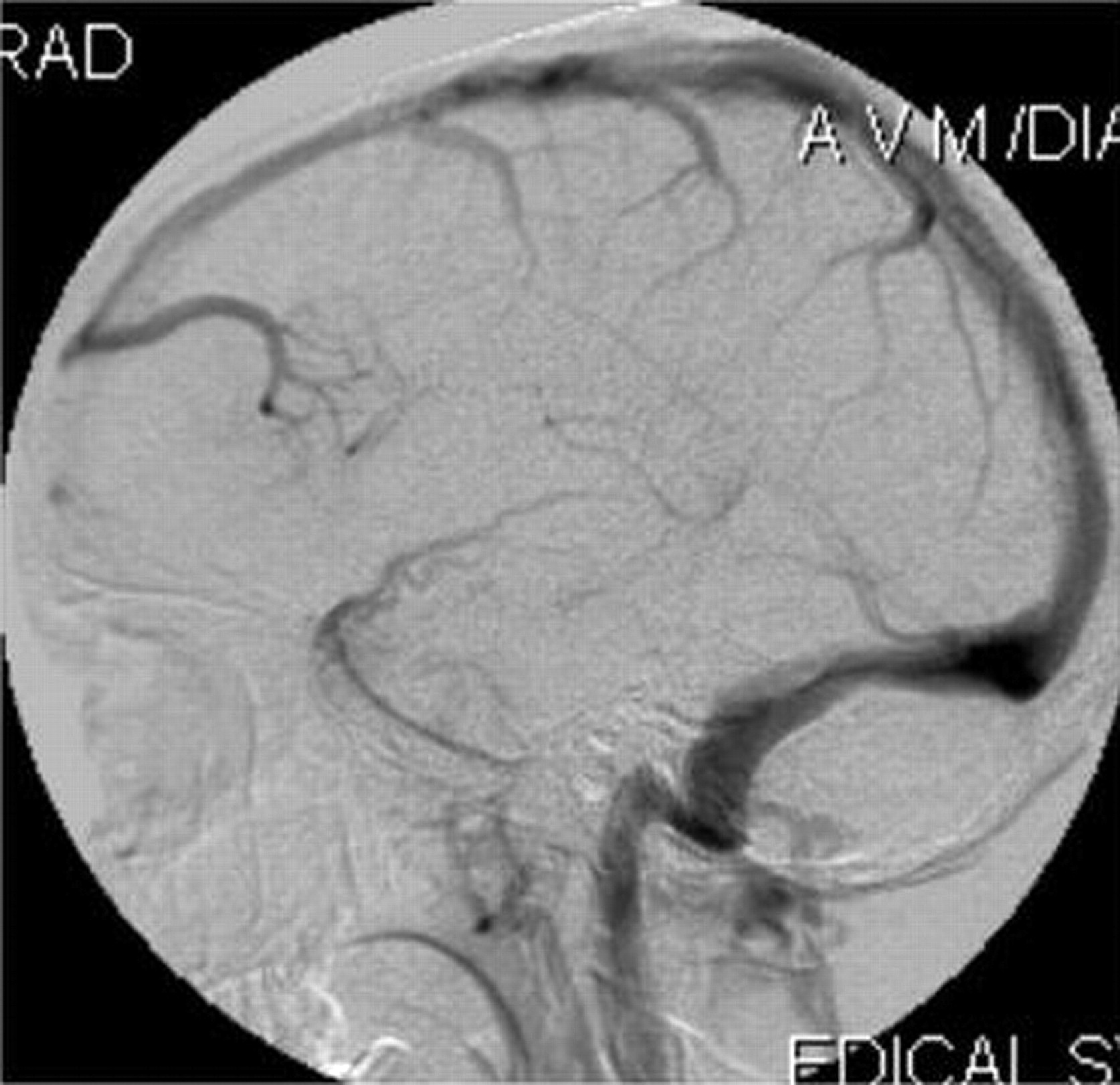
Lateral view of the venous phase of the right internal carotid artery angiogram shows a classic “Medusa head” appearance with a draining vein varix in the region of the right superficial middle cerebral vein.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Lateral view of the venous phase of the left internal carotid artery angiogram shows a classic “Medusa head” appearance draining into the superior sagittal sinus.
Discussion
Giant venous varices are a common association with an arteriovenous malformation, but a venous varix occurring in a venous angioma is very rare and only 8 cases have been reported in the literature (1). The most common vascular anomaly associated with a venous angioma is a cavernous angioma (2). Varices associated with a venous angioma occur in the draining veins of the angioma, and some case reports have shown that these varices can also bleed (3, 4).
Double supratentorial venous angiomas are rare. In 40 patients with radiologically diagnosed venous angioma, Fujii et al (5) found only one case with a double venous angioma. Garner et al (6) encountered no patient with a double lesion among his 100 patients having cerebral venous angioma. In a review of the literature of varices occurring with a cerebral venous angioma by Uchino et al (1), all 8 cases were supratentorial with varices involving the draining veins. They proposed that the increased flow in the draining vein might have increased the venous blood pressure causing a portion with a weaker wall to dilate.
Our case demonstrated 2 venous varices in the larger venous angioma involving the draining vein. Kazumata et al (7) described multiple varicose venous dilations that involved unilateral superficial cerebral veins accompanied by a varix of the internal jugular vein. Also, bilaterality of the supratentorial venous angioma associated with varices makes the present case highly unusual. Surgery is contraindicated in these patients because these venous structures drain the normal parts of the brain and surgery can result in extensive venous infarcts. There is a risk of hemorrhage especially if the patient develops focal stenosis of the terminal segment of the collector vein (8). Another potential complication is venous infarction, which may occur if the draining vein becomes thrombosed (9).
McCormick (10) categorized a pure intracranial varix as a venous malformation. Knowledge of the association of venous varices with venous angioma is essential to diagnose this combination correctly on CT or MR imaging and not to mistake it for the more common association of venous varices with an arteriovenous malformation. Digital subtraction angiography can confirm the diagnosis.
References
- Received December 26, 2004.
- Accepted after revision January 5, 2005.
- Copyright © American Society of Neuroradiology